|
Photographs by Arlene Mejorado and Carlos Chavarría When Antonietta Zuñiga woke up to smoke pouring through her bedroom window, everything she had learned about how to care for her grandson completely left her mind. It was November 2019, in the Los Angeles County city of Pico Rivera. Antionetta’s grandson, Carlos Zuñiga Jr., is schizophrenic; she had the number for ACCESS, L.A. County’s mental-health hotline, taped to her fridge for moments precisely like these. But she knew they were vastly underfunded, and it might take days for them to respond. Frightened and half-asleep, Antonietta picked up her cell phone and dialed 911. About 10 police cars showed up, she says. When they arrived, she recalls, she told the police that Carlos had been off his medication for weeks and refusing to come inside. He’d been collecting trash in the backyard and had set some on fire to warm himself. “He doesn’t do anything because he wants to do it,” she remembers telling them. “He’s doing that because he’s sick.” Even so, Carlos was taken to jail. Five months earlier and about 400 miles northwest, a similar scene had played out in the Bay Area city of Fremont. Police officers arrived at the door of Jose Jaime and Gabby Covarrubias, responding to a 911 call for help with their 20-year-old son, Christian Madrigal. “He needs to go back to the clinic,” Jose, Christian’s stepfather, says he told the police. “Something bad has happened in his mind.” Two weeks earlier, Christian had tried hallucinogenic mushrooms for the first time, and he hadn’t been normal since. “When you looked him in the eyes, he was not our boy,” Jose told me. “His eyes were different. His face was different. Everything was different.” Jose said when the Fremont police arrived, they called for backup and ordered that Christian be brought outside. There, they arrested him for being under the influence of a controlled substance, although his parents maintain that he hadn’t used any drugs since he ingested the mushrooms. When they led him outside the house, Christian began crying out to his mother for help. She and Jose stood by in shock, not knowing what to do. Carlos and Christian weren’t just unlucky. They’re representative of a decades-long pattern of filling up jails with mentally ill people. When policy makers began closing state-run psychiatric hospitals in the 1950s, they promised to replace them with localized mental-health care—but in most places the funding and political will required to make this happen never materialized, leaving large swaths of the U.S. without any options for those seeking treatment. A conservative estimate says 900,000 people with mental illness end up in our jails every year. “These are people who are not necessarily intending to perform criminal acts,” Christine Montross, a psychiatrist and author of Waiting for an Echo: The Madness of American Incarceration, told me. The moment their family members called 911, both Carlos and Christian became unwitting players in a system that is massive, complicated, and, according to many experts, manifestly broken. Both families would come to regret the decision to call the police for help, and Christian would not survive. “We were blind to the fact that something could happen to our son in that jail,” Jose told me. “Completely blind.” [Read: When mental illness becomes a jail sentence] Christian Madrigal was shy and disciplined, and he cared about the world’s problems. At 16, he stopped eating meat out of concern for the climate crisis. When his family ate at restaurants, he would order extra food and give it to homeless people on his way out. When Christian wasn’t playing sports or working out, he liked to snuggle up next to his mom on the couch, taking selfies they would decorate with puppy ears and post on Instagram. But since he’d taken mushrooms, his bad reaction seemed to grow worse each day. He would stare blankly and say nothing for hours, then he would begin weeping, destroying his belongings, and begging to visit his extended family in Mexico. Finally, Gabby relented and bought Christian a plane ticket, but when they arrived at the airport, he broke away from her, charging through the security checkpoint. In the ensuing scuffle with TSA officers, Christian was tased and then taken by ambulance to the emergency room. He was briefly taken to Santa Clara County Jail before being readmitted to the hospital. A day later, the psychiatric emergency room at Santa Clara Valley Medical Center discharged Christian. If he gets worse, Jose remembers the nurse saying, call 911. Ask the police to 5150 him, they’ll bring him back. (Section 5150 of California’s Welfare and Institutions Code allows the police to commit someone to a psychiatric hospital involuntarily if they present a danger to themselves or others.) But Christian’s distress continued. His family tried everything they could think of to calm him, but after two sleepless nights decided to call 911. Christian was not a danger, Jose reassured the officers, but he was worried that the mushrooms had triggered a mental-health issue. But the officers didn’t take Christian back to the clinic. First, they took him to Fremont Jail. After only a few hours there, he was transferred to Alameda County’s Santa Rita Jail. Santa Rita is a mega-jail, the fifth largest in the nation and bigger than most of California’s state prisons. Many of the prisons and jails I’ve visited are loud, with shouting and clanging of cell doors, but when I went to Santa Rita last October, it was eerily quiet. Long, windowless corridors seemed designed to disorient. A robotic cart system made even the food service impersonal. COVID-19 has drawn increased attention to overcrowding and unsafe conditions in jails nationwide, but there’s no evidence that anything has changed in response. At full capacity, Santa Rita can house roughly 3,500 people. Early in the pandemic, the Alameda County Superior Court ordered the sheriff, Gregory J. Ahern, to release as many incarcerated people as he safely could in order to protect those inside from the virus. The jail’s population dropped by about a third—but since then, it’s been steadily rising again. While on average two-thirds of people in the state’s local jails have not been tried or convicted, and are therefore legally innocent, in late 2019 Santa Rita’s number was 84 percent—among the highest in the state. With courts clogged during the pandemic, it’s gone up to 94 percent. [Read: Marketing psychiatric drugs to jailers and judges] “Our jail was designed to do incarceration,” said Ray Kelly, the public-information officer at the Alameda County Sheriff’s Office, after he had welcomed me to Santa Rita and handed me my PPE. “It was never designed to be a mental-health facility.” Yet a conservative estimate says that half of Santa Rita’s prisoners have mental illnesses, with an even higher number suffering from substance-use issues. Ahern has his own vision of Santa Rita’s purpose. In a phone interview two weeks before our tour, he described his role as that of a sheepdog, tasked with watching over the community. “The sheepdog has to look after the sheep, to protect the sheep,” he said. “A sheepdog is very much aware that there are wolves out in the community. The sheepdog is responsible to apprehend those wolves and to see that they’re treated as wolves, and not as sheep.” But legally, those “wolves” are entitled to a certain standard of treatment. Dozens of people currently and formerly incarcerated at Santa Rita have sued the jail, claiming that the people incarcerated there are hungry; that the food is so overcooked it’s inedible; that the cell walls are stained with body fluids, hair, and feces; that arbitrary, long-term isolation is routine; that preventable deaths are rampant. Lisa Fernandez, a reporter at the Bay Area’s Fox affiliate, KTVU, has been tracking every autopsy report: In the past seven years, at least 48 people have died in Santa Rita—a higher death rate than at any other jail in the San Francisco Bay Area. (The death rate in California jails is significantly higher than in the rest of the country.) Seventeen of those deaths were suicides. In 2019 alone, 10 deaths occurred, the most since 2014. Several wrongful-death suits have been filed, claiming excessive force. Another long corridor leads us to the Intake, Transfer, and Release lobby, which I immediately recognize from body-cam footage I’ve now watched numerous times. In the video, two officers carry Christian into the building like you would carry a bench or a slab of wood. His face is obscured by a spit mask made of nylon mesh. His hands are cuffed and chained, and his legs are wrapped together tightly with a restraining device. They place him on the floor, and eight or nine more deputies enter and form a circle around him, chatting among themselves. “He’s not answering questions,” one of the officers had said earlier. “He’s playing the game. He’s been here before, eh?” He hadn’t. Until recently, he’d never had an interaction with the police, good or bad. Jose knew that as Latino men, he and his sons could be targets, so he advised them to always play it safe. “If the cop says dance, you dance,” he told them. “And if the cop says don’t breathe, you just don’t breathe. You do whatever the cop tells you to do.” In the body-cam footage, Christian is unresponsive to the deputies’ questions, but he doesn’t resist or defy orders. Did he know where he was? Was he hearing voices? “When people are what we call ‘internally preoccupied,’ they’re not going to be able to follow instructions,” Christine Montross said. But in a jail, not responding can be interpreted as disrespect. At Santa Rita, I asked Kelly to take me to cell R-1. The cramped, windowless space contained a steel sink and toilet and a concrete bench. I immediately scanned the cell door for the food slot, which played a large part in Christian’s death. 
