|
In the past week, a new picture has emerged in COVID-19 data: The pandemic seems to be receding from its high-water mark in the United States. The most dependable metric of COVID-19’s spread—the number of people currently in the hospital with the disease—is in its first sustained, week-over-week decline since September, according to the COVID Tracking Project at The Atlantic. Hospitalizations fell in the past week in every state but Vermont. The number of people diagnosed with COVID-19 is falling too. New cases declined in every region of the country last week. Cases even seem to be ebbing in the coronavirus epicenters of California and Arizona, though the Sun Belt remains a hot spot. In the past two weeks, only two states—New York and Virginia—have set a single-day record for new cases. (In contrast, 13 states set a new record three weeks ago.) In other words, the numbers are finally moving in the right direction. But while the trajectory of the pandemic is encouraging, the overall level of infection is staggering. “We are entering what may well be the toughest and deadliest period of the virus,” President Joe Biden declared in his inaugural address. The same day, the United States reported that 4,409 people had died of COVID-19, the highest toll of any day so far. Hospitalizations might be falling nationwide, but they remain twice as high today as they were at the peak of the previous two surges. In the South, new cases have fallen from their peak, but they are more numerous today than they were when the month began; in the Northeast and West, new cases exceed their level on December 1. The most crucial question for Biden—and for the country—is how long the overall decline can endure. Biden has described the task at hand as a “wartime” effort against the pandemic, but the success of his cause will rest on factors partially out of his control. The Biden administration is now running a race of vaccination versus variants--it must continue to suppress transmission, and vaccinate people, before more transmissible variants of the virus emerge. The winner of this race will depend on three unknowns: mitigation, evolution, and vaccine distribution. Since the pandemic began, two trends have defined the virus’s behavior. First, when cases and hospitalizations start to fall in a region, they continue on that path for some time. Second, when a community has a high level of ongoing infection—when the virus is simmering in the background but not yet boiling over and overwhelming hospitals—a new surge will soon start up again. Today, several key metrics are in decline, but overall community transmission remains at high levels. Those high levels of ongoing infection make the standard tools of mitigation—social distancing, masks, and work-from-home orders—even more important to avoid continued deaths. Yet the allure of vaccination is beginning to stymie mitigation policy in some places. In Arizona, for instance, Governor Doug Ducey has opposed implementing any new mitigation efforts, because vaccinations are imminent—even though only about six doses have been administered for every 100 Arizonans, according to Bloomberg. “The vaccine is the only solution. It is the first solution that has presented itself since January 27 [of last year], when we saw the first case,” Ducey, a Republican, has said. Ducey is not alone in resisting mitigation efforts; local leaders from both parties are loosening some of restrictions they implemented at the peak of the winter surge. Chicago, Baltimore, and Washington, D.C., have resumed some indoor dining, or are planning to resume it soon, as has the state of Michigan. Yet the virus has not been eradicated from those areas. In the District of Columbia, hospitalizations are below their peak, but still significantly higher today than they were at any point over the summer. At the same time, the coronavirus is mutating in predictable but alarming ways. As my colleague Sarah Zhang has written, the virus has developed more infectious variants in several different places around the world. The variant that emerged in the United Kingdom may be more than 50 percent more transmissible than the coronavirus strain that dominates in the U.S. (British Prime Minister Boris Johnson claimed on Friday that the same strain may also be 30 percent more lethal.) So far, these variants seem to respond to the vaccine, but without widespread mitigation efforts, the risk increases that the virus will develop even more transmissible and lethal variants. The most immediate risk is that these new variants cause another surge of infection, and death, before mass vaccination can increase the number of Americans with protective immunity. How likely is such a scenario? The highly contagious U.K. strain is already circulating in the U.S.: Epidemiologists have found it in at least 20 states, in many cases in Americans who have not recently traveled abroad. But that may be the least of our issues. The U.S. may have its own highly contagious strains, but we would not necessarily know about them. Infectious-disease researchers detect new variants of a virus by sequencing its genetic code as collected from hundreds of COVID-19 patients. And the CDC is only now beginning to surveil widely enough to identify new variants. One particular strain of the virus seems to have become prevalent in Southern California, but it is unclear whether this strain is more transmissible or just happened to infect more people in several unlucky super-spreading events. Earlier this month, a CDC study suggested that if the U.K. strain is the only more transmissible variant circulating nationwide, the U.S. should not expect to see a bump in cases until the spring—at which point more than 67 million of the most vulnerable Americans should be vaccinated, if Biden’s plan bears out. Yet these models, again, account only for the U.K. variant: If a separate, “California” strain exists and is already widespread, it may cause another surge before the vaccines can suppress transmission. Many days, the U.S. is already at or near the goal of delivering 1 million vaccine doses every day. More supply should come online soon. Potentially as soon as this week, Johnson & Johnson could deliver the results of its Phase 3 trials. The company aims to deliver 100 million vaccine doses by the spring. Not all of the news is so rosy. Pfizer has begun reducing the number of vaccine vials it sends to the U.S., after some pharmacists found an “extra dose” in some of the vials, The New York Times reported. Because Pfizer’s contract specifies that it will deliver a certain number of doses to the U.S., the company informed the Trump administration that it would deliver fewer vials than initially promised, according to the Times. But only some types of syringes are able to use that extra dose, so Pfizer’s legalistic move may effectively reduce the number of doses available to Americans. The U.S.’s vaccine supply, in other words, is uneven at the moment, although the Biden administration has vowed to invoke the Defense Production Act to strengthen the supply and distribution operation. The country may very well soon have tens of millions of doses on hand each week, allowing the number of Americans with immunity to outpace the growth of more contagious virus variants. Or the U.S. could find itself with another surge in cases and no near-term increase in its supply of vaccines. from https://ift.tt/36bsVKq Check out http://natthash.tumblr.com
0 Comments
Ruth Faden, an expert in biomedical ethics with Johns Hopkins University, has helped vaccine drives answer some tough questions: Who should be ahead of whom? Do we prioritize speed or equity? And once people are inoculated, should they get “vaccine passports” allowing freer movement? She joins James Hamblin and guest host Maeve Higgins on the podcast Social Distance to assess how we’ve done so far—and what we could expect next. Listen to their conversation here: Subscribe to Social Distance on Apple Podcasts, Spotify, or another podcast platform to receive new episodes as soon as they’re published. What follows is a transcript of the episode, edited and condensed for clarity: Maeve Higgins: How do you think vaccinations are going so far? Ruth Faden: Globally, or within particular countries? James Hamblin: Let’s start with the U.S. Faden: Because, globally, it’s a disaster. Within the United States, it’s not so great, but it’s way better than it is globally. Right now, we are really in a bad situation. We’ve hit the horrible 400,000 death mark. And while there is some indication that the death rate and the hospitalization rate may be flattening, it’s still not clear. And if it does plateau, it’s going to plateau at a really bad place, which is the place we’re in now. We only have about 12.5 million doses administered to people. That’s not full courses, that’s doses, because we’re still dealing with the two-dose vaccine. And that’s nowhere near the pace we need to be able to get our arms around this terrible loss of life. We need to really pick up the pace in this country. Hamblin: In the months leading up to the actual rollout of the vaccine, there was a lot of discussion of how we created hierarchies and lists of who would get it when. How has that short supply—or less-than-expected supply—changed or put an emphasis on those difficult decisions about who should be vaccinated first? Faden: In the summer and into the fall, an awful lot of effort was put into coming up with prioritization frameworks, with a lot of attention to the ethics justifications for which groups should go where: first phase, second phase … first half of the first phase, second half of the first phase … and so on. And, to some extent, that planning had to occur when it did, in the absence of specifics about either the particular characteristics of the vaccines, like how effective they would be or whether they would work for everybody. We didn’t know when we were doing that planning what the epidemiological context would be, that is: exactly how bad or better the pandemic would be when vaccines started to become available. And we didn’t know the pace of the supply. A lot of that planning was done with reasonable assumptions about those three things, but knowing that the particulars would necessarily have an impact on what could be done. And I’ve been part of those efforts, so I will include myself when I raise this criticism: There was insufficient attention to matching the carefully thought-through prioritization road maps with the realities of mass vaccination programs. Hamblin: How so? Faden: Well, as we are learning in the U.S., it is hard to mount a massive vaccination program in a context of constrained supply with complicated criteria for who should go when. If we look to a country where things have gone well, Israel—which is totally the opposite of the U.S.: tiny population, tiny geography, and a really coordinated health-care system, so, like, nothing like the U.S. They began and continued with a very simple prioritization scheme that was age-descending. That’s a lot easier to get your hands around logistically, or so it’s argued, than the way in which we’ve sort of marched our way through in the United States. Higgins: I wonder if there’s another example. Israel is tricky because they’re not vaccinating Palestinians, so I don’t know about them as holding them up as a great example. Faden: Well, I think maybe you want to distinguish between two different things. They are a great example of an effective public-health program. I’m not saying whether it’s an equitable public-health program. It’s efficient. They’re doing an incredible job of getting a lot of people vaccinated in a short context. Higgins: That’s a good distinction. Faden: That is very different from saying whether the Israeli government has a moral obligation to Palestinians, who are not living in the territory of Israel but over which Israel has control. That is a whole separate conversation. They are linked, but you want to be careful. Generally, there’s the question of what we sometimes call “humanitarian situations of special concern.” There are lots of places in the world where people are living where the countries that have some jurisdiction, military or political, over them, are not viewing them as citizens or residents of the country for purposes of vaccine distribution. That’s a huge, horrible, terrible ethical morass. It’s awful. But what is going on in Israel is an example of what can be done with a really high degree of attention to detail. Within the system in which they’re operating, for people who are legal residents of Israel, whether they’re Arab or Jewish or Christian, the system is quite fair. You just have to show that you are the age at the time that that age cutoff is called up. And they also manage to largely solve the “What do we do with the doses at the end of the day?” problem. Hamblin: We were wondering about