|
Last June, as the Delta variant sat poised to take the globe by storm, Pfizer’s CEO, Albert Bourla, promised the world speed. Should an ultra-mutated version of SARS-CoV-2 sprout, he said, his company could have a variant-specific shot ready for rollout in about 100 days—a pledge he echoed in November when Omicron reared its head. Now, with the 100-day finish line fast approaching and no clinical-trial data in sight, the company seems unlikely to meet its mark. (I asked Pfizer about this super-speedster timeline; “when we have the data analyzed, we will share an update,” the company responded.) Moderna, which started brewing up an Omicron vaccine around the same time, is eyeing late summer for its own debut. Not that an Omicron vaccine would necessarily make a huge difference, even if Pfizer had made good. In many parts of the world, the variant’s record-breaking wave is receding. Having a bespoke vaccine in 100 days would have been an unprecedented accomplishment, but Omicron was simply “too fast” for a cooked-to-order shot to beat it, says Soumya Swaminathan, the chief scientist at the World Health Organization. This time, all things considered, we got lucky: Our original-recipe vaccines still work quite well against the variant, especially when they’re delivered as a trio of jabs—enough that some researchers have wondered whether we’ll ever need the elusive Omivax. But Omicron won’t be the last antibody-dodging variant that splinters off of the SARS-CoV-2 tree—which means the vaccines, too, will need to keep coming. Tough decisions are ahead about what triggers might prompt a whole new variant-specific vaccine campaign, and how we’ll manage the shift in time. That said, we don’t have to resign ourselves to a bleak future of infinite catch-up, with shots always lagging strains. Vaccine updates might not be that necessary that often, and when they are, we can poise ourselves to rapidly react. Rather than scrambling to sprint after SARS-CoV-2 every time it surprises us, we could watch the virus more closely, and use the intel we gather to act more deliberately. To vaccinate properly against a variant, we must first detect it. That means keeping tabs on the coronavirus and rooting out the places where it likes to hide and transform. Flu presents an excellent template for this sort of viral voyeurism. The viruses that cause that disease also shape-shift frequently enough to elude of the immune system’s grasp. For decades, scientists have been maintaining a massive, global surveillance network, now made of some 150 laboratories, that each year amasses millions of samples from sick people and susses out the genetic sequences of the viruses that linger within. That information then goes to the WHO, which convenes two meetings each year—one per hemisphere—to decide which strains should be included in next winter’s vaccine. A watchdog system for SARS-CoV-2 could piggyback off of flu’s. The symptoms of the two diseases overlap; hospitals are “already collecting those samples,” says Richard Webby, the director of the WHO Collaborating Center for Studies on the Ecology of Influenza in Animals and Birds. “You’d just test them for two agents now.” Scientists could scour coronavirus genomes for little red flags—big-deal changes in the spike protein, say, that might befuddle antibodies—then shuttle the most worrisome morphs to a high-security lab, where they could be pitted directly against immune molecules and cells. Based on flu’s model ideal candidates for a vaccine revision might meet three criteria: They’re riddled with unusual mutations; they’re recognized poorly by antibodies; and they’re spreading at least somewhat rapidly from one person to the next. A variant so heavily modified that it “overcomes our immunity enough” to make even healthy, vaccinated people quite sick would make the clearest-cut case for editing a shot’s recipe, Swaminathan told me. [Read: The coronavirus will surprise us again] In September, the WHO formed a new technical advisory group that’s been tasked with recommending ingredient adjustments to COVID vaccines as needed; Swaminathan envisions the committee operating parallel to one that calls the shots for flu. But over time, the conditions that demand we take quick action for COVID vaccines might not arise all that often. At least some coronaviruses are thought to metamorphose more slowly and less dramatically than flu viruses, once they settle into a population, which could mean a less frantic variant pummel than what we’ve experienced so far. Some experts also hope that as the world continues to rack up infections and vaccinations, our immunity against this new coronavirus will hold better. Our defenses against flu have always been a bit brittle—vaccine effectiveness for these shots doesn’t start terribly high, then drops rather rapidly. If our shields against SARS-CoV-2 are more stalwart, and the virus genetically quiets, perhaps we will need to rejigger COVID vaccines less often than we do for flu. Even against Omicron, the most heavily altered variant of concern identified to date, vaccine protection against severe disease seems extraordinarily sturdy. “I don’t think the entire population is going to need annual vaccines,” Swaminathan told me. (The important exceptions, she noted, might be vulnerable populations, among them immunocompromised people and older individuals.) And when we do need vaccine revamps, the blistering speed at which mRNA shots can be switched up will be an advantage. Because most flu vaccines need about six months to slog through the production pipeline, vaccine strains are selected at the end of winter and injected into arms the next fall. That leaves a gap for the viruses to morph even more. mRNA shots like Pfizer’s and Moderna’s, meanwhile, could—Omicron saga notwithstanding—zing from conception to distribution in about half the time, and eliminate a good chunk of the guesswork. Some parts of this relatively rosy future may not come to pass—or at least, they could be a long way off. We just don’t understand SARS-CoV-2 as well as we do flu viruses. In most of the world, flu viruses tend to wax in the winter, then wane in the warmer months, giving us a sense of the optimal time to roll out vaccines. And flu evolution occurs in a linear, ladderlike fashion; last year’s major strains tend to beget this year’s major strains. That makes it reasonably straightforward to “predict the direction that flu viruses are going in” and design our vaccines accordingly, says Emma Hodcroft, a molecular epidemiologist at the University of Bern. The evolution of SARS-CoV-2, meanwhile, so far looks “more radial,” Webby told me, with new variants erupting out of old lineages rather than reliably riffing on dominant ones. Omicron, for instance, wasn’t an offshoot of Delta. “If we saw ladderlike evolution, we would know we need an Omicron vaccine now,” Florian Krammer, a flu-virus expert at the Icahn School of Medicine at Mount Sinai, told me. “That’s not what we have seen.” The coronavirus has also so far been serving up new variants at an absolutely staggering clip--far faster than virologists expected it to at the pandemic’s start—and scientists are unsure whether that churn will stop. The coronavirus may eventually settle into more flu-like patterns—trending its evolution to be more stepwise than starburst, or sticking to winter waves—as population immunity grows and it learns to better coexist with us. Host defenses, when they’re strong and abundant enough, have a way of constraining which paths a virus can take; perhaps they will slow the speed at which new variants arise and take over. “The hope is that we head toward seasonality and stability,” Helen Chu, a flu-vaccine researcher at the University of Washington, told me. But there’s no telling how long that transition will take, or how bumpy it will be, or if it will occur at all. Chu also worries that we don’t yet have the proper infrastructure to pinpoint variants that gain steam in places where they can mutate unusually quickly: people with weakened immune systems, perhaps, or animals that can contract the pathogen and boomerang it back. (Similar events for flu, wherein other species pass a foreign version of the virus to us, can cause pandemics.) SARS-CoV-2 is unlikely to prefer exactly the same real estate that flu viruses do, and so our surveillance strategies will need to look different too. Even flu monitoring has notable holes: It still lags, for instance, in low-resourced parts of the globe. “We need eyes and ears everywhere,” Swaminathan told me. For at least the short term, our COVID-vaccine-update process is likely to remain a bit plodding; variants will crop up, and our shots will pursue them. Even late-arriving shot rewrites aren’t necessarily useless, Hodcroft pointed out. Say our next variant is an Omicron descendant; dosing people up with Omivax could still prep the body for what’s up ahead, even if the shot arrives too late to prevent past surges. That said, we’ll also have to be careful about going all in on Omicron; several experts recently warned me that it’s probably premature to totally trash our original-recipe shots. “If we went straight for an Omicron vaccine and stopped the others, that could potentially open up an immunity gap for the ancestral strains” to mutate, and their descendants to roar back, says Cheryl Cohen, a member of the WHO’s technical advisory group on COVID-19 vaccines and an epidemiologist at the National Institute for Communicable Diseases, in South Africa. [Read: Should we go all in on Omicron vaccines?] The pitfalls of pivoting from one spike version to the next are part of why this “whack-a-mole approach” of chasing single variants must end, says Raina MacIntyre, a member of the WHO’s technical advisory group on COVID-19 vaccines and a biosecurity expert at the University of New South Wales, in Australia. Ideally, future vaccines should protect, with a single injection, against multiple variants at once. An easy first step would be to combine multiple spikes into one shot—an Omicron-original combo, say, or an Omicron-Delta-original triple threat. Eventually, we might hit upon a universal formula that guards against all variants, including ones we “don’t know about yet,” Hodcroft said. If the flu’s any indication, that could be an enormous challenge: Even after many years of study, we’ve struggled to find a catch-all shot for that disease. With SARS-CoV-2, we don’t yet have a strong enough sense of all the evolutionary paths the virus could take; we may not be able to execute a wider-range shot until we understand our enemy better. Still, with so many efforts in the vaccine pipeline, Swaminathan is optimistic. “I am fairly confident it is scientifically feasible,” she said. “It is no longer, ‘Can we do it?’ It is, ‘We can.’” from https://ift.tt/KGsRnZP Check out http://natthash.tumblr.com
0 Comments
Several years ago, Paul Farmer and I both spoke at a conference at Harvard on the history and future of global health. As our program finished, Paul was immediately inundated with a throng of students eager to speak to the guru of the field, the man who inspired us all and asked more of each of us. I shuffled off to speak to the few avoiding the crowd. After Paul finished with the students, he came over to give me a hug, and we made small talk. Then he asked for a favor: Could he borrow a pair of socks? “Socks?” I asked. “Why yes,” he said, as if socks were a totally normal thing to be in need of in a lecture hall. He was in Boston briefly, stopping on his way from Geneva to Rwanda, and he had exhausted his supply. I walked over to my briefcase, pulled out a pair of socks, and handed them to Paul; he quickly put them away. For years, I often carried an extra pair if I was going to see Paul, especially when he was just passing through town. He was so deeply focused on the people around him and making the world a better place that he often forgot what he needed to put on his own feet. Paul was the creator of the modern global-health movement. He was a founder of Partners in Health, which changed the way we all understood what it means to care for the world’s poor. In service of this role, he was a world traveler, always on the road, preaching his message of caring for all. Many of us who loved Paul had at least one occasion to “lend” him socks, knowing there was little risk of ever seeing those socks again Paul passed away yesterday, a shocking and devastating blow to his friends and the generations of people inspired by his work. Throughout his life, he fought against a counterproductive mindset that has haunted efforts of global health. The field that started as “tropical health” had been deeply rooted in the colonial context of caring for the subjects of Western rule. As European powers left their colonies in the global south, the nomenclature of the field changed to “international health,” but the field kept that deeply colonial framework--we the anointed global north providing charity for the uncivilized global south. Even now, the field often views its work from a perspective of constraint. With the limited resources we have, what is the most good we can do? Paul hated that question. He preferred to flip it on its head: Given all the good we can do for our fellow humans, what are the resources we need to make it happen? He was unconstrained by small thinking. He rejected the artificial limitations we put on caring for the world’s poor—limits we would never put on ourselves or our families. He refused to accept the soft bigotry of low expectations. When HIV was devastating Haiti, the standard response in public health was to write off people, saying HIV therapies were too expensive and difficult to deliver to the world’s poor. So Paul set out to prove everyone wrong. He set up clinics and hospitals with a simple goal: deliver the same quality care that he provided when he was caring for patients in Harvard’s teaching hospitals. It wasn’t an easy task, but it worked. Tens of thousands of people