In the video, a few deputies stand in front of cell R-1, casually debating how to get Christian out of his restraints. Christian lets out an anguished cry. “He’s probably seeing music,” one officer jokes a few minutes later. “Or tasting colors,” adds another. They’ve been told about the mushrooms. Christian remains limp as deputies prop him against the cell door and remove the device wrapping his legs. Next, they nudge him into the cell, with his spit mask, handcuffs, and chain still attached. The lieutenant in charge, Craig Cedergren—who, through his attorney, declined to comment—instructs his deputies to leave Christian’s cuffs on, feed the chain through the food slot, fasten it outside the cell, and close the door. The deputies are visibly uncomfortable with the order. From outside the cell, a Spanish-speaking deputy tells Christian to bend down and let them unfasten the cuffs though the slot, but Christian just says he wants to go home. Cedergren then tells them to leave him like that, chained to the cell door. According to an internal investigation by the sheriff’s office published a few weeks later, Cedergren told the deputies, “I’ve done this a hundred times before. It’s not a problem.” In an email, Cedergren’s attorney told me that “Lt. Cedergren’s decision making was not unreasonable, was based on both training and past experience, and was not countermanded by the Jail watch commander.” Alameda County policy states that all other means must be exhausted before the use of “extraordinary restraint.” In cases where it’s deemed necessary, only a restraint chair can be used. At the time, the policy mandated that the restrained person be checked on every 15 minutes. Accounts vary, but Christian wasn’t checked on for between 30 and 40 minutes. Footage from the security camera shows Christian struggling inside his cell. At 5 p.m., all movement stops. He had contorted his body until the chain attached to his cell door was wrapped around his neck, causing asphyxiation. He died five days later at Eden Medical Center. 
The policies and practices of Carlos Zuñiga’s county would prove slightly more forgiving. Growing up in Riverside, a few suburbs away from his grandmother’s house in Pico Rivera, he had loved to draw complex geometric shapes and read about space travel. “But ever since [the voices] started,” Carlos told me when we spoke last summer, “I lost my hold on my life. It caused me to not care anymore. Sometimes I just want to die.” At age 13, with his father in prison, Carlos ran away from home—the first of many times. While living on the streets for a few months, he tried meth, which he found calmed the voices. At 19, Carlos was diagnosed with schizophrenia, and he moved in with Antonietta. The night Carlos was arrested, his family said, police charged him with residential arson—a sentence that can mean up to eight years in prison—and took him to Twin Towers Correctional Facility, one of several specialized facilities that make up Los Angeles County Jail, this one with a population composed almost entirely of men with mental illness. The next day, Antonietta called her granddaughter—Carlos’s cousin—Diana Zuñiga. Diana works for the county, and she’s a leader in the movement to close jails in Los Angeles and create alternatives. She has advised dozens of families on how to navigate L.A.’s complex systems of jail diversion and mental-health care. Diana grew up in a community gutted by incarceration, with many people she loved spending time in Twin Towers or in nearby Men’s Central Jail. She told me that most of her male relatives have been held in the L.A. County Jail system. “My family members experienced violence in that place,” she said. Almost a third of L.A. County Jail’s population suffers from mental illness, including nearly all of the inmates at Twin Towers, which is larger than Santa Rita. In 2019, Diana became a co-chair of the Alternatives to Incarceration Work Group, set up by the L.A. County Board of Supervisors to determine how to redirect resources from jails to community services like housing, substance-abuse programs, and mental-health care. In early 2020, the work group’s plan was adopted by the board of supervisors. When COVID-19 hit, many of their recommendations were rapidly implemented, and 6,000 people were released. Still, with its population lingering around 12,000, L.A. County Jail remains critically overcrowded. Carlos describes Twin Towers as being like a construction zone: Everything looks the same and smells like dust. For the first two months, he told me, he was given no clothes—just a mat-like garment to cover himself, used for inmates who are considered suicide risks. “We were naked and they had roaches and the toilet didn’t flush,” he said. (The L.A. County Sheriff's Department took issue with that characterization of Twin Towers Jail, and stated in an email that “inmates are only kept inside cells in good working order.”) After COVID-19 hit the jail system and he became terrified of catching it, Carlos tried to keep to himself. “I was having wicked visions of being incarcerated for a long time,” he says. “I would have thoughts about committing suicide.” By the time Carlos got to Twin Towers, the L.A. County Board of Supervisors had already decided they were in agreement: People shouldn’t have to go to jail to get treatment for mental illness. In 2015, the county had opened the Office of Diversion and Reentry, with the goal of identifying “appropriate candidates for diversion” and getting them out of jail. Peter Espinoza, a retired judge and ODR’s director, told me that the office has diverted close to 6,000 people into community-based services over the past five years. “That includes their housing, their medication, their treatment, and their therapies and whatever else it takes to stabilize [them] in the community,” he said. ODR makes this commitment, if necessary, for life. The good news, Espinoza said, is that community beds are much cheaper than jail beds, costing approximately $40,000 per year, versus $219,000 to care for a mentally ill person in jail. Carlos spent five months at Twin Towers before his cousin’s efforts finally paid off. On March 24, he was approved for pre-plea mental-health diversion into SSG Alliance, an in-house facility. He now shares a kitchen and a living room with more than a dozen other people. He’s required to do chores and attend biweekly group-therapy sessions, and staff check on him every hour. It’s boring, Carlos told me, and he wishes more young people lived there. But he’s relieved to be out of jail, and his family is relieved that he’s getting treatment. In November, L.A. County voted to pass Measure J, allocating 10 percent of the county’s $8.8 billion annual budget to diversion initiatives, like alternative crisis-response teams and expanded bed capacity in mental-health treatment centers. “I don’t think we just created a plan,” Diana told me. “I think we created community and shifted culture, in a place that doesn’t normally lift up the voices of people like me and my father and my family that have been impacted by incarceration.” 