that. Higgins: Yeah, there was a situation in Ireland, where I am at the moment, where a doctor gave out 16 extra doses to his family because he was worried they wouldn’t get used. But then members of the public found out and were very upset, understandably. But I can see it from both sides. Faden: So, look, this is a practical problem that needs to be dealt with pragmatically, but also with some attention to concerns of ethics and equity. The worst thing is to throw away a single dose of this precious vaccine. That’s ethically unacceptable. And from a public-health point of view, it’s just dumb. So if you haven’t planned for it and you’re at the end of the day and you’re close to the end of the window where the vaccine must be administered or tossed, I don’t have any trouble with grabbing any arm you can get from anybody who wants to be vaccinated. But stepping back, it’s possible to anticipate that you could be in that circumstance and plan for it. Even if you schedule appointments and have a very efficient system, there are going to be no-shows and there could be extra vaccine, just based on how it’s drawn out of the vial. So whether you use social media to alert people, kind of like vaccine flash mobs: It looks like we’re going to have X doses if you can show up by Y o’clock. There’s a queue. I live in Washington, D.C., and there are a couple of pharmacies that are reputed to let people know that they’re going to stop vaccinating at 8 p.m. and people can start queuing whenever they want in case there’s any vaccine left. It’s first come, first serve. And there have been reports of people lining up at, like, 3 in the afternoon for the possibility of a vaccine-access availability at 8. And a lot of the people who really need the vaccine right now are not positioned to be able to figure out how to check every two seconds on a website or wait forever for a phone call or navigate the system in a language they don’t know. We have a lot of equity challenges buried in the details. And then we have the equity challenges that come from the justified distrust of communities of color and poor people with respect to institutions generally and public-health programs in particular. Hamblin: We had a question from a listener asking about if and how it’s being kept track of who’s been vaccinated and who has not. Is there any discussion about the ethics of having a registry of who has and hasn’t been vaccinated? Faden: It’s a great question. There are two pieces to this. One: Absolutely, as a public-health matter, we have to keep track. That’s nonnegotiable. Now, the question is: What other data do you collect? Age, ethnicity, location? There’s that issue. And then there’s this issue of: Should any perks result from the fact that you’ve been fully vaccinated? And that’s the conversation about “vaccination passports” or “vaccination passes” of some kind. Hamblin: Like that you might not have to wear a mask if you’ve been vaccinated? Or something like that that could actually incentivize people to get the vaccine? Faden: Or maybe you have to wear a mask, but if you have been exposed and ordinarily you would be a contact and have to quarantine for two weeks, you would get a quarantine pass, for example. I don’t think anybody is going to say you don’t have to wear a mask. We don’t know enough about that yet. Hamblin: Yeah, we don’t know yet, but just in terms of the idea of what kind of things it might eventually be … Faden: Yeah, it could be something like that. And that’s a kind of calculated gamble too. No one is proposing that in the U.S. Higgins: If you could prove you were vaccinated, could you travel to another country, for instance? Faden: From a global point of view, it’s a complete structural-injustice mess. Because if we’re going to start privileging people—which makes a lot of sense, depending on what we learn about onward transmission and these vaccines, which we don’t know enough about yet … If we start basically saying that if you’ve been fully vaccinated, then you can start traveling globally. And we have a context in which a very tiny percentage of the world’s population outside of high-income countries gets access to the vaccine, who’s going to be able to travel globally? It’s an awful picture. The director-general of the WHO gave an address [recently], and he made a stunning point. There were 39 million doses of vaccine administered in 49 high-income countries as of [a few] days ago. Can you guess how many doses have been administered so far in a lowest-income country? Twenty-five total. Against 39 million. So I don’t think people have begun to get their heads around how wide the disparity is and how urgent it is to try to do something about this. We’re concerned about what to do because this doctor gave it to his family. I mean, there are definitely ethical issues there, and I don’t mean to dismiss them, but we have to put that in perspective as well. from https://ift.tt/2KHgU7V Check out http://natthash.tumblr.com Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. In last week’s update, we wrote that the United States had reported the worst weekly case, hospitalization, and death numbers of the pandemic. At the time, it wasn’t clear what proportion of the case and death increases were related to postholiday reporting backlogs. This week brings some clarity: The backlogs appear to be largely behind us, and the underlying trends are moving in the right direction for most of the country. Even for the states experiencing the worst outbreaks, we are seeing early indications that the rates of cases, hospitalizations, and deaths are easing, though some areas are still reporting dangerously high case and hospitalization levels and wrenching death rates. 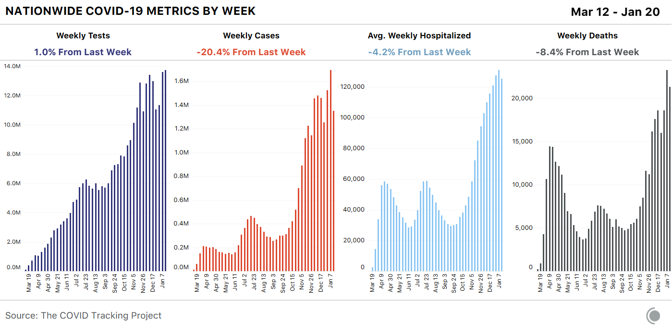
Weekly new cases for the seven-day period beginning Thursday, January 14 were down 20 percent, the lowest number of new cases we’ve seen for a non-holiday week since mid-November. As important, after 16 straight weeks of increases, average weekly hospitalizations dropped 4 percent this week—a modest improvement, but a good sign. Reported tests reached a new weekly high, edging out last week by 1 percent—though the high test numbers this week probably reflect the fact that the testing backlog is still catching up. [Read: The most reliable pandemic number keeps getting worse] States reported 21,301 deaths this week, the second-highest number of deaths of the pandemic to date. Yesterday, states reported 4,409 COVID-19 deaths, the highest single-day number of deaths on record. For comparison, in the week of September 24, 2020, states reported fewer than 5,000 deaths for the entire week. Because of the way states report data for nursing homes, assisted-living facilities, and other long-term-care facilities, our figures for COVID-19 in these facilities refer to the week beginning January 8. These numbers remain very alarming: For the second week in a row, LTC facilities reported the highest death toll since we started gathering long-term-care data last May—more than 7,000 residents and staff. The number of known deaths reported this week may include backlogged figures from the winter holidays, and they also got a boost from a change in Iowa’s death reporting that increased that state’s reported figure. 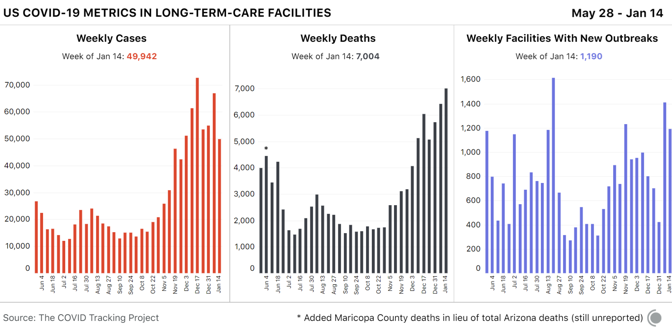
There is also tentative good news from long-term-care facilities: The number of new cases was down by about 15,000 this week. It remains unclear whether case data have fully normalized from the reporting delays associated with the holidays, but next week’s data should confirm whether this case drop indicates a real improvement in the situation in long-term-care facilities. Regional hospitalization and case dataA closer look at current COVID-19 hospitalizations offers good news for most U.S. regions. Hospitalizations remain very high but are declining modestly across the South and the West and continuing their substantial declines in the Midwest. In the Northeast, hospitalizations have plateaued. 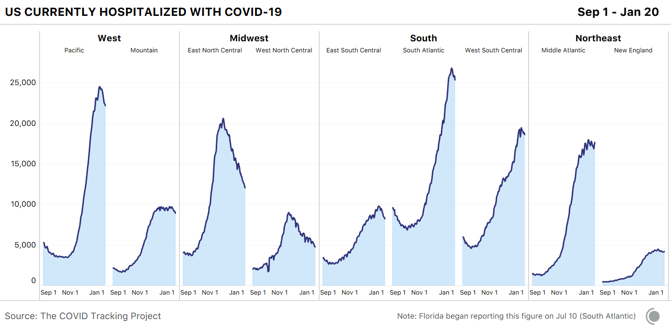
At the state level, hospitalization data remain encouraging: Hospitalizations are declining or flat in every state but New York. 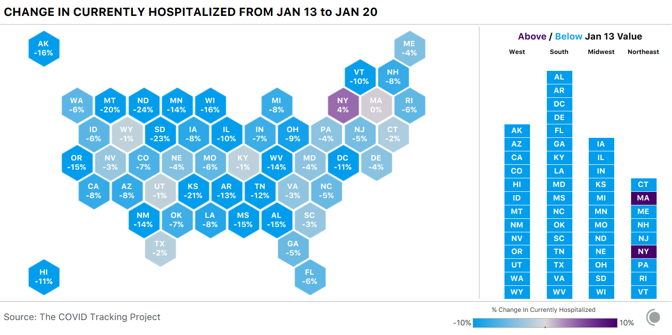
Cases, too, are falling in every region. In the Midwest’s “West North Central” division—which includes many of the states that had the worst per capita outbreaks late last fall—cases have very nearly returned to the levels reported at the beginning of October 2020. 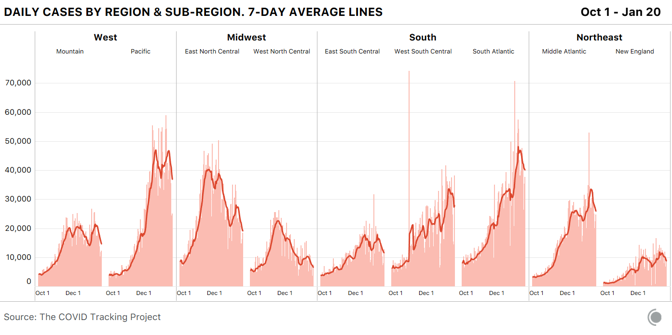
A breakdown of weekly reported COVID-19 deaths by census regions and subregional divisions shows that although deaths are falling modestly across the country, they remain painfully high in most regions. 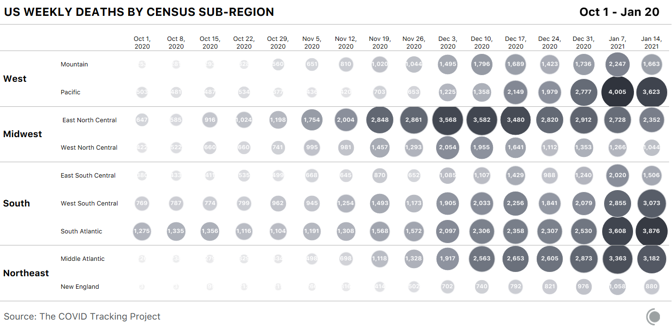
States we’re watchingCase and hospitalization declines are unquestionably good news. At the same time, in the country’s worst hot spots, states are still reporting very high numbers. Arizona’s case count has fallen from last week, but per capita, the state’s case numbers remain the highest in the country at a seven-day average of 958 per million. The state is now nearly tied with South Carolina, where cases are rising rapidly. In Yuma County, Arizona, home to many of the state’s seasonal laborers, the Associated Press reports that the county has a positivity rate of 20 percent, compared with 14 percent for the state as a whole, and county public-health authorities said last week that they had run out of vaccines. 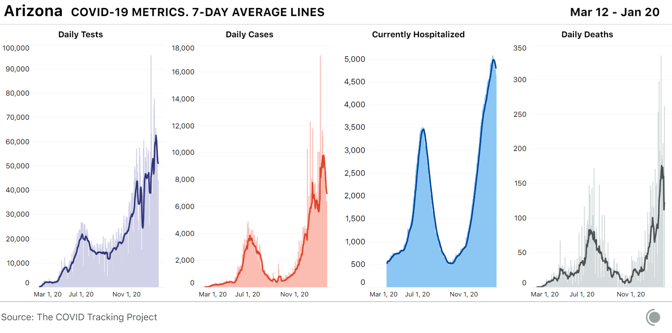
Hospitalizations lag behind cases, and Arizona’s per capita hospitalizations remain by far the highest in the country. Arizona’s hospitals are under severe strain, with 92 percent of all ICU and inpatient beds occupied as of Wednesday, accompanied by a surge in pediatric COVID-19 hospitalizations. Nursing homes are also experiencing an increasing number of cases and deaths, and Fox 10 Phoenix reports that 40 percent of Arizona COVID-19 deaths have come from nursing facilities. Despite this, delays in the distribution of vaccines mean that many facilities (and patients) are still waiting for the first doses. [Read: A vaccine for kids is coming, slowly] The disparity in COVID-19 outcomes for Indigenous people in Arizona has been pronounced throughout the pandemic. At least one in nine people identified as “American Indians or Alaska Natives” has tested positive for COVID-19 in the state, while one in 16 white residents has. Indigenous people in Arizona are more than twice as likely to have been hospitalized with COVID-19 as their white neighbors, and more than 2.5 times as likely to have died. 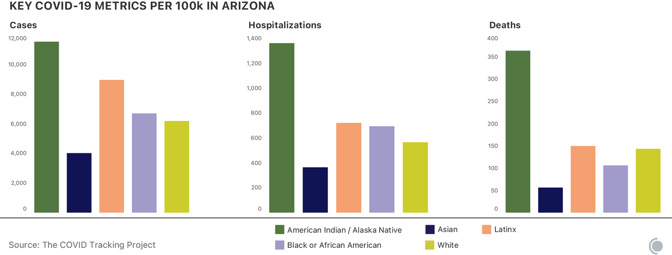
California, which reported the third-highest number of new cases per capita this week, is finally seeing the number of new cases reported each day begin to decline. Even the state’s Southern California epicenter is seeing modest but important improvements: Following weeks of record-breaking cases and hospitalizations in Los Angeles County, the number of new cases per day is down 17.6 percent from two weeks ago, and hospitalizations are down 10 percent over that same time period, according to data from the Los Angeles Times. County officials warn that the virus is still surging in the area, and that hospitalizations remain at dangerously high levels, with ICU numbers remaining nearly unchanged over the past two weeks. 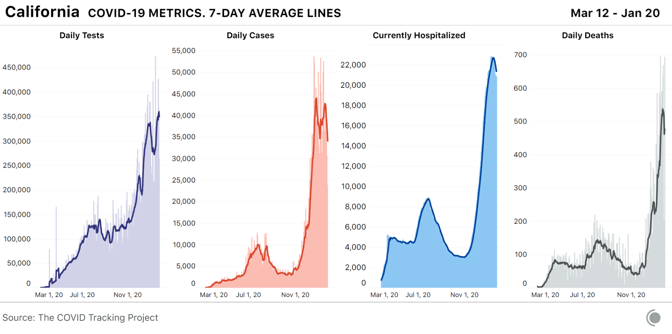
On Wednesday, the state surpassed 3 million total cases to date, meaning that one in 13 Californians has tested positive since the start of the pandemic. As we’ve seen over the entire course of the pandemic, rising cases lead to rising deaths. The massive number of cases in Southern California over the past month has resulted in a wrenching death toll: The state reported 3,331 COVID-19 deaths in the past seven days alone. In Los Angeles County, air-quality rules limiting the number of cremations each day have been suspended to allow crematoriums to clear a backlog of bodies at hospitals and funeral homes. In California, people identified as “Native Hawaiian and other Pacific Islander” are being disproportionately harmed by COVID-19. Although they make up a small part of the population, Native Hawaiians or other Pacific Islanders are three times as likely to have tested positive for COVID-19, and 1.8 times as likely to have died, as their white neighbors. Black people in California are 1.4 times as likely to have tested positive for, or died of, COVID-19 as white people in the state. Latino Californians, the largest single racial or ethnic group in the state, are 2.6 times as likely to have tested positive and 1.4 times as likely to have died as white residents. Alabama, which had the second-highest number of COVID-19 hospitalizations per capita last week, has now reported its highest ever number of weekly COVID-19 deaths. In a gruesome echo of Southern California’s outbreak, Alabama crematoriums are running “around the clock” to manage the increased demand. According to the CDC, Alabama also has the lowest COVID-19 vaccination rate of any state, although the Alabama Department of Public Health disputes the CDC’s numbers. 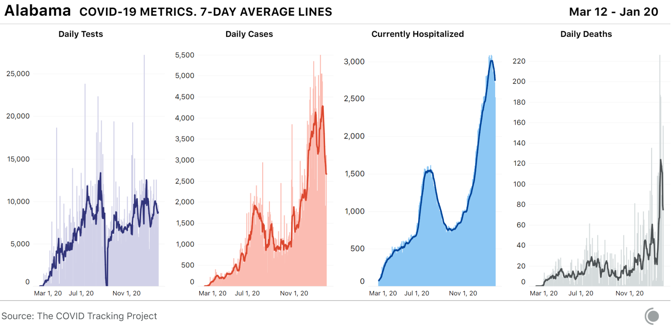