received the latest HIV care. So many lives were saved. Paul brough this approach to TB in Peru, to Ebola in West Africa, and to COVID-19 in the United States. In so doing, he built a new model of global health—one that begins not with constraints but with needs. It means asking what will allow people to lead healthy, productive lives and then, in Paul’s case, spending every second of his days generating the resources, assembling the systems, and training the people needed to deliver it. The work is hard, making things that don’t exist and convincing people of that what feels aspirational is actually doable. But it’s the only way forward in a world so connected. As two years of the coronavirus pandemic have made glaringly clear, people acting only in their own self-interest hurts us all in the long run. Paul understood that the world’s health is our health. We must all care for one another—anything less was morally unacceptable. Paul inspired generations of medical and public-health students and practitioners to reach beyond their self-imposed limitations and do more. That day at Harvard, I spoke about the future of global health. While the words were mine, the ideas and sentiments had been deeply shaped by Paul. I talked about how the future of global health must begin with the notion that all lives have value. That high-quality care that preserves human dignity is not a privilege of the few but the right of all. At a different time, in a different context, those words might have felt lofty or untethered to the difficult reality on the ground. But sitting next to Paul, those were the only words that made sense. He showed all of us what was possible. A few pairs of socks were the least I could give him in return. from https://ift.tt/MGBdeyV Check out http://natthash.tumblr.com When I found out this morning that Paul Farmer had died, I thought first of his wife, Didi, and their three children. I thought of his colleagues, and of everyone whose life was saved or changed for the better by him. And then I thought of all the people who know and care about global health because of Paul, far too many to count. Paul is a hero, and I was fortunate to call him a friend. Although we crossed paths at various conferences over the years, the first time I really got to hang out with him was during a trip to Cange, a small town in central Haiti with Melinda in 2005. We were there to visit a health clinic run by Partners in Health, the incredible organization that Paul co-founded (and that our foundation is proud to support). At the time, PIH was providing world-class healthcare to people in Haiti, Peru, and Russia, although it’s since expanded to eight more countries. Paul was the chair of the Department of Global Health and Social Medicine at Harvard, and he devoted his life to providing high-quality health care to the world’s poorest people. I’ve visited a lot of rural health clinics through my work with the foundation. I’m always blown away by the remarkable and dedicated people working at them, but Paul was special even among such peers. He was able to connect with his patients in a way that would be exceptional for any doctor, but was especially so for a gangly white guy from the Berkshires working in rural Haiti. He was a teacher who loved educating his students, whether they were future doctors studying at Harvard Medical School or community health workers-in-training at one of PIH’s clinics. But the thing that always stood out to me most about Paul was his single-minded focus on helping people in the world’s poorest countries. In Tracy Kidder’s book Mountains Beyond Mountains—which I can’t recommend highly enough if you want to learn more about Paul’s career—there’s a story about a young child whom Paul and his team treated for drug-resistant tuberculosis in Peru. After the boy was discharged from the hospital, his mother approached Paul to thank him as he was getting into his car to head home. Paul responded in Spanish, “For me, it is a privilege.” He was never happier than when he was caring for patients in one of the clinics he helped create. I have never known anyone who was more passionate about reducing the world’s worst inequities in health—or who did more to live by his values. Even as Paul’s reputation as a global health hero grew, his focus never wavered from helping people directly on the ground. He was a humble man who never had any interest in seeking attention unless it would make life better for the people he served. I remember meeting with one of his patients during that first visit to Haiti. The woman spoke Creole, so Paul had to translate for us. At one point, she launched into what was clearly a long story about him—I could hear the words “Doktè Paul” mentioned several times. When she finished, I turned to Paul and asked what she had said. He sheepishly replied, “Just some obligatory praise for me.” The only time Paul sought the spotlight was when he knew he had an opportunity to highlight inequality and speak to the next generation of global health leaders. He gave many commencement addresses over the years, and I suspect he is the reason a lot of young people have entered careers in public health. He is one of the most inspirational people I’ve ever met. His ability to inspire was one of the reasons why, when Melinda and I went back to visit Paul in Haiti in 2014, we brought our children with us. Although his work was his life’s joy, he was a wonderful person to be around when he was off the clock, too. I have fond memories of visiting his modest house in Haiti, which had a lovely garden that he was proud of. One of my favorite Paul stories happened when I traveled to visit PIH’s facilities in Rwanda. After our meetings were done, we decided to visit the mountains nearby to see the gorillas—but Paul hadn’t brought a change of clothes with him. I’ll never forget the image of Paul trekking up the steep misty hillside wearing a suit and tie. There will never be another Paul Farmer. I will miss him deeply. I am comforted by the knowledge that his influence will be felt for decades to come. His work will continue through Partners in Health, and it will be carried on by the many people he trained and inspired. At the end of the day, though, Paul’s most lasting impact can be found in the patients he loved so dearly—all of the mothers, fathers, sons, and daughters who are alive today because Paul dedicated his life to helping them. I can’t imagine a more phenomenal legacy. from https://ift.tt/qzwR8Wf Check out http://natthash.tumblr.com When the mayor of Washington, D.C., announced changes to the city’s mask mandate last week, spit hit the fan. As of March 1, District residents will need to cover up in order to attend school, go to a library, or ride in a taxi. But gyms, sports arenas, concert venues, and houses of worship—you know, all the places where people like to breathe hard or sing and shout in close proximity—will be facial free-for-alls. If the goal of mask policies is to reduce transmission of the coronavirus as much as possible, then D.C.’s new rules are difficult to reason out. Why should children, who are generally at low risk of severe disease, have to mask while sitting quietly in class when their more vulnerable elders can sing, unmasked, in church? It seems arbitrary, inconsistent, absurd. Then again, so does just about every community mask mandate. If the rules don’t apply equally in different settings, they’re unfair. If they do, they’re ridiculous: Good luck complying in a restaurant, bar, or airport food court. Pointing out the logical flaws in mask mandates is easy. Fixing them is hard—and important. Cases may be trending down in nearly every part of the United States, but this surge will almost certainly not be our last, just as Omicron will almost certainly not be the last variant to infect the world. When infection rates begin to rise again, local and state governments can try to implement mask policies that actually make sense to the people being ordered around. Take my city, Baltimore, as an example. Everyone older than 2 must wear a mask “indoors at any location other than a private home,” including at “foodservice establishments.” Yet indoor dining, which is associated with increasing COVID-19 transmission rates, has been allowed for more than a year, and diners do not need to be vaccinated. Performers are allowed to sing, speak, and play the oboe sans mask, despite the fact that maskless music has been known to be a potent source of contagion since the early days of the pandemic. I frequently walk past restaurants with MASK REQUIRED FOR ENTRY signs taped to the front door and their windows fogged up from the breath of maskless patrons. And in spaces where masks are both required and feasible—say, pharmacies and grocery stores—hardly anyone is enforcing their use. [Read: The Texas mask mystery] It all feels rather performative and silly. Why have a mandate if it can be so easily ignored? “The public sees right through that, and I think that’s led to a lot of the backlash,” Joseph Allen, the director of Harvard’s Healthy Buildings program, told me. To Allen, mask mandates’ contradictions and compliance failures are signs that the U.S. should stop trying so hard to influence human behavior, and start focusing on improving ventilation and filtration in buildings. Masking, because it’s obviously visible and has become unavoidably politicized, is the pandemic-mitigation strategy that’s easiest for most people to notice—which might explain why it’s received so much attention from the public and the media. But structural improvements can operate in the background, protecting people without making them feel inconvenienced. One common (though not definitively proven) argument against mask mandates is that they don’t actually change people’s behavior: People who would’ve masked anyway cover up, and people who don’t want to mask wear theirs badly or ignore the rules. “Anyone who has been in any sort of public location at any time during the pandemic recognizes that mask mandates are not followed consistently,” says David Dowdy, an epidemiologist at Johns Hopkins University. But even disregarded mandates could affect people in other, helpful ways. “From my perspective, the main benefit is not so much the masking itself, but the message to society that this wave is not yet over,” Dowdy told me. A mask mandate may not magically swaddle the faces of everyone in its jurisdiction, but it could remind already enthusiastic maskers to avoid large gatherings, or lead non-maskers to give the people around them a little more space. [Read: The case against masks at school] Mask mandates are easier to enforce in highly controlled environments, such as schools. A particular state’s or city’s values and political makeup matter for compliance too. “If it’s a community in which most people are already going to mask and you just need to convince a few more, in that case a mandate actually might be beneficial,” says Tara Kirk Sell, a senior scholar at the Johns Hopkins Center for Health Security. Such communities are widespread: About two-thirds of Americans have consistently supported the idea of a state or local mask mandate since August, when a bimonthly Axios/Ipsos poll first started asking the question. The other 30-something percent of the American public likely includes people who have lost faith in mask mandates that don’t seem to make sense. The way for decision makers to earn back their trust, Kirk Sell told me, is by listening to each community, taking their needs seriously, and tailoring policies to fit them. A town whose top priorities are keeping schools open and local business afloat could mandate masks and testing in schools, but allow adults to go mask-free in bars, which students can avoid. A town that wants to avoid straining its hospitals might flatten the curve by enforcing mask requirements in high-capacity settings such as concert halls and sports arenas. If rules are going to be applied unevenly—with mask mandates in some locations but not others—the tightest restrictions should apply in buildings such as grocery stores, workplaces, post offices, and schools, says Anne Sosin, a public-health expert at Dartmouth College. These are not necessarily the places where the virus is most likely to spread, but elderly and immunocompromised people may not be able to avoid them as easily as they could a bar or a hockey game. “I think that people have this expectation that everything has to be perfect, as far as how the logic works together,” Kirk Sell said. But no mandate is ever going to be perfectly consistent, and that’s okay. Mask policies can still make sense, so long as they serve a community’s shared goals. from https://ift.tt/dJoc0yR Check out http://natthash.tumblr.com Ryan McAdams, a neonatologist in Madison, Wisconsin, had a complex case to handle: A tiny newborn with a heart defect needed surgery. The baby had been struggling to feed, so doctors planned to insert a gastronomy tube directly into the stomach to assist in supplementary feeding. The baby’s mother was around all the time to care for the infant, until she tested positive for COVID-19 and wasn’t allowed to be in the hospital. The baby wasn’t feeding as well without the mom there, McAdams says. When the mom’s isolation period officially ended, at midnight before the scheduled procedure, she rushed back to the hospital. She told McAdams the agony she had experienced at home, sobbing as she watched the cribside camera set up to see her baby. “She just kept saying, ‘I wanted to be there,’” he says. “It was heartbreaking.” As a part of the hospital where babies are sent when they are very sick—perhaps because they have trouble breathing after birth, or because they were born far earlier than expected—the NICU has a special role. Patients sometimes stay for months, cared for by nurses and parents who must inevitably take breaks, coming and going from this isolated world. And in that shuffle, Omicron found openings. As case rates rose, caring