Nearly 18 months after Christian’s death, I asked Ray Kelly, the public-information officer, whether the Santa Rita Jail had learned anything from its striking rates of suicide and violence. His answer was vague: “Conversations have taken place,” he told me, and deputies are now being told to “question their superiors” when they’re given an order they believe might fall outside jail policy. “The county jails are left holding the bag because our communities don’t have anywhere else to put these people.” On that point, Kelly is right. Santa Rita, like all jails, is mandated by law to incarcerate whomever they are sent. Alternatives to jail and services for mentally ill people in Alameda County are critically insufficient. Most of the county’s mental-health facilities only house people for a day or two at a time, and are so overpopulated that they regularly turn people away. Arguably, the onus to fund these services is on the Alameda County Board of Supervisors. But instead of increasing funding for mental-health services in communities, the board is funding them in jail: Last May, it agreed to provide up to $106 million annually to hire more guards and mental-health staff at Santa Rita. John Lindsay-Poland, of the advocacy group Decarcerate Alameda County, told me he questions whether hiring more staff will solve the jail’s problems, pointing out that “nearly a dozen deputies were present when the decision was made to chain Christian to a cell door.” Kelly responded, “When you don’t have enough jail staff and mental-health staff, you will have an increase in suicides, behavior-health issues, and lack of intervention and help for the patient.” Ten months after the order to decarcerate, Santa Rita’s population continues to rise. Even if Alameda County did have the beds needed to care for its mentally ill population outside the jail, the current diversion programs wouldn’t be nearly robust enough to fill them. An ACLU study shows that a mere 5 percent of the 36,572 people arrested in Alameda from 2017 to 2018 were referred to diversion. On June 17, 2020, a full year after Christian died, the Alameda County district attorney, Nancy O’Malley, released a report that found there was insufficient evidence to file criminal charges against Lieutenant Craig Cedergren and the deputies involved in Christian’s death. When asked for comment on why she didn’t recommend that Christian’s case go to trial, O’Malley told me, “The sheriff’s department had serious issues, [but] in our professional opinion and evaluation of the law they did not support criminal charges.” (A few days after Cedergren learned that the department intended to fire him, he retired.) 
Christian’s death wasn’t counted as an official “in-custody” death by Santa Rita Jail, because he died at Eden Medical Center. His parents were paid $5 million in the wrongful-death suit they filed, the largest settlement payout in Alameda County since 2015. Jose and Gabby plan to give some of this money to the nurses at Eden, who fought for five days to save Christian’s life. Christian’s death didn’t spark national protests. His two younger brothers have moved to Mexico, where they feel safer, but Gabby and Jose remain in Fremont. Their family is divided, their faith in the system shattered. “Six months, a year, you’ll be interviewing someone else because their son passed away in that jail,” Jose told me. He still fantasizes about how things could have gone differently: “If I would have manned up and punched that officer, I could have been taken to jail and protected my son,” he told me. “He probably would still be here.” For Carlos, having a cousin like Diana in his corner meant everything, but he still feels traumatized by his experience in jail. He has been at the facility in Los Angeles for eight months, and he can’t see his grandmother because of the pandemic. He admitted to me that the program is helping him and he’s glad the voices have gone away, but his future is still uncertain. Meanwhile, death rates—especially suicide rates—in American jails continue to rise. The pandemic could have been used as a chance to rethink how our mentally ill population is cared for, but for now, most people sucked into the system are at the mercy of forces outside their control, and diversion opportunities remain rare. “Things are starting to shift in places like L.A.,” Insha Rahman, the vice president of advocacy and partnerships at the Vera Institute of Justice, told me. “We see one, great outcome for the Zuñiga family, but they are an outlier … That option of finding an alternative to incarceration is still few and far between.” This article is part of our project “The Cycle,” which is supported by a grant from the John D. and Catherine T. MacArthur Foundation’s Safety and Justice Challenge. Additional support was provided by the Alicia Patterson Foundation and the Pulitzer Center; additional reporting was done by Jean Casella, Katie Rose Quandt, and Andrew Stelzer; and additional research was done by Carter Deane, Alexandra Gibbons, and Tash Nguyen. Listen to Stelzer’s radio component on Reveal Podcast here. from https://ift.tt/2Yv0iUk Check out http://natthash.tumblr.com
0 Comments
Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. Last spring and summer, when a COVID-19 vaccine was only a glimmer of hope on the horizon, scientists warned in their careful way that vaccines might not live up to the public’s high expectations. The FDA said a vaccine needed to be just 50 percent effective. The most important thing, scientists told me, was that the vaccines at least protect against severe illness. Then, in the fall, data from the Pfizer and Moderna vaccine trials demonstrated 95 percent and 94 percent efficacy, respectively, against all symptomatic infections. They smashed expectations—and created new ones. In comparison, the results from other vaccine trials look pretty good but unspectacular: AstraZeneca’s vaccine looks to be 70 percent effective; Novavax’s achieved 89 percent efficacy in the U.K., but only 49 percent in South Africa, based on data released yesterday; and Johnson & Johnson’s demonstrated 66 percent efficacy against moderate and severe infection, based on results released today. These numbers are not directly comparable because the different trials were run in different countries, with slightly different protocols, against different versions of the virus. The lower efficacy in South Africa results is likely related to a new variant of the coronavirus, which seems to have evolved to escape immunity. But beneath these top-line numbers is a consistent pattern: All of the vaccines are very good at preventing severe illness and death from COVID-19. That was the original goal for the vaccines, and it is still the most important. “We’re most interested in our ability to keep people out of the hospital and keep people alive,” says Natalie Dean, a biostatistician at the University of Florida. [Read: Why the next phase of vaccination will be harder] Biologically, it makes sense that COVID-19 vaccines would be better at preventing severe infections than mild infections. Think of a vaccine as a dimmer, rather than a light switch. Each shot induces some protective immunity against the coronavirus, even if it doesn’t protect completely. Someone who might have died of COVID-19 without the vaccine could survive with supplemental oxygen. Someone who might have needed hospitalization might experience only a mild infection. A vaccine that confers partial immunity is still better than no vaccine. As it stands, even the lowest efficacy from these vaccines—49 percent against the South Africa variant—is roughly comparable to the efficacy of the annual flu vaccine. Before the results of the mRNA vaccines from Pfizer and Moderna raised expectations, scientists hoped for something similar to the flu shot. “Even that 50 percent range, given the severity of illness and death toll, would have been a game changer,” says Kelly Moore, the deputy director of the Immunization Action Coalition, a nonprofit that works with the CDC and others on disseminating vaccine information. The non-mRNA vaccines have logistical advantages, too. The AstraZeneca, Novavax, and Johnson & Johnson vaccines can all be stored at normal fridge temperatures. In addition, the Johnson & Johnson vaccine is one dose, not two. A one-dose regimen means half as many syringes, half as many appointments, and a much simpler tracking system, making the vaccine much easier to deliver to remote and underserved communities. How quickly these vaccines can help contain a global pandemic will depend on how quickly they can be produced. Johnson & Johnson has fallen behind on its manufacturing and is not expected to catch up until April, according to The New York Times. Novavax’s U.S. trial was delayed because of manufacturing challenges. [Read: The long haul of vaccine results is just beginning ] Additional vaccines—with different mechanisms and different efficacies—do further complicate the messages that public-health officials have