The Black population of Alabama is being hit hardest by the state’s outbreak. Over the past two months, the number of cases per capita for Black people has increased more quickly than for other groups. For the 57 percent of Alabama cases where race is reported, Black people are more likely than anyone else in Alabama to have tested positive for COVID-19, and they are the most likely to have died. [Read: The virus is showing Black people what they knew all along] Adjusted for population, Nevada had the second-highest number of people in the hospital with COVID-19 this week. It also reported its highest ever single-day number of deaths on Wednesday, most of which were reported in Clark County, where Las Vegas is located. Originally intended to be lifted this week, the state’s COVID-19 restrictions have been re-extended until February 15. On January 15, the Las Vegas Review Journal reported that a total of 40 prisoners in the state had died due to COVID-19, a number that is more than four times higher than the state’s eight cumulative deaths among prisoners as of January 7. 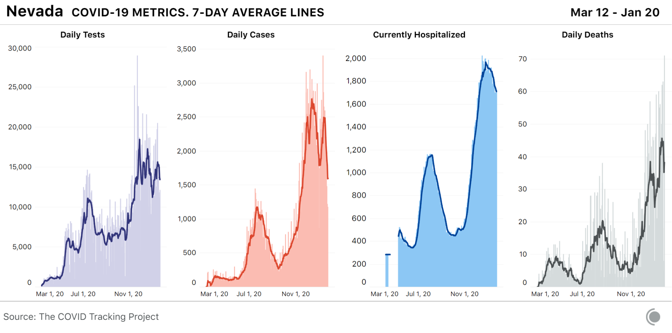
Throughout the pandemic, Latino people in Nevada have been more likely to experience COVID-19 than their white neighbors. One in nine Latino people has tested positive for COVID-19, compared with one in 15 white people in Nevada. We are frequently asked for data on known variants of SARS-CoV-2, the virus that causes COVID-19. At present, very little data on the spread of variants exist in the United States, and we need much more genomic-sequencing data to understand the degree to which the virus is changing, and where variants are appearing. Unfortunately, the U.S. currently ranks 43rd in the world for percentage of cases sequenced. By contrast, the United Kingdom, where the widespread B.1.1.7 variant was first identified, is ranked eighth in the world. Earlier this month, the director of the U.S. Office of Advanced Molecular Detection at the CDC’s National Center for Emerging and Zoonotic Infectious Diseases announced a plan to more than double the number of samples sequenced, from approximately 3,000 samples a day to about 6,500. The U.S. is currently reporting more than 200,000 new cases of COVID-19 each day. A state-run lab in Colorado was the first in the U.S. to identify a B.1.1.7-variant case this year and it is now routinely screening all samples submitted to the lab for this mutation. The Colorado Department of Public Health and Environment has also added variant case counts to their COVID-19 dashboards. To date, most states lack the resources to add genomic surveillance to their ongoing COVID-19 workload. from https://ift.tt/2Md8cP4 Check out http://natthash.tumblr.com A few days after Christmas, Molly Hering, 14, and her brother, Sam, 12, got their first shots as part of the Pfizer COVID-19 vaccine trials for kids. Their mom had heard about a clinical trial being conducted at Cincinnati Children’s Hospital, and Molly told me that she’d agreed to join because she wanted to contribute to the vaccine-development effort. Molly and Sam’s dad was recently hospitalized with COVID-19. (He recovered.) Both kids have spent most of the past year dealing with Zoom school and its attendant technical glitches. Molly finally went back to in-person ninth grade this month, but masks and social distancing are required at school. Like everyone else, she’s looking forward to the end of the pandemic. “I’ll finally be able to go to school normally,” she said. With COVID-19 vaccines proven to be safe and effective in most adults, Pfizer and Moderna have both begun U.S. trials for kids as young as 12. And if those trials go smoothly, the vaccines will be tested in younger and younger kids. This is typical for new vaccines: “It’s called the age deescalation strategy,” Carol Kao, a pediatrician at Washington University in St. Louis, told me. There are some 70 million kids in the U.S., nearly a quarter of the country’s population. Children in general are not especially vulnerable to COVID-19; most infections are mild or even asymptomatic. In some very rare cases--less than 0.01 percent—young patients can develop a complication called multisystem inflammation syndrome, or MIS-C, but it is generally quite treatable in a hospital. Vaccinating kids, however, is often not just about the direct and immediate benefits to them. It’s also meant to protect children against diseases that would otherwise become more dangerous for them as adults—measles, mumps, and chicken pox are three common examples—and dampen the overall spread of these diseases. In the short term, the primary reason to vaccinate children against COVID-19 may be that the U.S. will have a hard time reaching herd immunity otherwise. Vaccines that work in adults generally work in children. But their effects can differ, especially in very young children. In newborns, for example, antibodies passed to them in utero can interfere with the protection conferred by the measles vaccine, which is why that vaccine is not given until babies are 12 to 15 months old. An early version of the pneumococcal vaccine did not work well in children under 2, because it stimulated a part of the immune system that was not yet mature. Multiple factors determine the recommended age for a vaccination. “For example, when’s the peak incidence of disease? When is a child most likely to respond to the vaccine?” says Cody Meissner, an expert on pediatric infectious diseases at Tufts. The answers to those questions might not align. For instance, the vaccine for HPV, a sexually transmitted virus that can lead to cervical cancer, is given to boys and girls as young as 9 years old because it stimulates a better immune response in preteens than in older adolescents, even though preteens are unlikely to need the protection until later in life. Even though kids rarely get seriously sick from COVID-19, the vaccine can protect them from an illness that may still be bad enough for them to miss school and their parents to miss work, Jeff Gerber, a pediatrician at Children’s Hospital of Philadelphia, told me. “Even those two-to-three-day illnesses can pile up.” He pointed out that the flu vaccine is recommended for kids, and about the same number of children died of the flu last season as have died of COVID-19 to date. But the main argument for broadly vaccinating children is that doing so is likely to reduce COVID-19 transmission. Although schools have not been sources of large outbreaks, many switched to distance learning, and most of those that held in-person classes required masks and distancing. If school buildings reopen without these precautions sometime this year, after adults get vaccinated but while kids are still vulnerable, they will essentially be hosting mass gatherings of unvaccinated people, says Jason Newland, a pediatrician at Washington University. “Guess who’s going to end up having it? All the kids,” he told me. “And those kids with certain underlying conditions are disproportionately impacted.” What’s more, kids could bring COVID-19 home from school, even if they don’t have symptoms. “Children could pass it on to Grandma and Grandpa. They can pass it on to another loved one who has diabetes or has obesity or has chronic kidney disease” and is not yet vaccinated, Newland said. Public-health experts think that if precautions are in place, community transmission is low, and teachers and high-risk people are vaccinated, reopening schools in 2021 will be worth any remaining risk, given the many and wide-ranging consequences of keeping them closed. But the more children are vaccinated, the safer and more normal school reopenings will be. The ultimate goal of most vaccination campaigns is not just to protect the individuals who get the vaccines, but to prevent the spread of the disease to those who can’t get it, such as infants and people at risk of allergic reactions. The more transmissible the virus—and unfortunately COVID-19 appears to be evolving to be more transmissible—the more people need to be vaccinated in order to reach herd immunity and stop its spread through a population. The herd-immunity threshold against COVID-19 is estimated to be somewhere between 60 and 90 percent of the population. Because some people can’t get the vaccine and some may be steadfastly opposed to it, the U.S. needs to vaccinate as many of the rest of us as it can. “What we want to do is reduce the number of people who might be contagious to others,” Meissner told me. Children will almost certainly need to be a part of that effort. A still unanswered question about the COVID-19 vaccines, however, is how well they protect against asymptomatic transmission of the virus. When vaccinated people are exposed to the virus, their bodies’ immune response tamps down its replication—enough to reduce symptoms by 95 percent, according to the results of the Pfizer and Moderna trials for adults. But a person who is vaccinated and then exposed might still carry enough virus to spread it to others. Experts think the vaccines very likely reduce the risk of asymptomatic transmission, but follow-up studies are needed to find out by how much. How soon the vaccines are available to children will depend on how long the clinical trials and the FDA review process take. In the most optimistic scenario, a vaccine could be available for large numbers of kids, especially older ones, in time for the start of the school year in the fall. But last week, Operation Warp Speed said that Moderna was having trouble recruiting enough participants in its trial for adolescents, having enrolled only 800 out of a planned 3,000. The company’s CEO also said that while Moderna would soon begin trials for kids ages 1 to 11, it did not expect to have results until 2022. Pfizer’s adolescent trial has reportedly finished enrollment, though the company declined to specify when it plans to move on to younger children. The FDA fast-tracked the COVID-19 vaccines for adults using a process called emergency use authorization. But the normal vaccine-approval process may be more appropriate for children, says Vanderbilt’s Tina Hartert, who is leading a study on the incidence of COVID-19 in kids. Approval will take more time for several reasons. For example, the FDA has said that it wants to see more safety data—six months or more depending on the novelty of the vaccine technology—compared with the two months required for emergency use. The newness of the COVID-19 vaccines combined with the mildness of the disease in children might lead to hesitancy in some parents. When the chicken pox vaccine first became available, in the 1990s, uptake was slow—until public schools started requiring it. Meissner, who sits on the FDA’s vaccine advisory committee, said he thinks schools are unlikely to require a vaccine that is authorized only for emergency use. But there is genuine debate among advisory groups about whether to mandate COVID-19 vaccination at all. “Once you require a vaccine,” Meissner says, “a lot of people who ordinarily might get the vaccine become indignant and say, ‘I’m not going to be told what I have to do for myself or my family.’” In the long term, the COVID-19 virus is unlikely to go away entirely—and neither is the need for vaccination. If the virus continues to mutate or if immunity wanes, annual vaccinations or boosters every few years might be necessary. The vaccines could also become part of the recommended childhood immunization schedule. Experts say this is the best way to ensure that the entire population remains protected. “The most successful implementation programs are universal pediatric programs,” Kathleen Neuzil, a vaccine researcher at the University of Maryland School of Medicine, told me. Parents are already used to their children getting shots from pediatricians, and pediatricians are already used to vaccinating large numbers of children. Although children may not be particularly vulnerable to COVID-19, they will be when they reach adulthood. And vaccinating large numbers of adults, as the world is currently finding, is very difficult indeed. Molly Hering, who is participating in the Pfizer trial, doesn’t yet know whether she got the placebo or the actual vaccine. She and her brother are using an app to track their side effects; she had some nausea and headaches after she first got the shot, while he had a low fever. They are going back for their second shots this week. For childhood vaccinations to help slow the spread of the virus, more volunteers will have to join them in the trials. from https://ift.tt/3qDHs9n Check out http://natthash.tumblr.com