for babies in the NICU became more complex, and families struggled to keep up with changing policies. No one ever plans on spending time in a NICU, but one in 10 babies ends up there, says Rachel Fleishman, a neonatologist in Philadelphia. Most commonly, babies head to the NICU because their transition from the womb to the world outside did not go well, even after a full term of gestation, Fleishman says. Preterm babies, as small as your hand, as light as a can of soda, might need longer stays. The babies are attached to a maze of machines and wires, and tubes in their mouth. “You’re the parent, but you’re also an observer, and you can’t fix things,” McAdams says. “It’s a really stressful, formidable environment that you’re thrown into.” It has never been harder to be a NICU parent than now, says Rochelle DeOliveira, the director of peer support at the nonprofit Project NICU, whose son spent 97 days in the NICU. “The concerns NICU parents have always faced—sickness, visitors, hand-washing, isolation—have been hallmark aspects of the journey long before this pandemic,” she told me. But now they have become even more overwhelming and controlled. [Read: The coronavirus will surprise us again] She says the project is still hearing stories of parents who are not permitted to remove their masks or gloves when holding their babies; restrictions, in some hospitals, are still so stringent that grandparents have never been permitted to see their grandchildren. Meals in the family lounges, lactation and other support groups, and additional opportunities to connect with other parents in the NICU have been eliminated too, DeOliveira said. Parents might live like this for months—some babies stay in the NICU that long. The goal for most of that time is simply to keep the babies alive until they’re strong enough to go home, McAdams says. “We have these fragile little babies who are like these little warriors, you know, fighting for their lives and have all these struggles against them.” Until recently, COVID was not usually one of those struggles. “It was pretty rare to have a baby with COVID, let alone a baby that was sick with COVID,” McAdams says. That situation sometimes made him feel guilty—he was caring for all these babies, while his colleagues were managing an onslaught of death and serious illness in adults in the next wing over. The mood could grow ominous, Fleishman says, hearing alarms and codes go off several times a day in the adult ICU. All of that has changed with the recent Omicron surge. Now the NICU where McAdams works is seeing more babies testing positive, more symptomatic babies, and many more parents with COVID. “We’re back to wearing not only surgical masks, but N95 masks and eye protection.” The hardest part of the surge has been separating parents from babies after a parent tests positive for the coronavirus, Fleishman told me. She has seen parents who were essential workers separated from their infants, aching for their caramel smell and velvety skin, and mothers who risked losing their milk supply and pumped with such dedication that their nipples bled, asking her: “When will I get my baby back?” “That separation is really heart-wrenching for us as physicians; it’s very challenging for families, for the nurses as well.” She says she ends up calling the families often with positive updates on the baby, and they can also monitor through a cribside webcam. But none of that makes up for not being there, for the mother or the baby. Caregivers and infants are really a dyad—their outcomes and health play into each other’s, Clayton Shuman, a maternal-infant-health researcher at the University of Michigan, told me. When an infant in the NICU is ill, that illness affects the parent’s mental health. NICUs tend to focus on this pair, in supporting family-centered care through breastfeeding and skin-to-skin contact. But during the pandemic, infection prevention has taken over. And it makes sense: Neonates are especially vulnerable to infections. [Read: Why a three-dose vaccine for kids might actually work out] Shuman has been studying families with babies in the NICU during the pandemic, and the biggest way that the NICU has changed, he says, is a shifting ground of visitation policies. Many parents describe updated visitation policies where they have to choose prescheduled slots in which to spend limited windows of time with their baby, so as not to overlap with other parents, DeOliveira, of Project NICU, said. In one study, conducted in 2020, 46 percent of NICU parents said that only one person was allowed to visit at a time, and Shuman says his data show 67 percent of the parents reported more than one change to a policy during their child’s stay in the hospital. That makes caring for a sick baby incredibly challenging. Visitation restrictions disrupted parents’ plans to breastfeed, which can be helpful to vulnerable infants, Shuman said. Shuman’s research found that the parents of NICU babies were experiencing unusual levels of distress, on top of their decreasing likelihood of breastfeeding. This situation led the National Association of Neonatal Nurses to publish position statements about the role of parents as essential caregivers to their infants—not just as future caretakers but as team members in the NICU. Policies that keep COVID-positive parents separated from their babies vary by hospital, and may have to do with factors outside doctors’ control. Some NICUs keep multiple patients in the same room; others have single-patient rooms, which allow more protection. When babies in the NICU do come down with COVID, it complicates their other medical issues—getting the coronavirus generally adds a week or two onto their hospital stay, McAdams says. And the long-term issues are still unknown for newborns: that is, whether COVID in infancy has any lingering impacts, such as brain fog, heart issues, problems with smell or taste. “A baby can’t tell you any of that stuff. There are a lot of question marks I think that will need to be studied,” he said. At the same time, some research shows that separation from parents can be connected to babies’ failure to thrive, and could affect cognitive development, Shuman pointed out. “The NICU is that unique time when that connection is broken,” he said. “If a mom is still recovering and the baby is removed, the restrictions during COVID lead to prolonged separation of mother and infant.” In other words, the separation itself could be its own risk. One strange silver lining that Shuman found in his research: Although having a baby during COVID increased the odds that a mother would be diagnosed with postpartum PTSD, having a baby in the NICU was sometimes protective against this type of stress, paradoxically. He thinks that’s because, in the NICU, parents had support. “We think that exposure to the nurses was somewhat protective, because they were able to provide support and consistency,” he told me. “Those who did not have a NICU baby, they didn’t have visitors, and they were overwhelmed.” That support can, in some ways, extend to a parent’s COVID diagnosis. McAdams was handling a preterm baby who wasn’t feeding well—the baby’s mother had been in the NICU for days when she tested positive for COVID. She called McAdams and told him she wanted to take the baby home. The baby wasn’t quite ready to go home, he told her; it needed a few more days in the hospital to really make sure that the feeding was going fine. McAdams also ordered a COVID test for the baby—and it came back positive. Fortunately, the baby was not symptomatic. McAdams called the mom back, and arranged for her to stay isolated in the NICU with the baby, so that they could be together and she could breastfeed. It ended up working out: The baby didn’t get ill, and was able to stay with the mother. But there were challenges, McAdams said: “If mom then gets sick in the hospital, we’re in the neonatal ICU. It’s not the adult ICU, so if mom gets sick, we really can’t take care of her—she’s not our patient.” Ultimately, their job is to do whatever is best for the baby. from https://ift.tt/BeyELR3 Check out http://natthash.tumblr.com And just like that, the national attitude on COVID is flipping like a light switch. As the United States descends the bumpy back end of the Omicron wave, governors and mayors up and down the coasts are extinguishing indoor mask mandates and pulling back proof-of-vaccination protocols. In many parts of the country, restaurants, bars, gyms, and movie theaters are operating at pre-pandemic capacity, not a face covering to be seen; even grade schools and universities have started to relax testing and isolation rules. These policy pivots mirror a turn in public resolve: Two years into the pandemic, many Americans are ready to declare the crisis chapter of COVID-19 over, and move on to the next. We can debate ad nauseam whether these rollbacks are premature. What’s far clearer is this: We’ve been at similar junctures before—at the end of the very first surge, again in the pre-Delta downslope. Each time, the virus has come roaring back. It is not done with us. Which means that we cannot be done with it. What’s up ahead is not COVID’s end, but the start of our control phase, in which we invest in measures to shrink the virus’s burden to a more manageable size. “This is the larger, longer game we’re having to think about,” Jennifer Nuzzo, an epidemiologist at the Johns Hopkins Bloomberg School of Public Health, told me. [Read: Endemicity is meaningless] To even think of controlling COVID for the long term means knocking up against some of the limits of our knowledge. Our future will depend both on the virus’s continued evolution, impossible to predict right now, and on our response, which will hinge on the strength of our resources and our willingness to deploy them. Every disease that troubles us prompts some sort of reaction; for this one, the nation is still deciding how much to invest. Control, then, can’t mean putting the virus behind us—quite the opposite. It means keeping tabs on it, even when it’s not terribly abundant; it means building and maintaining an arsenal of weapons to fight it; it means having the resources and sociopolitical will to react rapidly when the threat returns. Monitor, then intervene, then monitor, then intervene. Taking this challenge seriously—trying to properly contain a deadly, fast-moving, shape-shifting virus that has spent the past two years walloping us—could require a revamp of the standard American approach to quelling disease, on a scale the nation’s never managed before. We’ll have to write a brand-new public-health playbook, and figure out a way to execute it. Control is a simple word that, in the realm of infectious disease, doesn’t come with a sharp definition. It is possible, in some cases, to roughly anchor the concept to epidemiological goals—cutting cases of X disease by Y percentage by Z year, say; organizations such as the World Health Organization have set benchmarks like this for the control of measles, malaria, and tuberculosis. For COVID, too, we may eventually agree upon “milestones to measure where you’re at,” Wafaa El-Sadr, an epidemiologist at Columbia University, told me. But hard numbers are not necessary to define a control program, says David Heymann, an epidemiologist and global-health expert at the London School of Hygiene and Tropical Medicine. What unites diseases that are under control is human effort—a sustained commitment to restrain a pathogen, and hack away at its harms. Controlled diseases, then, might be better imagined as ones that “do not impact a lot of social functions, and do not drastically exacerbate inequities,” Saad Omer, an epidemiologist and global-health expert at Yale University, told me. Control manages a threat down into something that society can accept day after day after day—practically, less disease, less death, less suffering than might otherwise occur. It is “how we talk about diseases we’re doing something about,” says Ellie Murray, an epidemiologist at Boston University. [Read: How public health took part in its own downfall] With COVID, one of the only things we can be sure about is that control will be difficult. The coronavirus spreads stealthily and speedily, and can hop among many animal species; it shape-shifts frequently, such that our immune systems have trouble keeping track. All of this will make it tougher to suppress. But with the tools we have—among them vaccines, treatments, tests, masks, and air filtration—a less chaotic reality than the one we’re living now also remains within reach. Exactly what degree of control is possible will depend on the precise (and still-evolving) potency of those tools—the durability of shot-induced protection, for instance—and how broadly and equitably we can distribute them. Control’s timeline can also stretch extraordinarily long. After millennia of coexistence with the bacterium that causes tuberculosis, which kills some 1.5 million people a year, humanity is still trying to diminish its staggering global burden. We also know that COVID control won’t be static. At this point, we can expect disease to wax and wane. But bringing the virus to heel, and keeping it there, will require monitoring it even when it appears scarce. That starts with a commitment to surveillance—tracking where and in whom the virus is circulating, how quickly its levels are rising, and whether a new version poses an additional threat. The granular details that surveillance offers can help policy makers plan a response. Early blips of a variant that’s highly immune evasive, for instance, might demand a different response (consider updating the vaccines) than one that’s primarily pummeling the unvaccinated, elderly, and immunocompromised (boost the vulnerable, and shield them to squelch further spread). “The virus will dictate a lot of the terms,” Omer said. That doesn’t mean counting every case. But it does mean improving our capacity for testing, and being more systematic about whom and what