to deliver. “These new vaccines provide great opportunities, but they also provide terrific communications challenges,” says Moore. Some people might be tempted to hold out for what looks like a more effective COVID-19 vaccine. But as Moore emphasizes, “any degree of protection is going to be better than putting off protection. This is not the time to be picky. I strongly recommend you go ahead and get it.” Johnson & Johnson is also testing a two-dose regimen for its vaccine; given how vaccines usually work, two doses will almost certainly be more protective than one. It may be that no matter which vaccine you start with, you’ll eventually need a booster—or even multiple boosters, similar to annual flu shots. Vaccine makers are already working to update their vaccines against the South Africa variant. A second variant, from Brazil, has several of the same key mutations and may also decrease vaccine efficacy. And although the vaccines seem equally effective against the U.K. variant, it is more transmissible and becoming only more dominant in the U.K. and elsewhere. The longer the coronavirus runs unchecked and the more people it infects, the more opportunities for dangerous new variants to arise. The global vaccination effort is now in a race against the evolution of the virus—and the more vaccines we have, the better our collective chances. from https://ift.tt/36pW2Ka Check out http://natthash.tumblr.com People are getting vaccinated, but it’s not happening quickly enough. Case counts are dropping fast, but a near-record number of people are still sick. Do we have reason for optimism? Or could optimism still get us in trouble? Alexis Madrigal and Robinson Meyer, staff writers and co-founders of the COVID Tracking Project at The Atlantic, join James Hamblin and Maeve Higgins this week to discuss. Listen to their conversation here: Subscribe to Social Distance on Apple Podcasts, Spotify, or another podcast platform to receive new episodes as soon as they’re published. What follows is a transcript of the episode, edited and condensed for clarity: James Hamblin: With vaccines rolling out and case numbers going down, there’s good news in the air. Are we at the peak nationally, in terms of cases and hospitalizations? Alexis Madrigal: I’ll leave it to Rob to put in the caveats. I feel remarkably optimistic right now, at least for the next month or two. The numbers are really dropping. We’re seeing the lowest case numbers that we’ve seen since November and December. We’re seeing hospitalizations way off their peak and dropping really rapidly. We think deaths are going to have a different path, [given] the lag time between when somebody dies and when it’s reported. I think it could be some weeks before we really start to see deaths really come down. But those things have basically already happened by this point. Obviously, I’m sure the variants seem like this big question mark. But the thing that isn’t a question mark is that there’s been a lot of vaccinations of older people, particularly in the long-term-care facilities, which we think make up 40 to 50 percent of the deaths. And so those two things combined—the falling cases and [having] so many older folks vaccinated—has made me feel pretty good. Maeve Higgins: Rob, I read your piece, and this line, really, it’s been haunting me: “The allure of vaccination is beginning to stymie mitigation policy in some places.” That’s like getting a cut and hearing the nurse is on the way, so you remove the bandages and let it bleed. Can you explain this? Robinson Meyer: Yeah. So Arizona has basically been an epicenter twice: It was one of the worst states during the summer surge, and it was one of the worst states during this current surge. But the governor, Doug Ducey, basically refused to put in any of the public-health measures that he put in in the summer, which did seem to play a role in successfully mitigating the summer surge. He refused to put them in this time, because he said there’s a vaccine on the way, and the vaccine is the true end to this pandemic. So it doesn’t make sense to do anything else, basically. We’ve seen governors and mayors from both parties loosening the measures before cases have fallen. Here in D.C., indoor dining is being allowed again. You can eat indoors now in Baltimore, in Chicago, and in all of Michigan. We’re seeing a general loosening of measures. And the trajectories are moving in the right direction, but the overall levels of illness and infection are still pretty high. There’s still more than 100,000 people hospitalized with COVID in the country right now. That’s more than there ever were over the summer. But the trajectories are really positive. They’re changing really quickly. You can say the trajectories are what matter because hospitalizations are dropping so quickly that we’re going to be back to an encouraging level soon. The problem is that “soon” is still two, three, or four weeks away. In terms of whether we just saw the peak of hospitalizations in the pandemic, period, I think there’s still a big question about whether basically we have time. If you look at the vaccination schedules we expect right now, and barring the arrival of another vaccine, the question is, do we have time for another surge? Madrigal: I’m sure I’ll feel regretful about saying this: I would be stunned if we saw a surge at the same level, unless things turn around really soon. If we follow the pattern of previous surges—which maybe we won’t; there’s question marks about these variants—it’s not like we’ve seen major metro areas have a surge and then three weeks later have another surge. That’s not how it has worked. And at this point, there were so many places that were hit hard in the fall and winter that it would take really different behavior at a population level to see things get really bad again in the next month or two. And during that time is when we’re expecting these vaccines to roll out to people who are 70-plus in fairly large numbers. At a million a day, you’re talking about vaccinating another 30 million people or so. That’s going to be a lot of the deaths. And so even if you were to see some other kind of surge, you’d be in better shape there in terms of the hospital system. Hospital workers will, by and large, be vaccinated. The chance that we have passed the very worst is extremely high, in my view. I’m optimistic about the direction, but the shape of the tail of this is something that I don’t think we have a firm fix on yet. Higgins: Speaking of the new variants, I’m in Ireland at the moment, and what we’re calling the “U.K. strain” has totally taken over our country. The prime minister here said it’s spreading at a rate that’s surpassed the most pessimistic models available to us. Meyer: This is why I might have marginally more concern than Alexis. There are two types of questions here. The first is: How widespread is the U.K. variant in the U.S.? How transmissible is it? Is it so transmissible that populations that have been playing it pretty safe so far are now going to get it using the COVID-avoidance regime that worked previously? Are we suddenly going to open up new populations to the virus? And the second is: Is the U.K. strain the only strain we have to worry about in the U.S.? We’re just not doing that much genomic surveillance of the virus in the U.S. What that means is: If there were, say, an Illinois strain or a Florida strain, we wouldn’t necessarily know. We do know there’s a California strain, but it’s still unclear whether that particular variant is more transmissible in the same way the U.K. strain is, or whether this California strain just got lucky, had a few fluke super-spreading events, and happened to dominate California. Madrigal: Going into the winter, there were a lot of questions about seasonality: what seasonality is, whether it would have a major effect ... And I’m not sure that what seasonality is has been answered satisfactorily. However, clearly, the winter was really bad. And worse than even anticipated in the U.S. And if seasonality was a significant factor, then that should be wind at our back. I feel like I’ve been quite gloomy at times throughout the pandemic about what lay ahead of us. And I guess I think vaccination is being underplayed as a factor in reducing [the] death rate. And it just seems like this mysterious entity of seasonality as a factor also isn’t really coming into a lot of the discussions right now. Maybe that’s just because the variant is sufficiently scary that we don’t want anyone to let up. But that kind of tactical communication—and I’m not saying that’s what Rob’s doing; I think Rob is genuinely concerned about the variants. Meyer: No, I agree with you. I think there is a lot of communication happening right now that’s like Don’t let up, don’t let up, don’t let up that is not as justified by the data. But if you want me to stake my credibility to saying we just saw the absolute worst ever, I would just want to attach a few more unknown unknowns. If we do have another surge, it