Dear Dr. Hamblin, I’m still confused about what our lives will be like after we are vaccinated. As I understand it, it will still be possible to get the virus, but hopefully the course won’t be as severe or life-threatening. And we are going to have people who won’t even get the vaccine. Do you foresee us still wearing masks for the next year or two? I hate to even type this question. Nancy Bernardy New London, New Hampshire Nancy, I can’t wait to stop wearing masks. I want to go out without a mask so badly that I’ve been dreaming about it. That’s how far the pandemic has lowered the ambitions of my dreams. Last month, President-elect Joe Biden said he will urge Americans to wear masks for the first 100 days of his presidency. “Just 100 days to mask,” he said, “not forever.” That sounds manageable even for those of us who can’t wait to go out maskless: I’m absolutely sick of this, but I can do 100 more days. Setting this sort of short-term goal can be helpful in making a seemingly endless challenge like this pandemic more manageable. But to be blunt, 100 days is not a realistic end point. On our current trajectory of illness and infection, masks will be part of most Americans’ lives for at least the rest of the year, and possibly longer. My hope is that it will soon be possible to say, as a general rule, that once you’ve been vaccinated, you don’t have to wear a mask. But that depends on two key variables. The first is that a vaccinated person could theoretically still transmit the virus. This isn’t typically an issue after vaccination against respiratory viruses, once your body develops antibodies and other means of immune memory. If you inhale the virus again, these defenses should identify and eradicate it before it multiplies in large numbers. But that doesn’t mean viral particles can’t briefly cling to your nasal cavity and replicate before your body’s alarms go off, creating a brief window in which you could transmit the virus to someone else. This coronavirus warrants special caution because we know that it can be transmitted by people who have no symptoms and low levels of virus in their bodies. That means it is especially adept at lingering in people’s noses without quickly triggering an immune response (which is the source of most symptoms, such as cough, muscle aches, fever). [Read: The next 6 months will be vaccine purgatory] The vaccines that have been rolled out in the U.S. do seem to be extremely, surprisingly effective at preventing people from falling sick with COVID-19, but the clinical trials did not monitor the mechanisms through which this protection is conferred. People were not tested to see when and how reliably they developed antibodies, nor screened to see whether they ever carried the virus. Additional research is under way to address these questions in coming months. Although I would be surprised to learn that vaccinated people are spreading the virus to any significant degree, it’s reasonable to have everyone continue wearing masks until we know more. The second variable in the countdown to mask-free life is how quickly entire communities get vaccinated. When the virus is spreading widely and very few people are vaccinated, the chance that a vaccinated person will carry the virus (and possibly even get sick, since no vaccine is 100 percent effective) is simply too high to suggest that anyone forgo masking. But as more and more people get vaccinated, the potency of each vaccine grows. Even if vaccinated people do prove to have the potential to carry and spread the virus in small amounts, for brief periods, that risk can be rendered moot if almost everyone gets vaccinated. All of this is contingent on the assumption that immunity generated by vaccines is reliable and long-lasting (which it seems to be, so far) and that the virus does not evolve to become resistant to this immune protection in the near term. Eventually, it likely will. But by that point, hopefully, the rates of transmission will be low enough that we can quickly identify new variants and modify vaccines accordingly, to stay ahead of any new surges. The bottom line is that the less the virus is circulating in the U.S., the more confident we can be transitioning away from masks. Unfortunately, we haven’t collectively actually started wearing them. More than 3,000 people are dying every day in the U.S. alone, and hundreds of thousands more are being infected. This wouldn’t be happening if we were all wearing masks effectively. Before we truly begin to think about the end of masks, we need to think much more seriously about how to use them better. [Read: The end of the pandemic is now in sight] I’d love to stop wearing masks. They erase the subtleties of communication that tether us to humanity, the cues that give context and nuance to everyday interactions. They make people feel two-dimensional. But we are far from done with them. I hope that if we can accept this reality soon, we can focus more on building public support and distribution channels for quality masks. There’s room for someone to win a Nobel Prize for figuring out how to get Americans to wear their mask over their nose. It’s easy to become numb to the numbers of people who are getting sick and dying every day, and let the annoyance of masks feel somehow more comparably urgent than it is. But even if the mortality rate were cut in half, and then cut in half again, we’d still be losing hundreds of people every day. For the foreseeable future, even among the vaccinated, masks will at the very least be symbols of solidarity and empathy. That symbolism may have real consequences. The clearest, most urgent challenge of the pandemic remains simply getting people to wear masks (and wear them correctly). The message would be made more complicated by creating two classes of people, some who have to wear masks and others who don’t. However long we have until the end of masks, we’ll get there far faster if we act together. “Ask Dr. Hamblin” is for informational purposes only, does not constitute medical advice, and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. By submitting a letter, you are agreeing to let The Atlantic use it—in part or in full—and we may edit it for length and/or clarity. from https://ift.tt/39NSB0F Check out http://natthash.tumblr.com Tomorrow, America inaugurates a new president. With the transfer of power comes the transfer of responsibility for the COVID-19 pandemic. On the eve of Joe Biden’s inauguration, the toll of the pandemic stands at 23.9 million cases and 392,428 deaths, according to the COVID Tracking Project at The Atlantic. There are 123,820 people hospitalized. Today alone, states reported 144,047 cases and 2,141 deaths. Ron Klain, the incoming president’s chief of staff, has warned that, by the end of February, COVID-19 may have taken 500,000 American lives. To reach that marker, the country would have to average 2,689 deaths every day until then, all too plausible a scenario. The seven-day average of deaths in the U.S. first surpassed that number on January 73. It’s currently at 2,988. Some modest signs do indicate that the country could be reaching a plateau or peak after nearly four months of climbing daily cases and hospitalizations, followed by more than three months of climbing daily deaths. Cases are falling in the overwhelming majority of states right now, and hospitalizations are falling or holding steady in most. If the country has reached a peak of COVID-19, however, this peak is the highest of the pandemic so far. And the more infectious B.1.1.7 variant, which has been found across the United States, could drive the peak higher, just as the first signs of its retreat have begun. Current hospitalizations are always the most stable indicator of the pandemic’s progress, and after peaking at 132,474 on January 6, they have declined more than 6 percent—meaning that 8,654 fewer people are in the hospital now, compared with two weeks ago. Hospitalizations have declined, too, in every region for at least the past week or so. Still, they are more than twice as high as the spring and summer peaks combined, both of which stopped just short of 60,000. And if the current peak follows the path of the previous two, the decline will be slow; the spring and summer peaks took about a month to build from the previous low, and then about two months to subside to the next low. Across the country, though, regional cases per million have been declining, with a substantial drop in the Midwest since late November and recent, short-term declines in the other three U.S. regions. Deaths, a lagging indicator, may be reaching a plateau in all regions as a result; there are the first hints of it in the seven-day average—ever-so-slight changes in momentum visible at the edge of the graphs below. Much of what happens next will depend on conditions in some of the country’s largest states— California, where the seven-day average of hospitalizations peaked at 22,703 on January 12; Arizona, which has the highest per capita hospitalization rate in the country and has of late had the worst outbreak in the world; Texas, where hospitalizations and deaths are well above prior peaks and climbing; and Florida, where hospitalizations and deaths may be peaking after a steady rise going back to late fall. New York may be hitting a second peak or plateau of hospitalizations, at a seven-day average just under 9,000, about half of its awful spring peak. New cases and hospitalizations are climbing in Virginia, which is at about twice its previous hospitalizations peak, in May. North Carolina’s seven-day average of hospitalizations has been climbing continuously since early November. But at the state level, peaks are not necessarily followed by an immediate decline. Missouri has had a seven-day average of hospitalizations between 2,500 and 2,800 since late November. New Jersey has remained between 3,600 and 3,700 since December 16. Even assuming that we are at a peak, unwinding the damage will take long enough as it is—at least a couple of months, if the previous lower peaks are any indication. The Biden administration inherits a mess, and now the B.1.1.7 variant of the virus, which may be 50 to 70 percent more transmissible, has been found in many states, suggesting that it’s widespread. But the administration also has the tools to clean this mess up. It has promised new, seemingly more aggressive action. The vaccine is rolling out, at an estimated rate of nearly 777,000 doses administered a day. We may still hope that this will be the worst point of the pandemic—the peak of this horrifying wave—and that from here the numbers will drop slowly but inexorably down. from https://ift.tt/3nY7YIX Check out http://natthash.tumblr.com When a hospital is in trouble, the signs are unmistakable. The number of COVID-19 admissions rises quickly. The number of patients who remain hospitalized grows steadily—and the bar to be admitted gets higher. The percentage of patients in intensive-care units increases. Supplies run low. As an ICU nears capacity, sick people get less care than they would have. More people suffer, and more people die. Right now, in Alabama, Arizona, and California—Los Angeles, especially—this is exactly what’s happening. We know this because of the data system that’s now in place. But until recently, we did not have this national picture. Who had the most COVID-19 patients? Which hospitals’ ICUs were overrun? Who had staffing shortages? No one could say. Even assuming that the federal government could have executed a competent pandemic response, it couldn’t know where help was needed. The government needed a national hospital-data system. So multiple teams scrambled to build one. In a short time, control over this hospitalization data became one of the most hotly contested elements of the American response, as fears of Trump-administration meddling cast doubt on the Department of Health and Human Services. Now the Biden administration is poised to take over as the country faces the worst surge yet, and hospitalization data may be the most important information it will have in the fight to save lives. The administration must decide where those data will live. Since July, these data have been routed through the Department of Health and Human Services, but some officials inside the CDC are trying to regain control. It might seem obvious that the CDC, the traditional repository of infectious-disease information, should win this intragovernmental battle, but the reality is much more complicated. The current, HHS-run system works—unlike so much else in the response—and with these data flowing in, the federal government can dispatch help to hospitals that need it. If the new administration changed that system, it would be setting aside the best available data about the pandemic, and gambling that it could build a better system when it cannot afford to lose. Since March, I’ve run the COVID Tracking Project with Erin