in the population we’re surveying—and not just in the midst of a surge. Flu can offer us a starter package, at least technologically: The globe is freckled with surveillance sites designed to track where flu viruses are percolating, and what mutations they’re accumulating; in the U.S., an intricate network of hospitals, laboratories, and state and local health departments regularly shuttle samples and symptom data from flu patients to the CDC for analysis. To build capacity for COVID, we’ll need better ways to zero in on infections, Nuzzo, of Johns Hopkins, told me—ones that aren’t biased by who’s seeking out tests or who has access to medical care. “We need a representative sampling scheme to know what we’re looking at, as it’s happening,” she said. The more sensitive these systems are, the faster they’ll be able to signal that a viral comeback is nigh. Periods of relative calm, too, offer opportunities for institutions to prepare for the next difficult stretch. Medical infrastructure will need some suturing. Should COVID become a winter disease, it will slam us when many other pathogens do. “We need to make sure our health-care systems are able to meet demand,” Crystal Watson, a senior scholar at the Johns Hopkins Center for Health Security, told me. There’s no single or easy solution for this, but we could start with building more flexibility into the systems we use to treat the sick. Staffing shortages could be patched with a supplemental workforce, while hospitals offer retention packages; mental-health resources could ease burnout in overtaxed personnel. Trained teams of community health workers could help bridge gaps in communication, and deliver care to where it’s often been lacking, says Camara Jones, an epidemiologist and a health-equity researcher at UC San Francisco. At the same time, the federal government could funnel funds into developing and maintaining stocks of high-quality masks, tests, and over-the-counter antiviral pills, with a particular focus on ferrying tools to high-risk settings—long-term-care facilities, prisons, and the like—so that they could be speedily distributed “right when surges start,” Anne Sosin, a rural-health expert at Dartmouth University, told me. [Read: Hospitals can’t accept this as “normal”] Proper ventilation in public spaces, as my colleague Sarah Zhang has written, could also be key to COVID control. Done well, systematically decontaminating our air can exemplify public-health intervention at its best—one so constant, invisible, and ubiquitous that people can be protected without even knowing it, “the difference between everyone boils their own water versus we have clean water everywhere,” Whitney Robinson, an epidemiologist at the University of North Carolina at Chapel Hill, told me. But society-wide overhauls of infrastructure tend to be slow going. Schools, for instance, have been billed as an especially important target for these upgrades, but the pandemic funds that might drive such changes have plenty of other pressing uses too. And specific indoor-air-quality standards could push lawmakers to update building codes, but these, too, have been sluggish to arrive. Our country’s immunity will need shoring up as well. In the United States, too many people remain unvaccinated, among them 19 million kids under 5, who are still ineligible for their shots. Demand for boosters has been tepid, and people who are older or immunocompromised don’t always respond to their first dose. The situation abroad is even more dire; many nations still struggle to access the supply to deliver first doses, much less seconds or thirds. And the more susceptible hosts it finds, the more SARS-CoV-2 will split itself into new and dangerous forms. For Jones, the biggest near-term goal is to, as “expeditiously as possible, vaccinate the world,” she told me. Even after the foundations of protection are established, they will need updates, whether because our defenses against infection are dropping, because a surprise variant has arrived on the scene, or both. Going forward, vaccine mandates may have a heightened role to play, as certain businesses, schools, or entire jurisdictions try to buoy uptake, says Jason Schwartz, a vaccine-policy expert at Yale. The policy is controversial, but the United States already has centuries of precedent to guide it, and thanks to flu shots, has long harbored the infrastructure to roll vaccines out en masse, and at a regular clip. If that capacity is partnered with policies that help close equity gaps, population immunity could soar. Ensuring that everyone’s up to date on their shots, Schwartz told me, is how we generate a lasting “baseline of protection.” Not all COVID interventions can simply come on and stay on. Some tools operate at the individual level, and these are the control-phase wild cards. Their success depends not only on capacity and planning but on public acceptance. Protections won’t work if no one is willing to adopt them. If control is a moving target, then there’s little question that response must shift in lockstep with the threat. Several experts told me we could reasonably expect a future in which we abide by a tiered system of response, with the stringency of public-health measures titrated to how much virus is around. “The idea is that you can have gradations of every policy, rather than just taking everything on or off,” Abraar Karan, an infectious-disease physician and global-health expert at Stanford University, told me. Such a system might be roughly analogous to how we categorize and respond to hurricanes. Most of the time, life can proceed as usual, our tools on standby, our surveillance systems whirring. But as soon as danger begins to brew, protections may start to kick back into place. Even if we manage to reach a consensus on cues, there’s not a lot of obvious intuition about the second big question: which precautions should take priority. With COVID, the manual’s still being written, but it could go something like this: Say there’s a surge next winter. An initial upswing in cases might prompt your company holiday party to, once again, require employees to test to attend; your local grocery store to, once again, ask that you mask. Local leaders might set up mask- and test-distribution centers throughout the community so residents can grab and go. These early pivots put the focus on the tools that are, in theory, lower-effort investments that don’t impede much mingling and help keep most businesses afloat. The leading edge of a wave is also an essential time to buttress blanket protections: If older or immunocompromised individuals have skipped boosters, they might be nudged to catch up; if hospitals are running low on personnel, reinforcements might be rallied and deployed. “We don’t waste the lead time we’re given,” Omer said. Should all go well at this stage, the outbreak could quickly be quashed. [Read: The millions of people stuck in pandemic limbo] But if cases continue to climb, if ICUs begin to fill, if a new variant starts to sidestep the protection that vaccines or previous infections left behind, those are signals to go stricter. New vaccine mandates or booster requirements could kick in. Government or business owners could put in place capacity limits in restaurants and entertainment venues, flip to work-from-home policies, or amend travel protocols, to ensure that the outbreak doesn’t spiral out of control. As a last resort, policy makers could consider shutting entire swaths of society down—closing schools and other essential institutions, Celine Gounder, an epidemiologist and a senior fellow at Kaiser Health News, told me. “Things would have to really get bad for that,” she said: “basically, if we get to the point where hospitals are not able to function.” The trick is balancing public well-being with palatability. Which raises the third, and thorniest, issue: Who gets to make these decisions, and who bears the cost if plans go awry? “That’s what it ultimately comes down to: how much of what we’re doing is mandatory versus motivated by personal risk-based decisions,” Nuzzo told me. Certainly, if deaths are skyrocketing, if health-care systems are near the point of collapse, governments will need to step in. Where experts start to diverge, though, is on questions of who’s in charge at every other stage—whether governments or individual members of the public should conduct the brunt of risk assessment and management. Mandates are the business of leadership. Their strength is that they “reach more people,” Julia Raifman, a health-policy expert at Boston University, told me. “And they reach them more equitably.” A coordinated response, helmed by leaders with money and a platform, can present a unified front against an incoming threat, and offer people clear-cut guidelines to follow. Denmark, which recently announced that it was lifting nearly all of its COVID restrictions, has embarked on a rather extreme version of this tactic, its government repeatedly removing and reimposing restrictions as circumstances shift. At its best, such a strategy can be especially well aligned with an infectious threat: Collective danger merits collective response. [Read: How Denmark decided COVID isn’t a critical threat to society] But totally extracting personal choices from the equation of disease prevention is impossible. Adherence to mandates and long-term investments in protective behaviors are “tied to the levels of trust” we have in one another and in the people who lead us, Tom Bollyky, the director of the global-health program at the Council on Foreign Relations, told me. He and his colleagues have found that in outbreaks past and present, trust in government seems to buoy vaccination rates and the adoption of infection-prevention behaviors—such as hand-washing and physical distancing—thus curbing contagion. In the U.S., with its streak of individualism and eroded confidence in the government, the chances of following the Danish model appear essentially shot. Plus, policies that are constantly switching from on to off run the risk of losing public interest each time they flicker. In the United States, decisions about mandates have also been left up to states, even to local jurisdictions, seeding a patchwork of policies. Many Americans have had to wearily navigate the chaos of living in a masks required neighborhood and working in a masks not required one. For these reasons and more, several other experts are wary of a mandate-forward approach. Nuzzo’s among them. “We have to be sparing with what we’re asking people to do,” Nuzzo said, both to keep people invested and to preserve their stamina for the next infectious crisis. Schwartz, of Yale, feels similarly. Most mandates are a lever to be pulled “in case of emergency” and, generally speaking, are far too great a sledgehammer to wield at other times. When it comes to daily-use interventions, such as masks, Watson, of Johns Hopkins, thinks that Americans might feel better if they’re told it’s okay to strike out on their own; such an idea could even be actively empowering, if people feel that they’re able to make informed choices in times of crisis. Heymann, of the London School of Hygiene and Tropical Medicine, says a version of this has been in place in the United Kingdom for months. “The government shifted risk assessment and risk management to the individual,” he told me. Masks, tests, and vaccines are widely available to residents; people are advised to cover their faces in certain crowded settings, but there’s no outright requirement. Should Americans follow suit, Watson imagines they might benefit from a tool to help guide personal, day-to-day choices—something like “a weather forecast for infectious disease,” which might take the form of a computer- or smartphone-accessible feed of data on local viral conditions. The precursors for a system like that are already taking root at the CDC, and with information in hand, she thinks that “people will take their own actions to protect themselves.” In the same way that weather apps issue winter-storm advisories, or flag high local pollen counts, governments could flag that a ton of virus is in the vicinity, and recommend precautions. Still, Watson and Schwartz admit that a system like this has no precedent—it would be a “large-scale reimagining of how we think about prevention,” Schwartz said. Americans have never had to be so keenly aware of how much of a respiratory virus is bopping around. And not everyone will be eager or able to opt-in. Many will simply lack the time or resources to check such a forecast, much less act on the intel, especially if access to masks, air filtration, and tests remains “a premium” in this country, Deshira Wallace, a health-equity researcher at UNC Chapel Hill, told me. And while the weather provides its own feedback—precipitation is visible and audible; temperature can be felt—viruses elude our senses, so their perils are harder to gauge. They’re much more insidious. One person’s ignoring a rainy forecast risks only that they get wet, but an individual’s negligence in responding to infectious disease can sicken both them and someone else. This is the problem with wrangling viruses: They do not obey the boundaries of bodies, or of cities or states. When they spill between people and communities, they ratchet up everyone’s risk. In the face of collective risk, the better bet will be at least to choose some policy, with the understanding that we’ll have to tweak and finagle it, rather than select door No. 3—total inaction, an opportunity for the virus to run roughshod over us because we simply let it. Disease control, when it’s done right, is as much a social undertaking as it is a scientific one. Weak social infrastructures can derail containment and push goals out of reach. But just as neglect can augment burdens, investment can diminish them. “Public health travels at the speed of trust,” Dartmouth’s Sosin told me. Even when state or federal governments falter, trust can still be forged. Springfield, Missouri, vanished