will be later than we might expect. It’s like looking at distant stars. If you look at a star that’s a hundred light-years away, you’re looking at the star as it was a hundred years ago. Because not everyone gets tested and because it takes time for the virus to incubate, it just takes a lot of time for us to see changes in the world in our data. When we look at cases going down, what we’re really looking at is infections going down a week ago. And if we expect a surge, by the time we even start to see that in the data, it would have to be, like, six weeks from now just because of how long it takes these things to show up in the data. And I think there is a chance that at the very moment that vaccinations really open up to the general public in April, we also see our last peak of cases. I do think Alexis is right though, that we’ll have vaccinated a lot of the most vulnerable population by then. What we’d be more worried about in that final surge is not so much deaths as just: This is not a fun illness to get. There’s a lot of long-term problems that we don’t fully understand. And if we could, [we should] avoid another 50,000 people potentially having to deal with those problems. Hamblin: So you’d be pretty confident saying that we might have another surge in cases, but that we probably passed our peak of hospitalizations and deaths? Meyer: Unless there’s something really wrong with the vaccination data, it would be really hard to get more deaths. Hamblin: So that’s the message people are hearing. It sounds very optimistic. And yet these numbers are still very high, and the way we play this out between now and the summer, it’s easy to lose track of those stakes because the numbers are already so high. Alexis, could you talk about California specifically? Are we potentially letting up on the basis of this future that’s just not quite here yet? Madrigal: The policies that states have enacted have not always had, to me, a totally clear and explicable relationship with what is happening in that state’s data. Some of that is the lagginess that Rob was talking about. California has pulled out of shelter in place. I think the thing that’s really tough for me is: We went into shelter in place a fairly long time ago and it’s hard to see the inflection there [for] the state making an ask of its population, and then [later] them doing something differently.[2] [3] Right now, the numbers in California are borderline unbelievable [in how] encouraging the last, say, five days [have been]. Even a week ago, it was still looking quite bad. And now we’re seeing case numbers that we haven’t seen since November. Hamblin: So was California wrong or right to let up on restrictions? Madrigal: I think there’s such a level of exhaustion that people are kind of just doing what they were going to do anyway. We ran a great story by Julia Marcus about the way that European public-health authorities are playing the vaccine, versus the way we’re playing it in the U.S. European public-health authorities are saying the vaccines are going to make life much better. And I think a burst of Yes, good things are on the way and focusing on the brightness of the light, instead of the darkness of the tunnel, is certainly what I’m telling myself. I’m not sure that I would be able to tell anyone else how they should be feeling right now. But it’s what I need right now in order to maintain the sort of COVID countermeasures that I have been in for what feels like five lifetimes. Higgins: You’ve put so much work into the COVID Tracking Project. Are you going to close it down? Are you going to switch to vaccines? Madrigal: I think, eventually, we’ll stop doing data compilation. From literally the very first day, we [felt] that when the federal government is in play here, that is the correct place to do what we’ve been doing. We’re, like, filling a gap here, not trying to become a federal agency. If we wanted to build the organization as a permanent entity, we could have done vaccine tracking or expanded internationally. But honestly, I want the U.S. government to do these things. I want them to feel responsible for it. Meyer: The irony of all of this is that we started out doing testing data. And we started doing testing data because the CDC actually did publish testing data until February of last year, at which point it stopped for, I think, still-unknown reasons. Of course, we know [former President Donald Trump] was never thrilled with the testing data that came out. At first, we hoped that we would shame the U.S. government into releasing data that we thought they had inside. And then it turned out that they didn’t, in fact, have this data inside, and that the effort of creating it was very labor-intensive and difficult and required hundreds of volunteers and the ad hoc construction of expertise. Madrigal: Yeah. By far the most shocking thing is that the government didn’t have the data inside. And when we came to realize that, [it] was probably one of the worst days of the pandemic, just because of what it said about the overall capacity of the federal government to do this response. from https://ift.tt/2MEWuNK Check out http://natthash.tumblr.com Amid a slow and uneven rollout of vaccines and increasing concern about new variants of SARS-CoV-2, the pandemic indicators we’ve been watching since March reveal that outbreaks are easing all over the country. For the second week in a row, new cases and COVID-19 hospitalizations dropped nationally—17 percent for cases and 10 percent for hospitalizations—though cases and hospitalizations remain much higher than at any point before the fall/winter surge. Tests have also declined, which is not what we’d like to see—drops in tests may mean that more cases are being missed—but this decline follows two weeks of testing data that may have been artificially elevated by the resolution of holiday-reporting backlogs, so it’s difficult to interpret. Reported deaths rose 7 percent this week, with states reporting a total of 22,797 lives lost to COVID-19. Deaths lag behind cases—both because it takes time to die of the coronavirus and because the reporting process for deaths is very slow. Even with cases falling across the United States, we may have another week or more of very high death numbers to come. Residents and staff in nursing homes and other long-term-care facilities are also seeing much-needed improvements. The week running January 15 to January 21 was the first time in four months that both new cases and new deaths in long-term-care facilities decreased at the same time without a holiday-reporting delay. Deaths among residents—who make up about 99 percent of COVID-19 deaths associated with LTC outbreaks to date—remain very high. States reported 5,883 COVID-19 deaths associated with long-term-care-facility outbreaks the week of January 15—about twice as many as were reported at the peak of the summer case surge. The data we publish about long-term-care facilities now include the CDC’s Pharmacy Partnership for Long-Term Care vaccination data. The figures we are able to provide for long-term-care facilities in the United States are an undercount—and we still don’t know how many cases and deaths we’re missing. New York, the epicenter of the deadly first U.S. surge, does not report case numbers for long-term-care facilities, and its death count excludes residents who died in hospitals or other locations outside the facilities where they lived. New York’s attorney general has released a report stating that Governor Andrew Cuomo’s administration has undercounted deaths in nursing homes and other LTC facilities by up to 50 percent. Additionally, neither Arizona nor Missouri releases any cumulative data on LTC cases or deaths. For these states, we’ve partly filled in the missing data by including the figures reported by the states’ largest counties. Nationwide, new cases among white and Black people are down more than 10 percent compared with the previous week, and new cases among Latino people are down more than 20 percent, the second week in a row with fewer new cases for all three groups. Cases among Indigenous people were also lower the past two weeks than during the previous two weeks. We would like to provide similar reporting on race and ethnicity among hospitalized COVID-19 patients, but only 23 states report any race or ethnicity data for hospitalization. The number of new deaths rose this week compared with the previous week for all the race and ethnicity groups for which we have data. A county-level view using case data compiled by USA Facts shows a marked reduction in particularly severe outbreaks in the past month. On December 20, there were 515 counties with a seven-day average of more than one case per 1,000 residents. As of January 24, only 287 counties had outbreaks that were equally severe. This measure tends to highlight areas with small populations and severe outbreaks—even devastating outbreaks in major metro areas have not recently reached such high case concentrations—and this tendency highlights