Kissane, dozens of staffers, and hundreds of volunteers. We have pieced together national data sets on tests, cases, hospitalizations, and deaths by compiling the information that states publish. The hospitalization data that we’ve pulled from the states became the de facto national standard for the majority of the pandemic. Our team has made hundreds of contacts with local, state, and federal officials to clarify what the numbers on all those dashboards actually mean. And through that work, we’ve been able to compare what states say is happening with whatever the federal government publishes. Hospitalization data reveal the condition of the country’s hospitals: COVID-19 admissions, currently hospitalized patients, ICU availability, and access to personal protective equipment and other supplies. In July, the Department of Health and Human Services directed hospitals to send information directly to an HHS database, bypassing the CDC, which prompted a series of articles in The New York Times casting doubt on the HHS system. There was reason to worry: HHS officials had tried to pressure infectious-disease experts, including Anthony Fauci, to echo President Donald Trump’s misleading public messaging about the pandemic. And Secretary Alex Azar and Deborah Birx, the White House’s coronavirus-response coordinator, were seen as beholden to Trump. Anonymous CDC officials said the change had been a surprise, and insinuated that perhaps the data would be manipulated. But what really happened is widely, wildly misunderstood. Although the CDC did not respond to multiple requests for comment on this story, internal communications show that the agency agreed to the change because of the limitations of its own system. And while the switch was rocky at first, over time the HHS system has become the most reliable source of federal pandemic data. “I’m not going to pretend that the data wasn’t messy at first, but the aspiration was valuable, and particularly over the last few months, you could see the data getting better and better,” David Rubin, the director of the PolicyLab at Children’s Hospital of Philadelphia, who has worked extensively with COVID-19 data, told me. “I think it would be a grave mistake to throw it out and go back to what we were doing before.” At the COVID Tracking Project, we were initially dismayed by the HHS changeover, but we watched closely as the system stabilized and began to become more reliable. In a series of analyses that we ran over the past several months, we came to nearly the opposite conclusion of other media outlets. The hospitalization data coming out of HHS are now the best and most granular publicly available data on the pandemic. This information has changed the response to the pandemic for the better. “Hospitals are now beginning to see how folks from Operation Warp Speed are using the data to identify specific shortages of specific supplies and reach out: ‘Are you okay? Can you get them from your supplier? Or can we help you in some way?’” Nancy Foster, the vice president for quality and patient-safety policy at the American Hospital Association, told me. Amid the United States’ overall failure to contain the pandemic, the small data team at HHS did a good thing. Biden’s team did not respond to a request for comment on this story, but starting on Wednesday his administration will have the power to choose what happens to this hospital data. Disrupting the flow now—when 124,000 people are hospitalized with COVID-19 and more than 3,300 people are dying each day—is a risk the country doesn’t need to and should not take. Pieces of data do not simply exist. They must be extracted from reality and processed into usable forms. From the molecules of the virus on up, measurements have to be taken and facts tabulated. These numbers have to flow from labs and medical examiners, hospitals and public-health departments, into larger systems, where they then get summarized into statistics. For example, most states identify most cases electronically, based on lab results. But not every state’s electronic reporting is equal. Some use advanced electronic-case-reporting protocols, while others rely at least in part on forms sent via fax. America’s system is incredibly decentralized, with thousands of different sources of data, and it is rife with idiosyncrasies and potential points of failure. Its complexity and heterogeneity are key weaknesses in U.S. public-health surveillance. It didn’t have to be this way. Years ago, the CDC prioritized data modernization as part of a plan to be ready for a possible pandemic, and the agency appeared to be making good progress. In 2019, a group of public-health experts even ranked the United States No. 1 out of every country in the world for pandemic preparedness, including data collection. We now know that the CDC and the rest of the federal government were not ready to confront the real thing. “As a country, we are really underprepared for large, real-time data collection and sharing,” Nahid Bhadelia, an infectious-disease physician at Boston University School of Medicine, told me. “And real-time outbreak analytics? Well, that’s like asking a Model T to compete on the Autobahn.” In the chaotic early days of the coronavirus crisis, the United States probably confirmed only 10 percent—or perhaps as little as 5 percent—of cases, though no one will ever know for sure. Even now some deaths are being reported weeks after they actually occur. Media outlets and government officials often say, as shorthand, “3,000 people died from COVID-19 yesterday,” but that actually means 3,000 deaths were reported yesterday. Though we usually don’t know exactly, the people represented by that number may have died two, five, 15, or 50 days ago. Hospital data began in even worse shape than testing, case, or death data. COVID-Net, a system for estimating hospital strain, drew on a network of only about 250 hospitals in 14 states. It did not provide granular national data. Beginning in March, different pieces of the federal government tried to stand up hospital-data systems. The CDC took a system created for tracking infections transmitted in hospitals, the National Healthcare Safety Network, and jerry-rigged it to take in COVID-19 patient data. HHS contracted with a small health-care-IT firm, Teletracking, to create a similar system. And Deborah Birx’s team worked with FEMA’s National Response Coordination Center, HHS, and the CDC to contract with Palantir, which built software called HHS Protect. Hospitals or their intermediaries—such as state hospital associations—could send information to any of the three systems, and eventually that data would drop into HHS Protect. Much has been made of the decision to use Palantir for HHS Protect, not least because one of Palantir’s co-founders, Peter Thiel, is a high-profile Trump supporter. The concern was reasonable enough. But HHS officials say they went with the company because the CDC already worked with Palantir. In fact, HHS Protect is an offshoot of another system Palantir produced, known as DCIPHER Cloud, which began under President Barack Obama. “It was really about using what was already in-house,” Kevin Duvall, the deputy chief data officer at HHS, told me. Throughout the spring, hospitals and states worked to create systems for reporting data to the federal government. States published their own accounting, too, which we gathered at the COVID Tracking Project. Those state hospitalization data did not match what we saw the federal authorities reporting. When we looked at May and June, we could see the CDC estimates for hospitalizations bouncing up and down. They look like a seismograph during an earthquake. Given that the states were reporting fairly smooth curves, we concluded that the fluctuations in the CDC data did not reflect reality, but were artifacts of the reporting process. If fewer hospitals reported to the CDC, then it could push down the number of hospitalizations, even if there were still sick patients in those facilities. It was impossible to know for certain, but the state data were almost certainly more reliable. In mid-July, as the Sun Belt teemed with infections, members of the White House Coronavirus Task Force realized that they needed to ask hospitals a new question: How much remdesivir did they have on hand? (Clinical trials had shown that the drug was more effective when administered earlier in the course of a COVID-19 infection, not later, after more severe illness had set in.) According to correspondence obtained by The Atlantic from a source who requested anonymity because they were not authorized to speak about the communication, the Data Strategy and Execution Workgroup at HHS—the team tasked with providing data for the federal coronavirus response—requested that the CDC add a single data field about remdesivir to the National Healthcare Safety Network (NHSN), its hospital-data-collection system. This is what you might think of as a new column in a spreadsheet, but officials ran into a problem: The CDC staff said that change would take more than three weeks, at a time when hospitalizations were approaching the highest levels of the pandemic to that date. NHSN was an old system, snapped together from other IT components in 2005 to track infections spreading in hospitals. Hospitals were familiar with it, and it came with a preexisting $60 million contract with a major federal contractor, Leidos, to keep it running. But it had not been built for the kind of flexible emergency response that this unprecedented pandemic required. The request to add the data field went all the way to Sherri Berger, chief operating officer of the CDC. But the word came back: The field could not be added faster. So the CDC gave the team within HHS the go-ahead to change the reporting system itself. This switch to HHS Protect was rushed—hospitals had just five days to figure out the new system before it went live—and hospital reporting fell rapidly, according to a dashboard HHS maintains. The change caused hiccups in state data, too, and the COVID Tracking Project noticed major reporting problems right as hospitalizations were peaking in hard-hit regions. There were other ominous signs of malfunction, or worse: A previously public dashboard showing hospital capacity blinked offline. A big story ran in The New York Times suggesting that the changeover had surprised the CDC and focusing on the possibility of political interference with the data. A CNBC headline read, “Coronavirus Data Has Already Disappeared After Trump Administration Shifted Control From CDC.” No one seemed to believe what the CDC’s director, Robert Redfield, said at a press conference: “In order to meet this need for flexible data gathering, CDC agreed that we needed to remove NHSN from the collection process.” The idea that the Trump administration would try to suppress COVID-19 data was not far-fetched, but the HHS staffers I spoke with said that public perception was misguided. The people on the team were not Trump-administration loyalists, but civil servants from across the federal government. Its leader, Amy Gleason, came from the U.S. Digital Service, a signature achievement of the Obama administration that brings technologists into the government from private industry. “It’s truly interagency,” Gleason said. “Every day I work with people from 13 different agencies and components, side by side.” As outside pressure mounted, they were scrambling to build a complicated system in a moment of national crisis. “I know there have been lots of stories written about the relationship of CDC to HHS. But I will say this: We weren’t prepared from the data perspective for the challenge that awaited us,” said Rubin from the Children’s Hospital of Philadelphia. “The systems for influenza based on sentinel surveillance were not sufficient for a pandemic of this magnitude, so creating a public-health war room is a noble goal. The question is why we didn’t have something like this previously.” Immediately after the switch-over to HHS Protect, the discrepancies between the federal data and state data really could be enormous. On some days in late July, HHS reported 200 percent more hospitalized patients than some jurisdictions themselves were reporting. While this was disturbing, an overcount of hospitalizations, making the pandemic seem more severe, was also a sign that the problems were unlikely to be purely political in nature. As the HHS data became public, we at the COVID Tracking Project found that news organizations and many public-health professionals were continuing to rely on our hospitalization numbers, even though an official government entity now provided similar data. HHS had major logistical problems to deal with. After the changeover, the team had essentially no hospitals reporting all of the data requested every day for the month of July. Many hospitals were unhappy that there had been disruptive changes. But