its masking requirements in May 2021, and “I don’t think we’ll ever go back,” Cora Scott, the city’s director of public information and civic engagement, told me. But she said she and her team feel that they’re still making inroads on mitigation by recruiting local messengers. For months, they’ve been pouring resources into getting the city’s still-low vaccination rates up—an initiative that’s included sending public-health personnel door-to-door. Leveraging the strength of communities will be an essential strategy in the months and years to come. For a long time now, American confidence in government has been troublingly low. But people still place immense trust in their own health-care providers, for instance—the individuals who feel close to home. And the tactic has played a role in halting outbreaks before. Bollyky points out that partnerships between local and national leaders, bulwarked by community liaisons, helped turn the tide during the 2014 outbreak of Ebola in Guinea, Liberia, and Sierra Leone. Key to all of this is “paying attention to the specific needs of individual communities,” Andrea Milne, a medical historian at Case Western Reserve University, told me, and tailoring policies to suit them. What works to stamp out misinformation in Guinea won’t necessarily be what gets shots into arms in Springfield. Locals will understand those differences best, and know how to navigate through them. [Read: The seven habits of COVID-resilient nations] HIV, too, offers an example of a virus that can be well managed via a community-centered approach, El-Sadr, of Columbia, said. In the past four decades, infections have become more bearable through the development of powerful and readily available antivirals and tests that can be taken at home, through routine surveillance for infections, and through public investment, education, and partnerships with the communities most severely affected by disease. Milne points to the San Francisco Model of AIDS care, which has centered a “multisystem, holistic approach” in beating the city’s epidemic back. Even in its early days, the program focused not just on clinical care but on “getting food to people, and making sure people could afford bus rides to the doctor,” she said. “Community members were doing the educating. People were treated not just as patients, but as agents in this health-care work.” In the years since the model’s debut, new HIV diagnoses in San Francisco have plummeted. SARS-CoV-2 is an entirely different pathogen, but our current response to it risks rehashing some of the failures of the early HIV response, shifting the burden of suffering to the vulnerable. The task of taming this new threat, El-Sadr told me, can and should bear hallmarks to the successful strategies we’ve leaned on before. There’s even opportunity to riff and expand on the templates that past pandemics have offered: to introduce paid sick leave and food assistance; to speed the development of safer housing options; to meet the needs of people who are chronically ill, immunocompromised, and disabled; to address the inequities that have concentrated suffering in marginalized populations, both domestically and abroad. Pandemics are an opportunity to respond in the present but also prepare for the future. And if SARS-CoV-2 sparks its own revolution, that won’t be the first time a virus has catalyzed lasting change. “When there’s no trust, it’s often because people feel they haven’t been listened to,” El-Sadr said. “In the HIV world, we always say, ‘Nothing about us without us’”—no decisions should be made about the fate of a particular group of people without their involvement. “I think that’s at the core of it.” It’s true that some of the best public-health interventions are ones we don’t notice. But others succeed precisely because they enlist people’s attention and use it. from https://ift.tt/V4Okuse Check out http://natthash.tumblr.com It’s suddenly become acceptable to say that COVID is—or will soon be—like the flu. Such analogies have long been the preserve of pandemic minimizers, but lately they’ve been creeping into more enlightened circles. Last month the dean of a medical school wrote an open letter to his students suggesting that for a vaccinated person, the risk of death from COVID-19 is “in the same realm, or even lower, as the average American’s risk from flu.” A few days later, David Leonhardt said as much to his millions of readers in the The New York Times’ morning newsletter. And three prominent public-health experts have called for the government to recognize a “new normal” in which the SARS-CoV-2 coronavirus “is but one of several circulating respiratory viruses that include influenza, respiratory syncytial virus (RSV), and more.” The end state of this pandemic may indeed be one where COVID comes to look something like the flu. Both diseases, after all, are caused by a dangerous respiratory virus that ebbs and flows in seasonal cycles. But I’d propose a different metaphor to help us think about our tenuous moment: The “new normal” will arrive when we acknowledge that COVID’s risks have become more in line with those of smoking cigarettes—and that many COVID deaths, like many smoking-related deaths, could be prevented with a single intervention. [Read: Endemicity is meaningless] The pandemic’s greatest source of danger has transformed from a pathogen into a behavior. Choosing not to get vaccinated against COVID is, right now, a modifiable health risk on par with smoking, which kills more than 400,000 people each year in the United States. Andrew Noymer, a public-health professor at UC Irvine, told me that if COVID continues to account for a few hundred thousand American deaths every year—“a realistic worst-case scenario,” he calls it—that would wipe out all of the life-expectancy gains we’ve accrued from the past two decades’ worth of smoking-prevention efforts. The COVID vaccines are, without exaggeration, among the safest and most effective therapies in all of modern medicine. An unvaccinated adult is an astonishing 68 times more likely to die from COVID than a boosted one. Yet widespread vaccine hesitancy in the United States has caused more than 163,000 preventable deaths and counting. Because too few people are vaccinated, COVID surges still overwhelm hospitals—interfering with routine medical services and leading to thousands of lives lost from other conditions. If everyone who is eligible were triply vaccinated, our health-care system would be functioning normally again. (We do have other methods of protection—antiviral pills and monoclonal antibodies—but these remain in short supply and often fail to make their way to the highest-risk patients.) Countries such as Denmark and Sweden have already declared themselves broken up with COVID. They are confidently doing so not because the virus is no longer circulating or because they’ve achieved mythical herd immunity from natural infection; they’ve simply inoculated enough people. President Joe Biden said in January that “this continues to be a pandemic of the unvaccinated,” and vaccine holdouts are indeed prolonging our crisis. The data suggest that most of the unvaccinated hold that status voluntarily at this point. Last month, only 1 percent of adults told the Kaiser Family Foundation that they wanted to get vaccinated soon, and just 4 percent suggested that they were taking a “wait-and-see” approach. Seventeen percent of respondents, however, said they definitely don’t want to get vaccinated or would do so only if required (and 41 percent of vaccinated adults say the same thing about boosters). Among the vaccine-hesitant, a mere 2 percent say it would be hard for them to access the shots if they wanted them. We can acknowledge that some people have faced structural barriers to getting immunized while also listening to the many others who have simply told us how they feel, sometimes from the very beginning. The same arguments apply to tobacco: Smokers are 15 to 30 times more likely to develop lung cancer. Quitting the habit is akin to receiving a staggeringly powerful medicine, one that wipes out most of this excess risk. Yet smokers, like those who now refuse vaccines, often continue their dangerous lifestyle in the face of aggressive attempts to persuade them otherwise. Even in absolute numbers, America’s unvaccinated and current-smoker populations seem to match up rather well: Right now, the CDC pegs them at 13 percent and 14 percent of all U.S. adults, respectively, and both groups are likely to be poorer and less educated. [Read: It’s a terrible idea to deny medical care to unvaccinated people] In either context, public-health campaigns must reckon with the very difficult task of changing people’s behavior. Anti-smoking efforts, for example, have tried to incentivize good health choices and disincentivize bad ones, whether through cash payments to people who quit, gruesome visual warnings on cigarette packs, taxes, smoke-free zones, or employer smoking bans. Over the past 50 years, this crusade has very slowly but consistently driven change: Nearly half of Americans used to smoke; now only about one in seven does. Hundreds of thousands of lung-cancer deaths have been averted in the process. With COVID, too, we’ve haphazardly pursued behavioral nudges to turn the hesitant into the inoculated. Governments and businesses have given lotteries and free beers a chance. Some corporations, universities, health-care systems, and local jurisdictions implemented mandates. But many good ideas have turned out to be of little benefit: A randomized trial in nursing homes published in January, for example, found that an intensive information-and-persuasion campaign from community leaders had failed to budge vaccination rates among the predominantly disadvantaged and low-income staff. Despite the altruistic efforts of public-health professionals and physicians, it’s becoming harder by the day to reach immunological holdouts. Booster uptake is also lagging far behind. This is where the “new normal” of COVID might come to resemble our decades-long battle with tobacco. We should neither expect that every stubbornly unvaccinated person will get jabbed before next winter nor despair that none of them will ever change their mind. Let’s accept instead that we may make headway slowly, and with considerable effort. This plausible outcome has important, if uncomfortable, policy implications. With a vaccination timeline that stretches over years, our patience for restrictions, especially on the already vaccinated, will be very limited. But there is middle ground. We haven’t banned tobacco outright—in fact, most states protect smokers from job discrimination—but we have embarked on a permanent, society-wide campaign of disincentivizing its use. Long-term actions for COVID might include charging the unvaccinated a premium on their health insurance, just as we do for smokers, or distributing frightening health warnings about the perils of remaining uninoculated. And once the political furor dies down, COVID shots will probably be added to the lists of required vaccinations for many more schools and workplaces. To compare vaccine resistance and smoking seems to overlook an obvious and important difference: COVID is an infectious disease and tobacco use isn’t. (Tobacco is also addictive in a physiological sense, while vaccine resistance isn’t.) Many pandemic restrictions are based on the idea that any individual’s behavior may pose a direct health risk to everyone else. People who get vaccinated don’t just protect themselves from COVID; they reduce their risk of passing on the disease to those around them, at least for some limited period of time. Even during the Omicron wave, that protective effect has appeared significant: A person who has received a booster is 67 percent less likely to test positive for the virus than an unvaccinated person. But the harms of tobacco can also be passed along from smokers to their peers. Secondhand-smoke inhalation causes more than 41,000 deaths annually in the U.S. (a higher mortality rate than some flu seasons’). Yet despite smoking’s well-known risks, many states don’t completely ban the practice in public venues; secondhand-smoke exposure in private homes and cars—affecting 25 percent of U.S. middle- and high-school children—remains largely unregulated. The general acceptance of these bleak outcomes, for smokers and nonsmokers alike, may hint at another aspect of where we’re headed with COVID. Tobacco is lethal enough that we are willing to restrict smokers’ personal freedoms—but only to a degree. As deadly as COVID is, some people won’t get vaccinated, no matter what, and both the vaccinated and unvaccinated will spread disease to others. A large number of excess deaths could end up being tolerated or even explicitly permitted. Noel Brewer, a public-health professor at the University of North Carolina, told me that anti-COVID actions, much like anti-smoking policies, will be limited not by their effectiveness but by the degree to which they are politically palatable. Without greater vaccination, living with COVID could mean enduring a yearly death toll that is an order of magnitude higher than the one from flu. And yet this, too, might come to feel like its own sort of ending. Endemic tobacco causes hundreds of thousands of casualties, year after year after year, while fierce public-health efforts to reduce its toll continue in the background. Yet tobacco doesn’t really feel like a catastrophe for the average person. Noymer, of UC Irvine, said that the effects of endemic COVID, even in the context of persistent gaps in vaccination, would hardly be noticeable. Losing a year or two from average life expectancy only bumps us back to where we were in … 2000. Chronic problems eventually yield to acclimation, rendering them relatively imperceptible. We still care for smokers when they get sick, of course, and we reduce harm whenever possible. The health-care system makes $225 billion every year for doing