the smaller and more rural counties that may experience locally intense outbreaks without causing state-level numbers to move substantially. The national improvements in hospitalization figures this week reflect a drop in hospitalizations in almost every state—a mirror image of the awful weeks in November when hospitalizations were rising almost everywhere at the same time. Only a single state, Vermont, saw hospitalizations rise this week, but by only 2 percent. (Vermont currently has fewer than 50 people hospitalized with COVID-19.) It’s the first week since November 5 that no state has reached a new record high for current hospitalizations. Hospitalizations are still very high—much higher than at any time before the third case surge arrived this fall—but they are now about one-quarter of the way back toward the baseline of about 30,000 hospitalizations that we previously experienced in early October. The number of people with COVID-19 in U.S. hospitals is also dropping faster now than it did in August, when we previously saw a sustained drop in hospitalizations. In California, cases are down 50 percent over the past two weeks on the seven-day average, from 42,000 new cases reported each day two weeks ago to just over 21,000 new cases a day yesterday. Hospitalizations are following behind more slowly—about 18,000 people are currently hospitalized with COVID-19 in California, down from a January 7 peak of about 23,000. California has lifted its stay-at-home orders throughout the state this week, which will allow outdoor dining and personal services to resume. A new preprint from UC San Francisco’s Department of Epidemiology and Biostatistics covered in Eater Los Angeles found that food-service and agriculture jobs occupy three of the five occupations associated with the greatest risk of dying of COVID-19 in California, with restaurant cooks at the top of the list. (This research is based on death records from the California Department of Public Health and has not yet been peer-reviewed.) Latino Californians make up more than half of the food-service workers classified as essential, and 85 percent of agricultural workers, according to the Los Angeles Times. Deaths are still rising in California, and more than 10,000 of the state’s total 36,000 COVID-19 deaths were reported after January 1; 4,500 of these deaths were reported in L.A. County. CBS Sacramento is investigating why so many California counties say they’re out of vaccines despite the state’s Vaccine Dashboard showing more than 2.1 million unused vaccine doses at the end of last week. Arizona is still reporting the highest number of COVID-19 hospitalizations per capita in the country, but its outbreak continues to ease, though much less dramatically than California’s. New daily cases are down 28 percent from two weeks ago on the seven-day average, from about 9,600 on January 13 to about 6,900 yesterday. COVID-19 hospitalizations in Arizona are down 16 percent from the state’s January 12 peak. Despite this, 92 percent of all ICU beds were occupied on Tuesday, more than half with COVID-19 patients. Also on Tuesday, of the 91 percent of inpatient beds that were occupied, 49 percent were occupied by COVID-19 patients. Vaccines continue to be distributed throughout Arizona, including to a homeless-health-care nonprofit in Maricopa County that hopes to serve state residents who lack access to traditional vaccination sites and processes. Georgia is now reporting the second-highest number of COVID-19 hospitalizations per capita in the country. The state saw its highest-ever number of hospitalizations on January 13, and has seen that figure fall about 17 percent since. This comes as Atlanta Magazine reports that the Georgia Registry of Immunization Transactions and Services has experienced technical difficulties resulting in “dramatically underreported levels of vaccine administration statewide.” Simultaneously, the NAACP has filed a lawsuit alleging that conditions in a privately owned Georgia prison—including crowding, poor sanitation, and minimal testing for COVID-19—have led to increased exposure to the virus within the prison. We are also continuing to closely watch the data reported by the high-population states New York and Texas, where hospitalizations now seem to have turned the corner and are improving. Concerns over known and newly emerging variants of SARS-CoV-2 continue to grow. As scientists scramble to determine how potentially more-transmissible versions of the virus may affect vaccine efficacy, public-health officials are doubling down on the importance of reducing transmission to avoid another surge in new cases. In several states and metro areas, added stress on already overtaxed health-care systems would be catastrophic for patient care and outcomes. Outbreak epicenters such as Los Angeles are starting to see an uptick in the percentage of variant cases among samples that are tested, and any new, variant-worsened surge in an area where hospitalizations are still very high would be devastating. Unfortunately, the U.S. is still not doing enough genomic sequencing to understand how widespread the variants have become. During yesterday’s White House COVID-19 press briefing, CDC Director Rochelle Walensky stated that resources are available to support states in processing thousands of samples. But until we get more complete data, we can’t know whether the variants we see in the headlines are to blame for any increase we may see in COVID-19 cases or hospitalizations. Although the virus is (expectedly) changing, the ways to prevent infection are not, so our best weapon against existing SARS-CoV-2 variants and to prevent the evolution of more variants is to keep doing what we know works: Wear masks, practice physical distancing, wash your hands, and avoid indoor gatherings. from https://ift.tt/3iWT8kX Check out http://natthash.tumblr.com In the spring, after my beloved, overpriced New York exercise studios closed one grim “In these unprecedented times” email after another, I did what any aspiring workout enthusiast with a little cash to burn might do: I got out my credit card and I bought monthly subscriptions to three different online classes. The era of kidding myself that I would actually exercise at home had begun. I started with a virtual edition of a class I had attended in person. I pushed my bed into the farthest corner of the room, away from the dresser where I’d set up my laptop, freeing up the only six remaining inches of space in which I could move. I lit a candle. I shut the door. I lifted my arms to begin—well, first I paused to check if my neighbor could see me through the window--then I began. A few minutes later, my partner texted from the next room to tell me that I was stomping and breathing loudly enough to make an off-camera appearance on his Zoom call. Also, I was scaring the dog. That was the end of that experiment. Fortunately for my checking account, my livelihood doesn’t hinge on my performance as an athlete. On January 16, a flight from Doha, Qatar, full of tennis players and their coaches touched down in Melbourne for the Australian Open, one of the four biggest tennis tournaments of the year. Soon after, all of the passengers received an email: Someone on the plane had tested positive for COVID-19. It was the third flight headed to the tournament on which this happened. All the players going to Australia knew that they would encounter a “modified” quarantine protocol, giving them just five hours outside their hotel room each day (strictly choreographed for the athletes to get to and from the practice courts and gym with as little contact as possible). But in light of the coronavirus cases, the Australian government would require everyone on the affected flights to “hard quarantine” for 14 days. No exceptions, including the freedom to leave their hotel room, would be made for the players. After all, Australia’s near elimination of the coronavirus didn’t happen by accident. Seventy-two athletes, 14 days of court-free-tennis fitness to maintain. No hitting partners, no physiotherapy visits, no kidding. [Read: The thrilling unpredictability of women’s tennis] A microcosm of pandemic absurdity was born. Before last week, Google results for “How to train for a Grand Slam in your hotel room” would have turned up empty. Searching that phrase now is to encounter a treasure trove of almost voyeuristic delights. Image upon image is available of some of your favorite players—in living quarters approximately the size of a falsely advertised Manhattan studio apartment—serving balls into propped up mattresses, squat-pressing a leather reading chair, and celebrating negative COVID-19 test results with pizza delivery. The athletes received stationary bikes courtesy of the event organizer, Tennis Australia, to help with indoor cardio. The American player Tennys Sandgren plucked his from the floor and lifted it over his head. Heather Watson, a top British player, completed a 5K by literally running back and forth across her room.