Nancy Foster credited Amy Gleason with putting a moratorium on tweaks to the system. She also built a troubleshooting team with hospital liaisons drawn from staff at the CDC, HHS, and other parts of the federal government. “It was really under Amy Gleason’s leadership that the folks from HHS started to work with states and other data intermediaries between hospitals and HHS Protect to understand where there were glitches in their processes and to help the states straighten those out,” Foster said. Jim Jirjis, the chief health-information officer at HCA Healthcare, which runs 185 hospitals across the country, considers the HHS effort highly competent. “The fact that there was listening and the ability to pivot and change was very, very reassuring that our government can do a really good job of modifying in the middle of a pandemic,” Jirjis told me. The improvements didn’t happen all at once. The federal government still had not released the granular data that it was receiving from hospitals and that underlay the state statistics. Civil servants across the government might have been striving to understand the spread of COVID-19 with great specificity, but their work was not reaching the public. At the COVID Tracking Project, we were keenly aware of how little information the public was receiving. And we, like many other people, worried that HHS officials would attempt to influence the data. While hospitalization data were trickling out, other information remained locked up inside the government. “As soon as COVID became a political issue, the administration willingly withheld data that showed how severe COVID was spreading in our communities,” says Ryan Panchadsaram, the former deputy chief technology officer of the United States under Obama and a co-founder of COVID Exit Strategy, which tracks the government’s response. “While internal reports were highlighting the ‘red zones’ and ‘areas of concern,’ the president and vice president continued to share that the reaction to COVID was ‘overblown.’” So at the end of the summer, we decided to look for signs of cooking the books in the federal hospitalization data. First, we simply looked to see if there were obviously political patterns in the data—say, red states with lower hospitalization numbers than anticipated, or overall depressed numbers. We didn’t see anything like that. Then we ran statistical tests looking at the variance in data from different states. What we found surprised us: The data that were flowing through HHS were much less spiky than what had flowed primarily through NHSN. In fact, at least on initial inspection, the HHS data looked a lot like our patchwork of data from states, which for the most part was not riddled with weird jumps or unexplained phenomena that were obviously not reflective of reality. When cases rose, hospitalizations did shortly thereafter. As the HHS data came to resemble the state data, we began to suspect that perhaps the HHS data had, as we put it in an internal report on August 20, “enormous potential to be the Federal numbers we’ve always wanted.” Stitching together state reporting into a national data set is an incredibly research-intensive way to produce those statistics. We have to figure out precisely what information 56 states and territories are reporting, and even then, we cannot guarantee perfectly comparable data. HHS, for its part, simply asked states to report all confirmed and suspected COVID-19 hospitalizations in the same way, creating a consistent and standardized data set. Once hospitals learned the system, the data solidified. Jason Salemi, an epidemiologist at the University of South Florida, described the changes as “amazing improvements.” “For a long while, there was very little help from federal data—it was a massive disappointment and failure to serve the public at a time when such information was direly needed,” Salemi told me. Since then, HHS “has stepped up to the challenge in a major way.” Some critiques of the HHS-generated information have called its accuracy into question. There are many data sets in HHS Protect that originate in many different places, so we cannot speak to all of them. However, the COVID Tracking Project can check HHS against the state reports. In late November, we found that the data had come to match almost perfectly. Not all states report precisely the same way, and the COVID Tracking Project runs one day behind HHS, but after we took those factors into account, we found that HHS and state data were now falling within 2 percent of each other. If the HHS data were off, then the data produced by every state were also off. For the week of December 28, the most recent data available, 96 percent of hospitals reported every data point to HHS every day. The interagency team led by HHS has done what had seemed impossible: gotten every hospital in America to tell the federal government what’s going on. “This pandemic shined a bright light on the data gaps we had in our understanding of the magnitude, spread, and burden of disease, across each community, county, city, and state,” Irum Zaidi, the White House coronavirus-response coordinator and chief epidemiologist, told me. “The system we needed and have set up makes every patient visible across the U.S. in order to provide the limited resources such as remdesivir, supplies, and staffing to every rural and urban hospital.” As the data improved, they became more and more available to the public. First up, HHS published the “metadata” about how facilities were reporting. This let us see for the first time how many hospitals were reporting. Then it released staffing-shortage details. Bit by bit, as the fall turned to winter, HHS published much of the crucial data that critics of the administration had been asking for. The capstone came last month, when HHS released data for every hospital in the country, exactly the kind of granular information that is necessary to understand where hospital systems are being overwhelmed. And given the general disaster of COVID-19 in America, there are many places that desperately need help from the federal government to secure supplies and shore up staffing. This data set is not perfect—no data set is—but it is the best available. “I am heartened to see facility-level [information] because we can also get a sense of how the same facilities are doing over time,” BU’s Nahid Bhadelia said. “This level of granularity also allows researchers to create a better evidence base for policy recommendations.” Examining the COVID Tracking Project’s map of the HHS release, one can zoom in on Dallas, say, and find data about how full any given hospital’s ICU is that week. It provides an unprecedented look at precisely how much pressure COVID-19 places on our health-care systems. The White House’s Coronavirus Task Force is now using this kind of information to dispatch medical support teams to hard-hit areas. This week, a new administration will take control of the HHS system, and is facing public pressure to change it once again. Switching back to the National Healthcare Safety Network, at this point, would likely undo the progress the HHS data team has made in the past six months, at the worst moment of the pandemic so far. “Going forward, it’ll be important for the next administration to pick up the baton and build off of what’s been created for this response,” Ryan Panchadsaram told me. “Is it perfect? No. But it is better than what we had before.” “My feeling is do not make any changes unless they are absolutely necessary,” Foster said. “Change is disruption.” from https://ift.tt/3iraIxx Check out http://natthash.tumblr.com For most of 2020, the coronavirus that causes COVID-19 jumped from human to human, accumulating mutations at a steady rate of two per month—not especially impressive for a virus. These mutations have largely had little effect. But recently, three distinct versions of the virus seem to have independently converged on some of the same mutations, despite being thousands of miles apart in the United Kingdom, South Africa, and Brazil. (A mutation is a genetic change; a variant is a virus with a specific set of mutations.) The fact that these mutations have popped up not one, not two, but now three times—that we know of—in variants with unusual behavior suggests that they confer an evolutionary advantage to the virus. All three variants seem to be becoming more common. And all three are potentially more transmissible. “Anytime when you have mutations that come up independently of each other in multiple places, it’s really a sign,” says Vineet Menachery, a coronavirus researcher at the University of Texas Medical Branch. Now scientists are scrambling to figure out if and how these mutations might give the viruses an edge. It’s still early, and data on the variant in Brazil are particularly sparse. In addition to sharing certain mutations, though, these variants simply have a large number of mutations, some unique to each variant. Gaining a whole suite of mutations quickly should be a very uncommon event. But with the virus so widespread right now, very uncommon events will happen—and will happen more than once. The usual two-per-month mutation rate may undersell how the coronavirus can mutate in unusual situations. “It’s a little bit of a wake-up call,” Kristian Andersen, a microbiologist at Scripps Research, told me. [Read: The coronavirus is evolving before our eyes] The role of each individual mutation is still unclear, but a particular mutation in the spike protein called N501Y is noteworthy because all three variants have it. The spike protein is how the coronavirus enters cells, and N501Y is in an especially important region called the receptor-binding domain, which latches on to the cell. An N501Y mutation may make the spike protein stickier, allowing it to bind to and enter cells more readily. Such a virus could become more transmissible. On the plus side, however, the mutation doesn’t seem to affect immunity from vaccines. Here’s how to read the names of the mutations, by the way: Proteins are made up of building blocks called amino acids. N501Y means that the 501st amino acid was originally an N, which stands for the amino acid asparagine, but has been changed to a Y, which stands for tyrosine. N501Y is not unique to these three variants, though; it’s been found in a number of sequences around the world. What is unusual about these three variants is that they also have an additional constellation of other mutations in other parts of the virus. A change in a variant’s behavior, such as increased transmissibility, is probably “due to not just one mutation, but multiple mutations,” says Emma Hodcroft, a molecular epidemiologist at the University of Bern. The U.K. variant has more than a dozen other mutations, which have not been scrutinized as much as N501Y. But the variant’s increased transmissibility is looking more certain: It’s growing more prevalent not just in the U.K., but also in Ireland and Denmark, two other countries that regularly sequence large numbers of samples. The CDC recently warned that it’s likely to become the dominant variant in the United States by March. (Scientists have given all three variants more specific names, but they have not, alas, standardized them yet. The U.K. variant is also known as B.1.1.7, and 20I/501Y.V1, and VOC 202012/01. The South Africa variant is sometimes called B.1.351 or 20C/501Y.V2. The Brazil variant is known as P.1 and 20J/501Y.V3.) The South Africa and Brazil variants also have a second and third mutation in common in the spike’s receptor-binding domain: E484K and K417. Scientists know a little bit more about the E484K mutation. It switches a negatively charged amino acid for a positively charged one; it’s like flipping a magnet. This likely changes the spike protein’s shape as it is binding to a cell, but this change seems to work in synergy with the N501Y mutation, Andersen said. These mutations, possibly along with others, may make the virus better at binding to cells. [Read: Why aren’t we wearing better masks?] But the South Africa and Brazil variants might have an additional advantage. A recent study suggests that viruses with the E484K mutation might be better at evading antibodies from the blood plasma of recovered COVID-19 patients. Some viruses with this mutation could become a little better at reinfecting people or even infecting vaccinated people. This one mutation alone is unlikely to render immunity from previous infections or vaccines totally ineffective, though. With current vaccines, “you have more than enough antibody, and even if you cut that amount in half, you still have more than enough antibody to control the virus,” Menachery told me. “If the new variant reduces the efficacy … by 50 percent, you still have a lot of protection there.” Studies are ongoing to figure out exactly how much this mutation affects vaccines, but it does suggest that vaccine