so—paid out of all of our tax dollars and insurance premiums. I have no doubt that the system will adapt in this way, too, if the coronavirus continues to devastate the unvaccinated. Hospitals have a well-honed talent for transforming any terrible situation into a marketable “center of excellence.” COVID is likely to remain a leading killer for a while, and some academics have suggested that pandemics end only when the public stops caring. But we shouldn’t forget the most important reason that the coronavirus isn’t like the flu: We’ve never had vaccines this effective in the midst of prior influenza outbreaks, which means we didn’t have a simple, clear approach to saving quite so many lives. Compassionate conversations, community outreach, insurance surcharges, even mandates—I’ll take them all. Now is not the time to quit. from https://ift.tt/OiC9nlX Check out http://natthash.tumblr.com When the coronavirus pandemic began, Emily Landon thought about her own risk only in rare quiet moments. An infectious-disease doctor at the University of Chicago Medicine, she was cramming months of work into days, preparing her institution for the virus’s arrival in the United States. But Landon had also recently developed rheumatoid arthritis—a disease in which a person’s immune system attacks their own joints—and was taking two drugs that, by suppressing said immune system, made her more vulnerable to pathogens. Normally, she’d be confident about avoiding infections, even in a hospital setting. This felt different. “We didn’t have enough tests, it was probably around us everywhere, and I’m walking around every day with insufficient antibodies and hamstrung T-cells,” she told me. And she knew exactly what was happening to people who got infected. One night, she found that in the fog of an earlier day, she had written on her to-do list: Make a will. “And I realized, Oh my God, I could die,” she said. “I just cried and cried.” Two years later, COVID-19 is still all around us, everywhere, and millions of people like Landon are walking around with a compromised immune system. A significant proportion of them don’t respond to COVID vaccines, so despite being vaccinated, many are still unsure whether they’re actually protected--and some know that they aren’t. Much of the United States dropped COVID restrictions long ago; many more cities and states are now following. That means policies that protected Landon and other immunocompromised people, including mask mandates and vaccination requirements, are disappearing, while accommodations that benefited them, such as flexible working options, are being rolled back. This isn’t a small group. Close to 3 percent of U.S. adults take immunosuppressive drugs, either to treat cancers or autoimmune disorders or to stop their body from rejecting transplanted organs or stem cells. That makes at least 7 million immunocompromised people—a number that’s already larger than the populations of 36 states, without even including the millions more who have diseases that also hamper immunity, such as AIDS and at least 450 genetic disorders. In the past, immunocompromised people lived with their higher risk of infection, but COVID represents a new threat that, for many, has further jeopardized their ability to be part of the world. From the very start of the pandemic, some commentators have floated the idea “that we can protect the vulnerable and everyone else can go on with their lives,” Seth Trueger, who is on immunosuppressants for an autoimmune complication of cancer, told me. “How’s that supposed to work?” He is an emergency doctor at Northwestern Medicine; he can neither work from home nor protect himself by avoiding public spaces. “How am I supposed to provide for my family or live my life if there’s a pandemic raging?” he said. Contrary to popular misconceptions, most immunocompromised people are neither visibly sick nor secluded. “I know very few people who are immunocompromised and get to live in a bubble,” says Maggie Levantovskaya, a writer and literature professor who has lupus, an autoimmune disorder that can cause debilitating inflammation across the entire body. As the coronavirus moves from a furious boil to a gentle simmer, many immunocompromised people (like everyone else) hope to slowly expand their life again. But right now, “it’s like asking someone who cannot swim to jump into the ocean instead of trying a pool,” Vivian Cheung, a biologist at the University of Michigan who has a genetic autoimmune disorder, told me. “I feel this pressure of jumping into the Pacific and not knowing if I can survive or not.” Whether that changes depends on the accommodations society is willing to make. Ramps, accessibility buttons, screen readers, and many other measures have made life easier for disabled people, and a new wave of similar accommodations is now necessary to make immunosuppression less of a disability in the COVID era. Exactly none of the people I talked with wants a permanent lockdown. “It’s not like immunocompromised people are enjoying any of this,” Levantovskaya told me. What they do want—work flexibility, better ways of controlling infectious diseases, and more equitable medical treatments—would also benefit everyone, not just now but for the rest of our lives. For more than three decades, Julia Irzyk has lived with lupus symptoms. She also has rheumatoid arthritis, a degenerative spinal condition, and heart problems. When she gets colds, they tend to progress to full-blown pneumonia, so even before the pandemic she was mindful about infections. She’d avoid big events and rarely ate out. When she flew, which she did infrequently, she’d wear a mask. For this story, I spoke with 21 people who are either immunocompromised or care for those who are; others were similarly fastidious pre-pandemic about washing their hands, getting their flu vaccines, and avoiding people who were clearly sick. Landon wouldn’t go to parties at the height of flu season. Cheung wore masks on flights and wiped down the surfaces around her. But none of them was living in seclusion. All of them had rich social lives. COVID changed that. The new coronavirus forced them to go beyond their previous precautions, because it is deadlier than normal respiratory pathogens, can spread from people who aren’t obviously sick, and did so at breakneck speed. Compared with others, when immunocompromised people get COVID-19, they tend to be sicker for longer. Irzyk’s rheumatologist told her not to go out: If you get this, your heart and lungs won’t be able to take it. So she went seven months without leaving her home, and still spends most of her time there. She missed both her grandmothers’ funerals. She delayed important medical procedures, even as her lupus symptoms got worse because one of her treatments—hydroxychloroquine—ran out of stock after Donald Trump falsely touted it as a COVID cure. COVID has also defined Harper Corrigan’s life. She was born in September 2019—nine weeks early, and with a rare brain malformation called lissencephaly. She has never played with another child even though, being sassy and funny, she really wants to. A week before the U.S. shut down in March 2020, Harper had to have a tracheostomy, leaving her even more vulnerable to respiratory viruses and, in turn, potentially deadly seizures. The Corrigans spent 11 months with her in the hospital. Even after her health had stabilized, they couldn’t find any nurses to help with home care, and the hospital wouldn’t discharge her. When they finally got home, they went into strict lockdown. Children with Harper’s condition aren’t expected to live to adulthood, so her mother, Corey, told me that her priority is to “squeeze a full life into an unknown amount of time.” But that requires the spread of the virus to slow, and vaccines to be authorized for children under 5. The danger of the pandemic’s first fearful year still hangs over the heads of many immunocompromised people, even as those around them relax into the security of vaccination. Vaccines should substantially slash the risk of infection and severe illness, but many immunocompromised people barely respond to the COVID shots. At one extreme, about half of organ-transplant recipients produce no antibodies at all after two vaccine doses. Compared with the general vaccinated public, they are 82 times more likely to get breakthrough infections and 485 times more likely to be severely ill. Should they get infected, their risk of hospitalization is a coin flip. Their risk of death is one in 10. “Imagine walking around and being in society and thinking, If you give me COVID, I might have a 10 percent risk of dying,” Dorry Segev, a transplant surgeon at the Johns Hopkins University School of Medicine, told me. His patients are better off than unvaccinated people, “but not by much, despite all we’ve done.” Other groups of immunocompromised people fare better after vaccination, but Segev estimates that a quarter are still insufficiently protected. And some people with autoimmune disorders cannot be fully vaccinated, because their initial doses led to severe flare-ups of their normal symptoms. Alfred Kim, a rheumatologist at Washington University in St. Louis who specializes in lupus, told me that 5 to 10 percent of his patients experienced these problems; so did two of the people I interviewed, both of whom declined further shots. Many immunocompromised people are now stuck in limbo—unsure about how safe they really are, even after getting three shots and a booster, as the CDC advises. Scientific studies can hint at the average risks across large groups but offer little certainty for individuals. Sometimes, no studies exist at all, as is the case for Cheung, whose genetic disorder is so rare that it doesn’t even have a name. “As a doctor, I’m trained to parse scientific data, but I can’t parse my way to answers that don’t exist,” says Lindsay Ryan, a physician at UC San Francisco who has a neurological autoimmune disorder. “Could I actually define my risk of death if I got COVID? No, I really can’t. And that’s a hard thing to make peace with.” Each individual infection is its own high-stakes gamble. I’ve spoken with immunocompromised people who got COVID and were fine. Others had mild initial illness, but then developed more severe long-COVID symptoms. Yet others are certain they’d fare badly: Chloe Atkins, a political scientist who works on disability and employment issues, has an autoimmune disease called myasthenia gravis, and “colds can immediately make it difficult for me to breathe, see, move, walk, or talk,” she told me. She knew two people with the same condition, both of whom died from COVID. She and others are facing the same arduous risk assessments that everyone else contends with—but heightened because of the greater possible costs of choosing wrongly. And while they wrestle with those uncertainties, the gulf between them and the rest of society is widening. Over the past year, as many Americans reveled in their restored freedoms, many immunocompromised people felt theirs shrinking. When the CDC announced that fully vaccinated Americans no longer needed to mask indoors, simple activities such as grocery shopping became more dangerous for immunocompromised people, who were offered no advice from the nation’s top public-health agency. When Joe Biden said in a speech that unvaccinated Americans were “looking at a winter of severe illness and death,” “I felt like he was talking to me,” Cheung said. And when commentators bemoaned irrational liberals who refused to abandon pandemic restrictions, many of the people I spoke with felt they were being mocked for trying to protect themselves and their loved ones. “I already feel different from other people because of this situation,” Colleen Boyce told me; she donated a kidney to her husband, Mark, who is now immunosuppressed. “The thought that when I mask up, others might look at me like there’s something wrong with me is hard to handle.” These changes were especially hard to take because, for a time, immunocompromised people caught a glimpse of something better. Beth Wallace, a rheumatologist at the University of Michigan, told me that many of her patients once accepted that viruses would regularly flatten them but have now realized that they don’t have to live that way. Cautious behaviors and flexibility around work meant that the flu practically vanished, and many immunocompromised people were actually less sick during the COVID era than before. And while they don’t want lockdowns to persist, they had hoped that the flexibility might. Sung Yun Pai of the National Institutes of Health told me that in the past, her patients—children who receive stem-cell transplants to treat genetic immune disorders—would simply have had to miss school. “In some ways, the whole world going virtual gave them better access to education,” she said. But remote options are now disappearing, and not just in schooling. Several immunocompromised people told me that their social world is shrinking, as friends who earlier in the pandemic hung out with them virtually are now interested only in face-to-face gatherings. Work is becoming less flexible too. Finding and keeping jobs can be very hard for people with chronic illnesses such as lupus, which can leave them feeling powerless to advocate for themselves. With “close to no say about your working conditions, you can only do so much to protect yourself,” Levantovskaya, the literature professor, said. Several immunocompromised people have been told that they’re holding the rest of society back. In fact, it is the opposite: They’re being forced to reintegrate with no regard for their residual risk. And perhaps worst of all, immunocompromised people began to be outright dismissed by their friends, relatives, and colleagues because of the misleading narrative that Omicron is mild. The variant bypassed some of the defenses that even immunocompetent people had built up, rendered several antibody treatments ineffective, and swamped the health-care