At any hour of the day, the players are on social media, posting about boredom or anxiety, just like the rest of us fed up with quarantine. They get stir-crazy. They stop shaving. The occasional grumbling appears in a fleeting Instagram story, but for the most part during all of my swiping, I found everyone in admirable spirits, the sheer athleticism of their footwork drills hypnotic. Sometimes the makeshift circumstances can get pretty noisy. “In the beginning, you would hear sounds occasionally, more from players playing video games, but now it’s constant background noise,” Andrea Petkovic, one of the athletes in modified quarantine, told me. “Players hitting balls against the walls, players throwing shit around, players jumping, players running in place. It would be hilarious if you were not about to have a nap but can’t because the person upstairs decided to do their daily workout.” Other players have dropped the gimmicks for more typical quarantine workouts. The New Zealand player Artem Sitak, set to play doubles in the tournament, arrived in Melbourne on a flight from Los Angeles. After he learned that someone on his flight had tested positive and that he would be stuck in his hotel room for two weeks, he posted a thoughtful video explaining how he’d known the risks of traveling to Australia mid-pandemic. I reached out to Sitak on Instagram to get a sense of his daily routine. His three-hour workouts, which he starts after lunch, sound vaguely like something I would never make it through at a CrossFit gym I would never attend. First, he bikes at high intensity for an hour (admittedly not his favorite activity; he prefers to run). Then he switches to a series of wall squats, lunges, jump lunges, free weights, and medicine-ball and core work. Everything is wrapped up with stretching and foam rolling. And, like most of us, it’s Netflix before bed. Isn’t staying in shape incredibly challenging to do in quarantine? “It’s all in the mindset,” Sitak assured me in an Instagram message. “I decided on day one that it wouldn’t be difficult. I’ll have a set program each day and I’ll stick to it. Now here we are on day twelve and I feel great mentally.” Oh, okay. But seriously, isn’t staying in shape incredibly challenging to do in quarantine? [Read: The healthiest way to sweat out a pandemic] I asked Paul Annacone, a former coach to Roger Federer and Pete Sampras, what effect the forced quarantine might have on players. He wasn’t particularly optimistic. “I can’t imagine not hitting a tennis ball, or even not being outside, for 14 days, all within a couple days of playing a professional tennis tournament,” he said. (Annacone now coaches Taylor Fritz, an American up-and-comer who is playing in the tournament but is not one of the 72 players in hard quarantine.) The Australian Open starts on February 8, so the players currently in their rooms will have more than a week to make the most of their court access once their isolation period is over. But still, two weeks in the lead-up to a Grand Slam without the regular rhythms of daily practice matches and physiotherapy, or fine-tuning responses to a hitting partner’s strokes and movements, is a significant disadvantage. Many professional tennis players pick up their first racket in early childhood—Novak Djokovic and Rafael Nadal both started playing when they were 4 years old—and it’s a reasonable expectation that some may go years or even decades without spending two weeks off the court. Otherworldly talent certainly helps (cue Federer), but for most pros, success is largely the result of consistency and relentless repetition. One tactic to fend off rust, Petkovic suggested, is to play “shadow tennis.” “Either actually take the racket and swing while you imagine hitting balls,” she said, “or just hold it in your hand when you’re rewatching Friends for the umpteenth time. This way the body gets used to it and it won’t feel so foreign once you step on the court.” The rose-tinted view is that this unexpected period of rest could actually do the players some good. During the 2008 Olympics, in Beijing, the American runner Shalane Flanagan came down with food poisoning and had to forgo training to sleep and rehydrate before the 10,000-meter race. She won the bronze. Not bad. Could there potentially be any benefits to all of this? I posed the question to Rennae Stubbs, the former top doubles player in the world. “None whatsoever,” she said. Meanwhile, for those of us without the glory and the glamour of a Grand Slam to train for, we do what we can. A few nights ago, as I hunched forward and scrolled through Twitter for player updates, a flash of movement caught my eye. It was my next-door neighbor jumping up and down in his living room. Burpees. Unmistakable. I squinted, and saw the familiar outline of a pumped-up instructor on his television. At least he was trying. from https://ift.tt/2L0k9ro Check out http://natthash.tumblr.com Video collages by Sara Serna You need to be a certain kind of person to want a reality-TV show about yourself. Jeffrey Young was one of those people. In 2016, Young, who was 42 at the time, invited a cameraman to shoot a pilot episode about his life as a nurse practitioner in Jackson, Tennessee. It doesn’t sound like much of a sell—a middle-aged man doling out medical advice in a city midway between Memphis and Nashville. But Young was eager to let the world know that he was no typical nurse practitioner. Throughout Jackson, he had created for himself a reputation as a rock-and-roll renegade, happily showing off his piercings, tattoos, and goatee. He blasted heavy metal at his private practice and filled his Instagram feed with photos of himself smoking cigars. In his frequent social-media updates, he would drink and flip off the camera. Though he was not an M.D., Young christened himself “the Rock Doc.” His vision was, evidently, to one day launch a reality series of the same name. The pilot footage—some of which Young posted to YouTube, and some of which I obtained from a person who was once close to Young—portrays the Rock Doc as a medical bad boy who’s willing to break free from the establishment to deliver real talk. In confessional-style interviews, Young seems to enjoy offending anyone who’s shocked by his approach. In one scene, he and his best friend, a pharmaceutical representative named John Kevin Phillips, broadcast themselves on the video-streaming app Periscope. With a heavy “Mercy me,” Phillips produces a pair of women’s panties from a bag. Young grabs them and takes a big whiff. “Let’s see here, she’s 23,” Young says. “Brown hair, green eyes, amazing body.” He smells them again. “And no education whatsoever,” Phillips jokes. Defending himself in one of his on-camera interviews, Young acknowledges that he is “maybe a little untraditional” and that he “might like to drink a little bit after hours.” But, he says, “I’m very passionate about what I do … I work hard, but I play harder.” Young’s practice was, for a time, an inexpensive, reliable option for medical care in Jackson. The waiting room often overflowed with patients. Young put his name behind charity projects around town, took health insurance, and offered discounts for people who otherwise couldn’t afford care. He exhibited a certain tenderness as he filled syringes and sutured skin. For the cosmetically minded, he hosted alcohol-fueled Botox parties. Young was, in short, a medical provider who acted like everyone’s best friend. As the cameraman who filmed the pilot told me, “Everywhere he went, it was like the Beatles.” But the way in which Young gained some of these fans has become the focus of a federal court case. In April 2019, he was indicted on drug-trafficking charges, along with five other medical providers in Jackson, two of whom were the supervising physicians Young, as a nurse practitioner, was required to have. Young and the others were among dozens of doctors, nurses, and pharmacists arrested across seven states, targets in the nation’s largest takedown of medical providers related to prescription opioids. Prosecutors say Young used his rebellious persona to take advantage of patients, distributing highly addictive painkillers on demand and in large quantities for profit—and, often, his own sexual gratification. At least 50 women are thought to have come to the clinic to have sex with Young, some of them allegedly doing so in exchange for drugs, according to court testimony. (Young has pleaded not guilty to all charges. Through his attorney, he declined to comment on this and the other allegations in this story because of a gag order issued by the judge in the case.) Over the past two decades, opioids have claimed more than 450,000 American lives. Though many of these deaths have been caused by street drugs such as heroin and illegally manufactured fentanyl, the nation’s opioid epidemic was sparked by the kinds of painkillers medical providers prescribed. The allegations against Young point toward an especially sordid type of abuse in which some doctors victimize patients twice: first by getting them addicted to drugs, and then by sexually exploiting them. In the past five years, at least 40 medical providers nationwide have been accused of exchanging sex for addictive drugs. As so often happens with irresponsible medical providers, Young’s popularity in the community—along with an indifferent, slow-moving bureaucracy—allowed him to operate for half a decade despite initial warning signs and then multiple arrests and investigations. One other factor might help account for his long, illicit career: the sheer number of patients who stood by him, almost to the very end. In an attempt to understand how Young got away