makers might need to update their shots if more mutations like E484K accumulate over a period of years. This is already done every year with the flu shot, and the current mRNA COVID-19 vaccines can be updated especially quickly, in as little as six weeks, according to the manufacturers. Scientists now wonder whether the variants in South Africa and Brazil are spreading precisely because they have this slight advantage in overcoming previous immunity. Both variants were originally found in parts of the countries that have had high levels of COVID-19 infection--especially in Manaus, Brazil, where an especially large proportion of people have already had the virus. (One December study says 76 percent, which is probably an overestimate, but the region’s high COVID-19 death toll suggests that it indeed had a huge outbreak in 2020.) The South Africa variant is becoming dominant in the country; the situation in Brazil is less clear because less data exist, but Manaus is currently experiencing another big surge of COVID-19. Menachery said he doesn’t think previous immunity is necessarily a reason for these variants to become more common, especially because South Africa isn’t as close to herd immunity. Better transmissibility is already an advantage. [Read: The next phase of vaccination will be even harder] But others sketched this plausible, though still hypothetical, scenario: The variants may have evolved in immunocompromised patients who were infected with the virus for months. Normally, Hodcroft says, “your immune system is going to town on it. It’s really trying to beat it up.” But immunocompromised patients mount weaker immune responses. “It becomes almost like a training course for how to live with the human immune system,” she says. That may be why these variants have so many new mutations at once, as if a year or two of evolution has been compressed into months. This is probably quite rare, but with tens of millions of infections around the globe, rare things will show up. A variant could emerge, then, from the training ground of a chronic infection, with mutations that make the virus better at binding to cells and thus more transmissible. This may be what happened with the U.K. variant. It could also emerge slightly more capable of reinfection. This may be what’s happening in Brazil, where there are already two documented cases of reinfection with the new variant. In a place where many people have already been infected with COVID-19, a variant that is just a little better at evading preexisting immunity will have an advantage. These reinfections might not be serious, and they still might not be the norm, but over time, that variant will win out. The coronavirus is in a constant arms race against our immune system. It will keep evolving. That means our vaccines may need to evolve with it. But the United States is sequencing only a tiny percentage of its COVID-19 cases. (Standard COVID-19 diagnostic tests probe a few regions of the virus genome, but they don’t sequence the whole thing.) “San Diego is one of the places in the country we’re doing well, and we’re sequencing 2 percent of cases. It’s laughable compared to the U.K. and Denmark,” Andersen said. “And we need to change that.” The sequencing data, when they are collected, are fragmented across individual labs all over the country. What the U.S. needs, Andersen said, is a federal mandate for genomic surveillance. That’s the only way for the U.S. to keep abreast of an ever-changing virus. from https://ift.tt/35QF8Ed Check out http://natthash.tumblr.com What do I do now? COVID-19 diagnoses start with a barrage of grueling decisions and paralyzing worries. Did I infect anyone else? Whom will I tell? Where can I isolate? Should I go to the hospital? Will I be okay? Millions of Americans have fallen sick with this virus, and we’ve seen the full kaleidoscope of ways people react and cope with illness. Some have dutifully rung up contact tracers and locked themselves in total isolation. In March, after a 63-year-old man in Los Angeles broke out in coughing fits and couldn’t get hold of a coronavirus test, he spent five days quarantining in his 2009 Mercedes. Other people have been an epidemiologist’s worst nightmare. Someone in southern Oregon kept going to work after falling sick, super-spreading the virus and killing seven people. A groom in Texas reportedly tested positive one day and went on with his maskless wedding party the next. “Oh, no, no, no, don’t freak out,” a bridesmaid told the very freaked-out photographer. “He doesn’t have symptoms. He’s fine.” Then there’s a more curious response. Some people tuck away a bout of COVID-19 like it’s a deep, dark secret. Even among those who have been fully responsible about quarantining, at least a small number have decided not to tell their closest relatives—or their friends, or anyone at all—that they are sick in the first place. Long after they recover, they hide what they’ve been through, resorting to lies and subterfuge. It’s impossible to speculate about just how many COVID camouflagers are out there, given that, well, their whole aim is to keep their illness under wraps. I was able to connect with three of them, all on the condition of anonymity, to suss out why they made the call to hide a life-threatening illness from the people who most value their life. One Philadelphia father who got the virus in the spring confessed to me that his son still doesn’t know what he’s been through. He doesn’t want his 12-year-old chirping at his friends, “Dude, my dad got the ’rona,” he said. An anguished health-care worker in New York told me about the baggage from shrouding her illness from her mother and grandmother. Her mom went into full-on panic mode in March, blaming the pandemic on 5G towers and chemists, so why add to her hysteria? [Read: The coronavirus conspiracy boom] The grandest coronavirus cover-up I encountered, by far, came from Michelle, a flight attendant for a major airline who asked to be identified by her first name so that word wouldn’t reach her family. In late March, when most Americans were still settling into their year of quarantine and social distancing, Michelle was holed up in her Connecticut home for six weeks, battling a virus that robbed her of her sense of smell and taste, then her breath, and then strengthened its grip as it nearly put her in the hospital. Besides her boyfriend, a cousin, and one friend, no one knows what she’s been through. Since early June, she and I have had a series of long, meandering conversations about her illness. Before coming down with COVID-19, Michelle said, she never kept secrets from her family. She splits her time between Connecticut and Florida, where she lives right down the street from her parents in the same gated community. As a teenager, Michelle would always fess up after borrowing her dad’s car. She’s 60 years old now, and her parents have met every single man she’s ever dated. There was one fender bender a few years back that she didn’t tell them about, but she swears that’s it. That was before the pandemic. In late March, Michelle worked on a packed flight from Tel Aviv to the United States, and so many of the passengers seemed sick. Three days later, she knew something was wrong. “I had hallucinations,” she said. “I was really, really sick. I don’t think I had enough breath to even talk. I’ve had the flu before; that’s aches and pains. This is unbearable pain.” Her doctor sent her to a drive-through clinic for a COVID-19 test. She knew even before she heard the result: positive. Michelle put herself in full quarantine. Right away, she told her boyfriend, who lives nearby, that she had COVID-19 and wouldn’t be seeing him for a while. She stayed at home all alone as the virus clamped down on her body. When she lost her sense of smell, she would mistakenly let her dinner go in circles in the microwave until it burned up. When swallowing got tough, she forced herself to drink water. When the virus smothered her ability to speak, she settled on sharing the illness with a few more people, texting a friend and a cousin. “The friend was horrified, almost like she could catch it through the phone,” Michelle said. “Even in telling one person, there was so much judgment about everything. When I started getting better, I said, ‘Oh, I had a good day today. I was able to walk to the mailbox.’ And the friend was even judgmental about that, as if I was spreading it to the entire neighborhood.” Michelle was Zooming with her doctor all the time and following every recommendation, but her cousin lashed out, too, and said it all wasn’t enough. Michelle was confident that she hadn’t done anything wrong. She always washed her hands for the full 20 seconds. She never took her mask off in-flight. But haunted by the shame, she completely shut down. “In March, if you were COVID-positive, you were a leper,” she said. She’s the closest thing her parents have to a caretaker, so the last thing she wanted to do was rack them with worry that they might lose her. Michelle’s boyfriend nudged her toward the idea: What if you just don’t tell anyone else? [Read: A shift in family values is fueling estrangement ] She began to dodge her parents’ phone calls, enlisting her boyfriend as a co-conspirator who would call them back and lie. “Oh, Michelle’s just stuck in Connecticut for work, waiting for her next flight assignment.” When her nieces checked in on her, worried that she might catch the virus from all the flying, she would tactfully shoot off “Oh, everything’s fine” texts. Over the months, the minor fib has spiraled into Mrs. Doubtfire levels of deception. Now, long since Michelle recovered enough to fly again and head down to Florida, she still fears that if she tells her parents, “they’ll hear on the news that someone else tested positive after getting over it and they’ll be worried,” she told me. “I’m just going to let them think that I’m bulletproof and that I’ve dodged it.” She doesn’t even think about telling strangers or her co-workers. If two of the people she trusted most reacted so poorly, why would anyone else treat her better? No one hides an illness because they enjoy unleashing a cascade of lies. Sometimes, people think of what they’re doing as an act of kindness, says Meghan Moran, a health-communications scholar at Johns Hopkins University. “We’re constantly making decisions about what version of ourselves we want to present to others,” she told me. “Disclosing an illness could fracture the impression that people have of us. It’s giving up control.” Long before the pandemic, all sorts of people concealed all sorts of illnesses. Some of the writer Nora Ephron’s closest friends heard that she was sick with leukemia only a day or so before the disease killed her in 2012. One study in the United Kingdom found that 40 percent of gay men with HIV didn’t tell their family members about their diagnosis. But secrecy can also be motivated by one of the deepest-rooted myths around: that health is a sign of virtue, and infection a sign of sin. A particularly cruel dynamic of the coronavirus is that although everyone runs the risk of contracting it, those unlucky enough to fall ill can still feel the wrath of shame from those lucky enough not to. “It’s not surprising that people are scared of judgment when we’ve been telling them for months on end that if they take any risks, they are selfish, reckless, and irresponsible,” Julia Marcus, a Harvard epidemiologist and frequent Atlantic contributor, told me. “So of course when people test positive, their first reaction is, What did I do wrong?” [Read: The danger of assuming that family time is dispensable] From spring-break revelers in March to Thanksgiving travelers in November, risk takers have been cast as one of the pandemic’s arch villains. Some people really have acted pretty boneheaded during all of this, but risk takers aren’t the reason the United States has bungled its pandemic response to such world-historical proportions. Rather, since the beginning of this crisis, government leaders at every level have failed to proffer Americans the very things they need most in a moment like this: clear messaging on how to stay safe, and basic resources that will help them do so. In that vacuum, Americans have only one thing left to protect themselves: personal responsibility. For the most part, “people are making rational decisions with the information they have,” says John Pachankis, a public-health professor who runs Yale’s LGBTQ Mental Health Initiative. With all the stigma around the coronavirus, Pachankis told me, COVID camouflaging reminds him of an entirely different phenomenon: staying in the closet. People don’t conceal who they are because of some spur-of-the-moment brain fritz, he said. They do so after endlessly running the cost-benefit analysis in their head and deciding that telling the truth is just not worth it. Still, even after weighing the options, the