system that immunocompromised people rely on. And yet one of Wallace’s patients was told by their sister that no one is dying anymore. In fact, people are still dying, and immunocompromised people disproportionately so. Ignoring that sends an implicit message: Your lives don’t matter. Sometimes, the message becomes explicit. Several of the immunocompromised people I talked with have been told—sometimes by family members or former partners—that they are a burden on society, that they don’t deserve a relationship, that their dying would be natural selection. When Corey Corrigan was trying to decide whether to put Harper through another surgery, “a medical provider said, ‘Well, she’s not going to live very long, so it doesn’t really matter,’” she told me. When Atkins, the political scientist, first heard that the other coronaviruses that cause common colds may have started as worse pathogens, she immediately thought about what that trajectory means for COVID. “Oh, people like me die off and the ones for whom it’s not a big impact carry on, and COVID becomes a cold,” she told me. “Part of me still feels that way, like there’s a sort of natural eugenics happening.” Eugenics—the concept of improving humanity by encouraging the “fittest” people to have children while preventing the “unfit” from doing so—is most commonly associated with the Holocaust, Aparna Nair, an anthropologist and historian of disability at the University of Oklahoma, told me. But in the 20th century, the concept had broad support from physicians and public-health practitioners, who saw it as a scientific way of solving problems such as poverty and poor health; it influenced the development of IQ tests, marriage counseling, and immigration laws. Eugenics is “often framed as part of a past that is over,” Nair said. “I think the pandemic has demonstrated that that’s not entirely the case.” Most Americans today would probably think the concept reprehensible and few are actively pursuing it. But when a society acts as if the deaths of vulnerable people are unavoidable, and does little to lessen their risks, it is still implicitly assigning lower value to certain lives. COVID isn’t going away. With eradication long off the table, the disease will become a permanent part of our lives—another serious infectious threat added to a ledger already full of them. “Everyone who’s immunocompromised will have to figure out what their normal looks like—and it isn’t going to look like the normal for other people,” Ryan, of UC San Francisco, told me. New treatments could help. Paxlovid, an antiviral drug from Pfizer, can reduce the risk of hospitalization and death from COVID by 88 percent, as long as patients are treated within five days of their first symptoms (although the NIH notes that the drug shouldn’t be given alongside certain immunosuppressants). Evusheld, a two-antibody cocktail from AstraZeneca, can reduce the risk of developing COVID, and though less effective against Omicron, it is still protective; the FDA issued an emergency-use authorization for the cocktail to prevent infections in immunocompromised people. But these drugs are in short supply. The government has ordered only 1.7 million doses of Evusheld and distributed 400,000, which is woefully inadequate given that the U.S. has at least 7 million immunocompromised adults. Many institutions have only enough for their most severely immunosuppressed patients, “and there’s people like me who don’t even come close to meeting the cut,” UChicago Medicine’s Landon told me. Even patients who clear the high bar of medical need might not be able to get a dose quickly; some hospitals have had to run lotteries to decide who gets the drugs. “It’s truly not acceptable,” said Cheung, who got Evusheld only by pestering every medical contact she had—a route not available to people without connections, time, or privilege. For her and others, this problem compounds their sense that their government deems them dispensable, especially considering the far-greater effort put into producing and distributing vaccines. “There’s a drug that could prevent immunocompromised people who aren’t protected from vaccines from dying,” Ryan said. “Shouldn’t they have access to it before we decide that COVID belongs in the same category as the flu?” Beyond equitable access to treatments, the people I spoke with mostly want structural changes—better ventilation standards, widespread availability of tests, paid sick leave, and measures to improve vaccination rates. Above all else, they want flexibility, in both private and public spaces. That means remote-work and remote-school options, but also mask mandates for essential spaces such as grocery stores and pharmacies, which could be toggled on or off depending on a community’s caseload. Without better, more available treatments or more structural changes, immunocompromised people will still depend on measures that prevent infections. Maintaining them would require, at times, that others make some allowance for their heightened risk. But in terms of what individual people can do for them, the most common request I heard was: Just have a heart. Regardless of your own choices, don’t jeer at us for being mindful of our higher risks, and definitely don’t tell us that our lives are worth less. All of these measures would protect society as a whole from infectious diseases in general. They would also require some upfront investment in deciding how, exactly, they would work—should companies be required to offer remote work, when possible, for some duration? What’s the threshold for switching on mask requirements? These policies represent added expense and effort for our institutions, but this is the question that the U.S. now faces: COVID has added burdens to our society; who will bear their weight? Immunocompromised people often hear that the world didn’t make accommodations for them before the pandemic and shouldn’t be expected to do so after. But in the past, infectious diseases did prompt big social changes. A massive infrastructure was created to meet the yearly onslaught of influenza, including antivirals, annual vaccines, and a global surveillance system that tracks new strains. After the polio epidemics of the 1940s, “there was a wave of interest in remote schooling and an increasing number of people who used phones and other technologies to finish school and go to university,” Nair, the historian of disability, told me. And in the late 20th century, the notion of disability itself began to shift. It used to be seen as an entirely medical problem—something that emerges from a person’s biology and can be fixed, Nair said. But the disability-rights movement ushered in a more social model, in which disability is as much about a person’s environment as it is about their body. People who use wheelchairs are less disabled in spaces with ramps and accessibility buttons on doors. Similarly, equitable access to Evusheld and flexible working policies would make immunocompromised people less disabled in an era where COVID is here to stay. COVID will eventually become endemic—a term “with so many definitions that it means almost nothing at all,” as my colleagues Katherine J. Wu and Jacob Stern wrote. “The error I hear so often now is to use the notion of an endemic virus as a reason for abdication—to drop precautions quickly and not do the more important and difficult work of putting in place the societal measures that would make living with coronavirus more tolerable,” Ryan said. “We need to earn the ability to switch from emergency to endemic.” Fashioning a world in which being immunocompromised requires fewer compromises is possible and is not too onerous. And even if people reject the moral argument for creating such a world, there are two good, selfish reasons to build it nonetheless. First, the coronavirus evolves rapidly in people with weakened immune systems, who also suffer longer infections and are contagious for more time. The Alpha variant of the first pandemic winter likely evolved in this way, and Omicron may have too. “It’s quite possible that a new variant that harms someone with a normal immune system could come from an immunocompromised person who they failed to protect,” Kim, the Washington University rheumatologist, told me. Second, the immune system weakens with age, so while most people will never be as vulnerable as an organ-transplant recipient, their immunity will still become partly compromised. Respecting the needs of immunocompromised people isn’t about disproportionately accommodating some tiny minority; it’s really about empathizing with your future self. “Everyone’s going to deal with illness at some point in their life,” Levantovskaya said. “Don’t you want a better world for yourself when that time comes?” from https://ift.tt/FegUsRb Check out http://natthash.tumblr.com Of all the pandemic waves the United States has weathered so far, this one feels uniquely baffling. Omicron is on its way out, and states are relaxing their mask mandates, but close to 200,000 people are still testing positive each day. The country is more vaccinated than ever before, but not vaccinated enough to stop hospitals from filling up with COVID patients. And while we’re still dealing with this variant, another one capable of breaking through those defenses could still emerge. With the coronavirus continuing to surprise us at every turn, the only thing that is certain now is uncertainty. At this point, many Americans are no longer letting the pandemic interfere with their lives. Some never bothered with safety measures; some are finally just beginning to loosen up as case numbers fall. Meanwhile, for other people—especially the immunocompromised and parents of young, unvaccinated children—post-Omicron life is downright maddening: It’s still tough to figure out how safe being indoors with others is, whether to let kids go maskless at school, or if whatever variant comes next will thwart your travel plans. As this crisis drags into its third year, the anxiety of not knowing what’s ahead of us is sparking even more pandemic fatigue, Catherine Bagwell, a psychologist at Emory University, told me. “We are starting to see that [uncertainty] spill over and affect mental health,” she said. Unfortunately, there’s no secret hack to make the pandemic less uncertain right now. But learning to live with ambiguity can go a long way in helping get us to the end of this crisis. “We can’t really predict well what’s going to happen, but accepting that we can’t predict the future is something that’s fairly freeing,” Tara Kirk Sell, a risk-communication researcher at Johns Hopkins, told me. All the advice that experts shared with me converged on a single idea: The best way to prepare for an uncertain future is to stay as flexible as you can. Of course, doing so is easier said than done. The rigidity in certain pandemic routines, such as insisting on eating outdoors, can make it harder and more stressful to adapt when the situation changes. And these days, the situation is always changing. In the most basic sense, a more flexible mindset is necessary because it is aligned with scientists’ evolving understanding of COVID. The constant changes in public-health messaging during the pandemic have been bewildering and poorly handled, and this highly erratic and still poorly understood virus does not do us any favors. When COVID numbers begin to improve, as they are doing right now, flexibility empowers us to take advantage of the situation. As The Atlantic’s Katie Wu recently wrote, “This stretch may be defined less by what we can’t do, and more by what we safely, carefully, finally can.” Likewise, flexibility gives us space to pivot if things worsen. Sell, for example, lets her son play in an indoor soccer league, but she has taken him out of games when she’s noticed that other players are clearly sick. “Have the flexibility to say, ‘I don’t have to have the same standards all the time,’” she said. “It’s not a bad thing to say ‘New information will change my outlook.’” Hearing this may come as a relief to anyone who has felt sheepish about constantly changing their personal safety standards, as if the inconsistency reveals some character defect, such as being indecisive or a worrywart. I feel particularly silly every time I explain to my (less anxious) friends why I felt comfortable going to an event one day but not the next. Especially right now, when Americans’ pandemic behavior varies so widely, staying flexible can be easier if you communicate your personal standards to your friends, and find ways to spend time together that allow everyone to feel comfortable. A good friend probably won’t hold it against you. Moreover, giving yourself a break is important, Karin Coifman, an associate professor of psychology at Kent State University, told me. Part of what makes post-Omicron life so stressful is that knowing what precautions to take is so hard. Especially if you’re fully vaccinated, you don’t have to feel guilty or ashamed about relaxing some of your personal rules. “It may be that this week you’re feeling that you’re not ready to go out into the world so much yet,” she said. “Allow yourself the flexibility, and a little bit of compassion. Allow yourself to reevaluate, to change your mind, and to try things out.” The same goes for consuming information about COVID. Although staying up to date on local pandemic numbers—case counts, hospitalizations, positivity rates—is important, it’s okay to take a break from doing so if it causes so much dread that you want to disengage entirely from seeking out information about what’s going on. “Sometimes you need to time out,” Coifman said. Unfortunately, while flexibility can help with the stress of post-Omicron life, staying flexible is also harder to do in times of stress, Coifman added. But you can train yourself to get better at it. “We have to increase our tolerance for not knowing what’s to come,” Pauline Boss, a professor emeritus at the University of Minnesota, told me. “The way to increase tolerance for ambiguity is simply this: Do something different.” This can take many forms, such as finding a new route to work or signing up for a class on a topic you’ve never explored. Boss recommends getting to know people outside your bubble. New people and situations allow you to practice adapting to different circumstances and become more confident in your ability to do so. The pandemic could take a number of different directions from here, and this training equips you to handle whatever new or uncomfortable situation may arise next. And although considering the pandemic’s next turn might stoke your anxiety, now is the time to do it. Boss recommended thinking through what you’re going to do no matter what happens: if Omicron was the last big wave, if the current uncertainty continues, and if the pandemic worsens once again. The idea is that you become mentally prepared for any scenario and more willing to accept it instead of waiting for the moment that “it’s either over or it’s not over,” Boss said. “It’s not going to work that way.” By picturing yourself in all these scenarios now, rather than when they happen, you’ll hopefully have a mental playbook for tackling whatever the future throws at us. Fortunately, people have proved capable of flexibility throughout the pandemic. The past two years have been extraordinarily brutal, but in small ways, people have adapted to the chaos and found satisfaction in the things they can control. For me, keeping up with a monthly Dungeons & Dragons campaign has provided both a creative outlet and a sense of regularity. Remember that no matter what happens, humans are quite resilient. “As a field, we used to assume that if bad things happen, people are going to struggle, but we can now have the assumption that when bad things happen, most people are going to be okay,” said Coifman. It’s not ideal, but people can live for a long time with uncertainty, she added. Many people already do. One day, the pandemic will finally end. Until then, it’s important to remember that you’re equipped to handle the ambiguity, even when you don’t feel like you are. Vaccines give us a head start on whatever wave might come next, but don’t undervalue the past two years of experience with facing the unknown. “People are bending with the pressure like a tree bending in the storm,” Boss said. “You’re doing some things differently, and you are being more patient than before. Know that you’re doing better than you thought.” from https://ift.tt/IPMebmq Check out http://natthash.tumblr.com It is common knowledge that COVID risk goes up with age, but how steeply it rises is still astounding to see after two years of living and dying with this coronavirus. Compared with someone in their 20s, a person over 65 years old is not slightly more likely to die of COVID but at least 65 times more likely to die of COVID. Over age 75, they become 140 times more likely to die. Over age 85, they are 340 times more likely to die. No other basic fact of life matters as dramatically as age for COVID. Other common factors associated with risk--race, diabetes, cancer, immunosuppression—make the disease deadlier by a factor of “only” two to four. These are significant differences that influence how doctors care for COVID. But age increases risk by entire orders of magnitude. It is simply in a league of its own. This is why, even though America’s vaccination and booster rates look better in the older groups compared with the young, they are still too low. As a result, deaths in the United States are still too high. The unvaccinated elderly have been dying at incredibly high rates, but even the vaccinated and unboosted elderly are still dying of COVID at four times the rate of unvaccinated adults under 49. A booster cuts that risk dramatically. This is based on detailed CDC data in early December, which are the latest available. Age continues to be the driver of COVID’s brutal math with Omicron, though: In 2022 so far, three-quarters of COVID deaths in America have been in people 65 and older, 93 percent in people 50 and older. 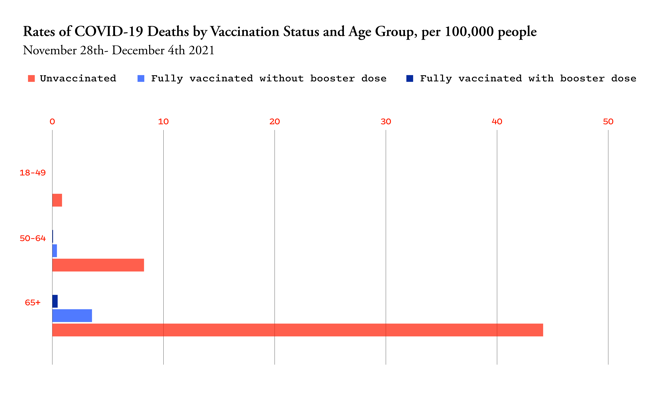
“Our vaccination rates, as well as booster use, in people aged 60- or 65-plus are woefully low and exposes a tremendous amount of vulnerability to severe disease, hospitalizations, and deaths,” says Eric Topol, the director of the Scripps Research Translational Institute. “This has been one of the most serious disappointments in our performance.” Persuading vaccine holdouts among the elderly at this point is hard, but COVID risk is so high for this group that it’s very much worth trying. Boosting the already vaccinated, by contrast, should be eminently doable, as the group is clearly open to vaccines. With America’s vaccination campaign sputtering, this is where efforts are likely to have the biggest payoff. Hospitalizations and deaths are so heavily concentrated in older people, in fact, that a single course of a vaccine in someone over 65 might have the same effect on those numbers as dozens given to the young. The U.S. fortunately has enough vaccine doses that we don’t have to choose whom to vaccinate. But as immunity in the unboosted continues to wane and persuading new people to get immunized becomes harder, a focused effort on vaccinating and boosting the elderly can have an outsize impact on preventing hospitalizations and deaths in the next COVID wave. The most severe COVID outcomes are not the only ones worth preventing, but they are the most urgent if we don’t want hospitals and morgues filling up again. Consider the current Omicron wave, which has been far deadlier in the U.S. than in other highly vaccinated and boosted countries. The U.S. has reached 80 percent of its pre-vaccine peak in daily deaths, compared with only 20 to 30 percent of peaks reached in other countries. America has not only a lower overall vaccination rate but lower coverage in the elderly. England, for example, has achieved 96 percent full-vaccination coverage in people over 65. In the U.S., this number is 88.5 percent, with big geographic variations that range from 79 percent in Arkansas to 95 percent in Vermont. These percentages may all look high, but they represent very different levels of remaining risk. “People see 90 and 95 percent as not very much” of a difference, says Adam Kucharski, an infectious-disease modeler at the London School of Hygiene and Tropical Medicine. He prefers to invert the number. “Think of it as: There’s 5 percent unprotected or 10 percent unprotected.” That doubles the pool of people over 65 who are at high risk for hospitalization and death. In a massive epidemic wave like that of Omicron, hospitalizations and deaths can scale up very quickly. Moreover, the U.S. does lag quite far behind other wealthy countries in boosters for people over age 65. England has boosted 92 percent of its elderly population, while the U.S. is at 65 percent. Even highly vaccinated Vermont is at only 78 percent of seniors boosted. Boosters are necessary because waning immunity and new variants have eroded the spectacular effectiveness seen in 2020’s vaccine trials: Six months-plus after vaccination, two mRNA doses mitigate hospitalizations due to Omicron by only 57 percent across all ages. A booster gets that back up to 90 percent. This extra protection is especially crucial for the elderly because their immune systems tend to mount less robust initial responses to the vaccines. The effects of a third dose may eventually wane too; if any group will need regular boosters in the future, it is again older people—and not just the most elderly. How old is old when it comes to COVID risk? I’ve so far focused on age 65 because the CDC uses this threshold for a lot of vaccination data and because it represents the highest-risk group. But other countries have been more ambitious. Denmark, which dropped coronavirus restrictions amidst sky-high Omicron cases, has been able to do so because it has excellent booster coverage down to age 50. Ninety-five percent of this group has been fully vaccinated, and over 90 percent have had three doses. As a result, Omicron has “been not so bad in terms of health impact,” says Lone Simonsen, an epidemiologist at Roskilde University in Denmark. Cases have fallen a bit off their peak in Denmark, but excess mortality is already back to near zero. To minimize hospitalizations in addition to deaths, Simonsen says the percent vaccinated over age 40 is crucial too, because the median age of COVID hospitalization is lower than that of death. (Hospitalization risk also rises steeply with age, just not quite as steeply as death risk.) Among Danes in their 40s, vaccine coverage is not universal but still very good: 90 percent are fully vaccinated, and three-quarters are boosted. Vaccination uptake among Americans 40 to 65 is even further behind, with even the fully vaccinated rate lingering in the 70s. How could the U.S. maximize vaccine and booster uptake in older Americans? I put this question to several health-policy experts with the more modest threshold of age 65. This seemed more achievable, given the even lower uptake among middle-aged Americans, but also because nearly everyone over 65 is already on government health care—Medicare. England and Denmark have achieved such high vaccination rates in no small part because they have centralized national health-care systems. Health care in America is incredibly fragmented, but Medicare at least reaches most people over 65. In December, in fact, the Biden administration announced that it would mail all 63 million people on Medicare a letter encouraging COVID boosters—“the first time in more than 4 years” that Medicare had sent such a universal notice, the White House touted. At the same time, the agency that oversees Medicare, the Centers for Medicare & Medicaid Services (CMS), laid out a suite of other outreach efforts promoting COVID boosters. CMS could add more direct incentives, experts say. Most Americans on Medicare are on traditional Medicare, which is a fee-for-service program that pays the bills but does not closely manage a patient’s care. CMS does have levers to influence health-care providers, though. It could, for instance, incentivize them by making the COVID vaccination and booster rates among patients a “quality measure” that helps determine how much providers are reimbursed. Medicare already does this with pneumococcal vaccines for pneumonia, says Mark McClellan, a former CMS administrator who is now a health-policy professor at Duke University. Slightly less than half of Medicare recipients are on Medicare Advantage plans, which are run through private insurers such as Kaiser Permanente and Humana that more closely manage a patient’s care. Here, too, CMS could make COVID vaccination part of the plan’s quality measures. And these private insurers, in turn, are “closer to the patient,” says Robert Field, a health-care policy expert at Drexel University, which means they have better data to target patients who still need vaccines. “They can be using their claims data to follow up with people and say, you know, ‘We noticed you got only one shot’ or ‘You’ve gotten two shots and you need a booster,’” he told me. Nursing homes are another potential focus of COVID vaccination. Residents are at particularly high risk for COVID, not just because of age and underlying health conditions but because they live in close quarters. Yet vaccination rates in nursing homes are not any better than in the overall elderly population: 87 percent of residents are fully vaccinated, and only 69 percent are boosted. In general, vaccination rates tend to be lower in for-profit and chain facilities, in those with high staff turnover, and in communities with low vaccination rates, according to a study published last fall. Understaffing and “organizational dysfunction” probably explain why boosters have not been prioritized, says Michael Barnett, one of the study’s authors and a health-policy professor at Harvard. Nursing homes on average turn over more than 100 percent of their staff every year. When staying fully staffed is such a big challenge, simply keeping residents “fed and giving them their meds and helping them use the bathroom—just basic daily stuff is already an overwhelming task,” Barnett told me. “Giving vaccines is a one-time intervention that doesn’t necessarily take that many person hours to figure out. But somebody has to coordinate it and organize it.” Medicare rates the quality of nursing homes too, and CMS could also add COVID boosters to its criteria, as it has with flu and pneumococcal shots. Barnett thinks that this might not be a big enough incentive, given the long list of rating criteria already. Money, however, could be a stronger enticement, and states could also play a role. “There’s nothing stopping a state from offering direct financial incentives,” said Barnett, whether a payment per booster or a cash bonus for hitting a threshold. “To me, it’s a total no-brainer.” These changes are individually incremental, and some may take longer to implement than we would like. But with so many hospitalizations and deaths in Americans over 65, even incremental progress is worthwhile. If immunity in this population wanes and older people need regular boosters, building this system now will make it easier to deliver shots in the future. Vaccines cannot eliminate the risk of COVID among seniors entirely, as everything gets riskier with age, be it a cold or a fall. COVID pills can help bring down hospitalizations and deaths when supply is better available, but this depends on timely testing and access. Vaccines remain our most powerful preventive tool. To avert the worst outcomes of overwhelmed hospitals and high death rates in future COVID waves, we need to get more doses to the people who need them the most. That was and still is the oldest. from https://ift.tt/LG1FRn3 Check out http://natthash.tumblr.com |
Authorhttp://natthash.tumblr.com Archives
April 2023
Categories |
 RSS Feed
RSS Feed