deception is never easy. Over the months that Michelle and I have talked, I’ve sensed the mounting stress and torment of having to harbor her secret. Simply keeping up the ruse all the time seems to be draining, after everything the disease did to her. She’s thankful that she’s not one of the tens of thousands of American airline workers who have lost their job during the pandemic, but she said she still has trouble catching her breath on the job, especially when she’s playing Tetris by rejiggering luggage in overhead bins. Her taste and smell flipped back on in May, but her love of food and cooking never quite did. Clumps of her hair are mysteriously gone. The virus “just ravaged me and my looks,” she said. For the first time in her life, she has crippling migraines that have her frequently popping aspirin. Before, going over to her parents’ place was just a quick little walk. Now she says it requires an elaborate game of dress-up to hide the scars of COVID-19. She blankets herself in makeup, and even though she’s tested positive for antibodies and doubts she can spread the virus, she puts on a mask and never takes it off. Her parents are deep into their 80s, and recently they’ve needed more help around the house. Michelle used to pick up the slack, ascending a ladder to clean out the gutters and tightening the loose shower handle. “Now I just can’t do it,” she admitted. The last time we talked, in December, Michelle was stewing that her parents might finally be on to her. “Why not just tell them?” I asked her. She didn’t hesitate. “As long as I can get away with not telling anyone else, that’s what I plan on doing,” she said. She’s simply started spending less time in Florida with her family to escape from it all. from https://ift.tt/2XLLlwz Check out http://natthash.tumblr.com After a new variant of the coronavirus spread throughout the United Kingdom, daily cases hit record levels and the prime minister ordered a national lockdown. Now more mutations from South Africa and Brazil have made headlines. The prospect of a more transmissible virus has many worried, but exactly how bad are these new mutations? And should you change anything you’re doing already? Vineet Menachery, a virologist at the Galveston National Laboratory who studies coronaviruses, joins staff writer James Hamblin and executive producer Katherine Wells on the podcast Social Distance to explain. Listen to their conversation here: Subscribe to Social Distance on Apple Podcasts, Spotify, or another podcast platform to receive new episodes as soon as they’re published. What follows is a transcript of the episode, edited and condensed for clarity: Katherine Wells: My understanding is that virus mutations happen all the time. And the lesson I learned in the early days of this pandemic was: Don’t worry about them too much because it’s normal, and it doesn’t mean it’s worse just because it’s mutated. These latest mutations in the news seem different and more worrisome, but I don’t understand why. Are they in fact different and more worrisome than all the previous evolving mutations? Vineet Menachery: The quickest answer at this point is: We don’t know yet. The mutations that we think about are twofold: There are mutations that allow the virus to replicate or transmit better. These are worrisome because obviously that just changes how fast this virus can spread. And that’s one of the concerns for these variants. There’s the U.K. variant. There’s a South African variant. And, most recently, there’s a variant in Japan that’s been traced back to Brazil. Each of these have a mutation at a position in the spike protein that are associated with, potentially, an increase in transmission. Wells: Can you help me visualize it? It’s like the spike is spikier and therefore stickier, or something? Menachery: The analogy I would make is that it’s like a key. And the spike protein has to fit to its key. Now you can think about a key in a lot of different ways, but the better that key fits, the more efficient and transmissible the virus is going to be. These new variants may actually fit that key better. And that allows the virus to replicate or transmit a little bit better than the previous versions. And that’s what’s concerning. Wells: So this particular mutation wouldn’t mean that it hangs longer in the air or that it is better at sticking to your skin or something. It just means that, once it is in your body, it is better at actually latching on to the cells that it needs to infect you. It’s not actually that it’s easier to get into your body. It just is more likely to infect you once it’s inside. Menachery: Yeah, I think it gets back to efficiency. Now, we don’t know anything for sure, but the barriers that are in place [such as] masking and social distancing will still be effective against this. The virus hasn’t changed fundamentally. It’s a small difference in a molecular aspect of the virus that gives it a little bit of an advantage. We think, based on the math, that it does have an advantage over the original, but we don’t know the scale at which it has an advantage. Is it 10 times worse or is it two times worse? Both viruses, the original and this version, are pretty transmissible. And so if it’s two times worse, you may not be able to see the difference. If it’s 10 times worse, you’ll see that in terms of how quickly the virus spreads. Wells: How do we figure that out? Menachery: There are a bunch of different ways, and none of them are particularly great. There are experimental ways. Scientists here, and around the world probably, will take the different variants and put them into animals in direct competition. We’ll take the original and the new variant, mix them together, and put them in animals to see how well they transmit [and] how well they replicate. Wells: Is that what you’re doing now? Menachery: People in our group are doing that experiment as we speak. Wells: What animals? Menachery: We’ll be doing them in hamsters. I imagine groups will try to do it in ferrets, and maybe even in mice. Each of these models are useful in their own way, but none are ideal because none of them are really human. James Hamblin: When you hear a number, like what was widely reported out of the U.K., like “70 percent more transmissible”—which I believe made it to a push alert from The New York Times and is widely cited—do you think it’s premature to put a number like that on it, or do you think that’s an accurate ballpark [figure]? Menachery: The number is accurate in the context of the viruses that are spreading in the U.K. So that’s just based on what they’re surveying and the total numbers. You can see that it is becoming a great part of the population very quickly. But it’s hard to gauge. You have the original virus, and you’re comparing it to this other virus. And it’s moving faster, but we can’t control for other aspects. The virus may be moving through a population faster than it was in the summer because of the temperature or the conditions or the lockdowns or how [lax] sick people are with their masking. There are so many factors that contribute to that. It does appear, based on just the pure mathematical numbers, that the strain is moving faster and is more transmissible. But again, we don’t have a relative scale to know how much more transmissible it is than the original. Wells: How do I, as a person trying to just get through this, internalize this news? There are two concerns: Do I have to change my behavior? And should I be worried about vaccines? I’ve developed an understanding of how this transmits, a way of behaving, a risk tolerance that involves mostly being very worried about being not masked with people close and kind of being aware of surfaces, but everyone tells me surfaces aren’t really how it transmits. Does this raise the stakes of any of my day-to-day behaviors? Menachery: I don’t believe so. The precautions you’re taking should still keep you safe. The virus is not structurally different. It’s these small changes at the molecular level. But it is a situation where, if you’re unmasked, you may be at a greater risk of getting infected from that same person. We don’t know how much more, but if you’re in contact and don’t have the same level of precaution as before, you’re going to be at a greater risk with these new variants. Hamblin: As I understand it, viruses can become more transmissible by either being more efficient—that key being better able to enter a cell—and/or increasing the viral load within a person. So when you are carrying this virus, you just have more within you and you therefore have more that’s able to infect other people. Are there possibly other effects of that? [If it causes] a higher viral load, people might develop symptoms differently or the disease might manifest differently. Could that have other good or bad consequences that would change the course of the pandemic? Menachery: The worry would be: If you’re increasing the viral load, the virus is replicating better and that might cause more severe disease. We haven’t had any evidence that these new variants cause more severe disease. And this gets to a weird aspect of disease and transmissibility. If you get really sick, you actually don’t transmit the virus all that well because you’re really sick and you don’t interact with the same number of people, whereas a virus that causes less disease might actually be more transmissible in a sense, because, since you don’t feel as bad, you’re more likely to transmit it to other people. So there’s a bit of a dichotomy in how viruses spread. This particular COVID-19 is kind of this Goldilocks of viruses. If it was a little bit more severe, it would be easier to control. If it was a little bit less severe, it wouldn’t be as disruptive. And so, in the same sense, these variants could push in one direction or the other. So far, we haven’t had any evidence from the human data that there’s more severe disease associated with it. But often it takes three or four weeks for that data to come in. Coronavirus doesn’t kill in three or four days. It takes three or four weeks. And so, we may be just getting some of that information now. And then the studies we’re doing in hamsters and in mice will also give us some insight. When we compare the variant to the original, we’ll see how sick those animals get and really look at how much disease and how much damage the new variant causes, relative to the original viruses. Wells: What is your level of worry right now? Menachery: On a scale of one to 10, I’m probably at a three or a four at this point. There are certain mutations that are more important than others. Some are related to transmission. And these variants are coming up in a population of people [where] the vast majority of people don’t have any immunity. These variants we’re seeing haven’t been pushed to evolve away from antibodies yet. Your antibodies may be not as effective, but they’re still going to be effective. If you have 10 times the amount of antibody that you need and you lose half of that, you’re still going to be well protected. And I think that’s where these variants are. Most people will be well protected from the worst aspects of disease. Hamblin: Is the virus going to become more transmissible and eventually infect us all but cause less severe disease? Do we have any idea of the overall arc of this narrative that’s just starting to unfold? Menachery: It’s hard to say, obviously. What you’ve described is something that may have already happened in the natural world with common coronaviruses. There are four or five common-cold coronaviruses. Many of them have their roots in animals, whether they be bats or cows or other animal species, and then jumped into humans. None of those viruses cause severe disease. They’re all relatively transmissible, and you can get infected every two or three years with them. There is some possibility [SARS-CoV-2] will go along that route. Once we’ve all gotten some level of baseline immunity—we’ve seen a virus like this or very similar to this—the next time you have it, it [may cause] a mild infection but, for the most part, you won’t end up in a hospital or on a respirator. That’s kind of the trajectory that you could expect, but again, we don’t know. This event could have happened in 2002 with [SARS-CoV-1], but that virus was effectively stopped through quarantining and other procedures. We have an event now where most of the world will have seen this virus, either through a vaccine or through natural immunity, and so its trajectory in a few years is really hard to predict. I’m hopeful that it’s going to be more like a common-cold coronavirus. The best outcome would be that it’s like SARS 1 and it just disappears from the Earth. from https://ift.tt/35KbpN9 Check out http://natthash.tumblr.com |
Authorhttp://natthash.tumblr.com Archives
April 2023
Categories |

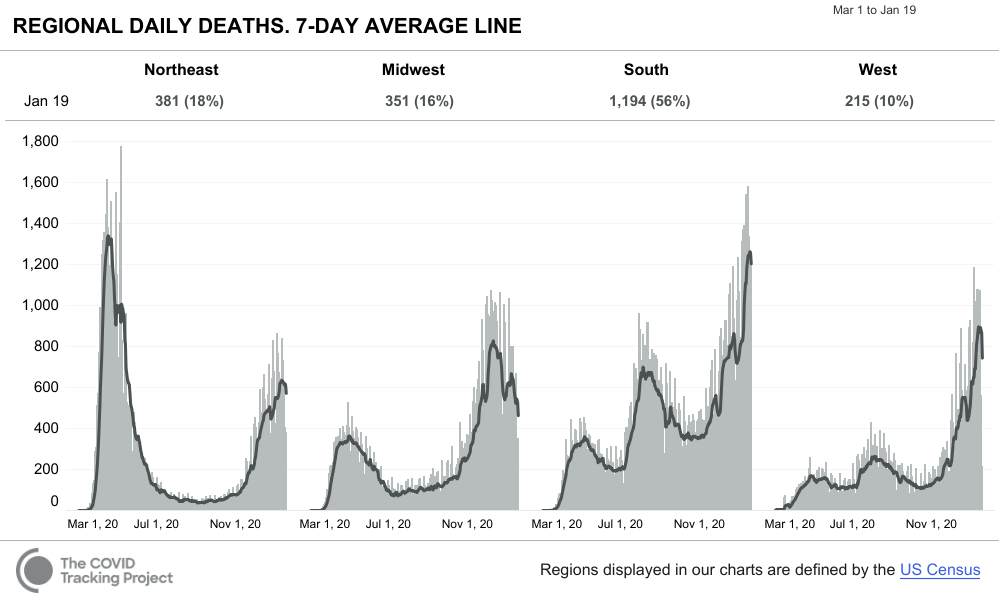
 RSS Feed
RSS Feed