with so much for so long, I’ve spent more than a year tracking his story, reading court documents, and examining his extensive digital footprint. In May 2019, shortly after Young was indicted, I traveled to Jackson to try to understand the place that gave rise to the Rock Doc. Then and over the ensuing months, I spoke with dozens of Young’s friends, enemies, alleged victims, and former co-workers. Many of the people I interviewed—including some of Young’s former patients and employees—asked to remain anonymous, often because they feared retribution at the hands of Young and his friends. Others accused me of seeking to discredit Young and slander his name. I visited Young’s clinic, but, through a staffer, he declined to speak with me. Jackson, a city of about 70,000 people, looks like almost any midsize patch of America that sprang up sometime after the Pilgrims but before Microsoft. Downtown has an old-fashioned square, a few coffee shops striving for trendiness, and some suburban standbys—McAlister’s Deli, Kohl’s, Chili’s, Panera Bread—all connected by well-maintained roads and featuring black oceans of parking lots. Still, the city’s southernness peeks through. On my trip, I strolled by a glass case near the federal courthouse that held a large Bible opened to the Gospel of John. A restaurant called the Little Rebel displayed a Confederate flag. There is a friendliness, too, that one associates with the South. “We’re small enough where we still talk,” Jerry Gist, who was the mayor at the time, told me. Jackson’s cheeriness, though, is at odds with the population’s somewhat grim physical health. Nearly a fifth of the city’s residents live below the poverty line, and many are afflicted with chronic diseases that often accompany the stresses of a low income. Obesity and diabetes are rampant; so is chronic pain. To deal with the latter, the city, like so many others in America, has become ever more reliant on opioids. A woman I spoke with who has worked for seven doctors’ offices in the area estimates that about three-quarters of medical visits there result in an opioid prescription. One patient she knew kept a cane in the trunk of her car and visited doctors’ offices with it in order to appear disabled so she could get more pills. Throughout the opioid epidemic, a distressing number of doctors have seen a perverse opportunity in Americans’ suffering. Many medical providers are small-business owners who operate with limited oversight from authorities. Health care is one of the Jackson area’s most important industries, and West Tennessee Healthcare, which once employed Young, is the largest employer in the county. Young grew up in Bethel Springs, a 700-person village near Jackson. In his early adulthood, he was a straitlaced young Republican who had short hair and wore a tie much of the time, one of his former co-workers told me. He graduated from Union University, an evangelical Christian school, in 1995, then earned a degree from the University of Tennessee College of Nursing in 2003. Young got married, then quickly got divorced, according to several people who knew him then. He remarried in 2006. In 2012, Young was working at a cardiology practice in Jackson when, with a consultant named Rich Reitz and cardiologist named Dharmesh Patel, he set up a side business giving talks to doctors about treating heart attacks and strokes. Before long, the three men hatched a plan to found a network of health clinics that would check patients’ cholesterol levels and offer diet and exercise advice. The clinics’ aim would be to halt the parade of miseries—heart attacks, early deaths, hospital bills—brought on by the obesity epidemic. In September 2014, Young, Reitz, and Patel opened their first clinic and called it PreventaGenix. Reitz says he and his girlfriend came up with the unwieldy name—a futuristic combination of prevent and genetics. (Patel did not respond to requests for comment.) The men each contributed $40,000 to the endeavor. The clinic sat on a quiet road crammed with other medical practices—a sleep doctor, a dentist, a nephrologist, an orthodontist—each in its own brick McMansion. PreventaGenix, with its Doric columns and grand portico, appeared to preside over the rest. 
At first, Young seemed to Reitz like an affable, outgoing dad who loved rock and practiced medicine. But Young soon revealed a blustering personality that started to overwhelm the team project. Rachel Fullington, an early employee of Young’s, told me Young wanted the clinic’s atmosphere to be loose and fun, while the others wanted it to be more buttoned-up. Young seemed eager to hire lots of staff, but would end up firing them later. A few months into their new venture, Reitz and Young were supposed to meet to discuss the running of the clinic. Instead, Young began by kicking Reitz out of the business, Reitz told me. Patel left soon after. Fullington, who was also let go, told me she got a threatening call from Young. “If you speak against me,” she remembers him saying, “you’re gonna regret it.” Once his colleagues were out of the business, Young began crafting a persona based around rock music and hard living. He decked out PreventaGenix with psychedelic artwork and set the stereo to loud rock. On Instagram, photos tagged #preventagenix show Young on a motorcycle, surrounded by women. “Don’t worry, my tattoos don’t like you either,” one image reads. No one could quite tell me who or what was responsible for Young’s transformation. Some speculated that it could have been drugs, alcohol, the prospect of fame, a divorce from his second wife the year after PreventaGenix launched, or a combination of all of them. Whatever the inspiration, his new persona was good for business. As Young collected more tattoos and befriended more local bands, he began to attract a certain clientele. “When you got all kinds of money,” said Jon Benjamin Sharp, a local musician who used to see Young around town, “you got all kinds of friends.” (Sharp made clear that he himself wasn’t a fan of Young’s.) Strippers, tattoo artists, and rock-band groupies saw a kindred spirit in Young and came to him as patients. Phillips, Young’s best friend, would often stop by the clinic to hang out and drink, according to former employees. The next morning, the office manager, Kristie Gutgsell, would clean up after them. Sometimes the two men would fight, and broken glass would litter the floor. (Later, Phillips pleaded guilty to threatening a Drug Enforcement Administration agent who was investigating Young. Through his lawyer, Michael R. Working, Phillips did not return several requests for comment. In an email to The Atlantic, Working said that when it came to Phillips’s actions, “there was no direct threat. There was no statement even made to the Feds. Phillips popped off to a friend.”) Young was late to the office almost every day. A former employee said that staffers had to go to Young’s house—another McMansion—to drag him out of bed, and that he would occasionally arrive at the clinic drunk. One employee recalled him sometimes being too drunk to see patients. They would shut off the power so they had an excuse to close the clinic on those days. While Young’s antics could be a nightmare for his staff, his pool of patients increased as word about his practice spread. Young was a “people pleaser,” as one former employee described him. This ingratiating tendency allegedly extended to handing out prescriptions. Young became known for putting drugs into the hands of almost anyone who asked. Employees I spoke with said he eventually was seeing 50 to 85 patients a day, compared with about 20 for the average doctor, and most of them seemed to be on opioids. (Young’s attorney claimed in court that only about 25 percent of his patients were.) At Young’s practice, the quantities of opioids were “larger than many investigations that I conducted,” Shirley Pickering, a nursing-board investigator, later said in court. Nurse practitioners have played a key role in Tennessee’s opioid epidemic. Opioid manufacturers such as Endo, the maker of Opana, and Purdue Pharma, the maker of OxyContin, targeted high-volume providers, in particular generalists, nurse practitioners, and physician’s assistants, “who generally had less expertise in pain management and were more receptive to marketing from sales consultants,” according to a lawsuit filed by the state of Tennessee against Endo in May 2019. (Endo denied the allegations.) Sometimes patients seeking opioids go to different providers until they find one who is willing to prescribe to them. And doctors—who work in what is, after all, a service profession—sometimes feel that it’s easier to pacify the patient than to push back. Otherwise, fledgling practices, in particular, risk losing patients. If PreventaGenix staffers suspected that a patient was abusing drugs, they would sometimes try to “fire” the patient, by telling him or her not to return to the clinic. Though Young claimed that he also fired drug-seeking patients, Gutgsell testified in a deposition that he would meet some patients after hours and write them prescriptions anyway. He seemed, to his former employees, constitutionally unable to deny patients the pills they wanted, even if it was the last thing they needed. Young’s second marriage was already in trouble by the time PreventaGenix launched, and after his divorce he quickly found new girlfriends. He would sometimes brag about having sex on his lunch break, sharing with his staff pictures of his conquests, three employees said. They learned to ignore it. At other times, PreventaGenix staffers would stumble upon a woman he had brought to the clinic the previous night. Women were drawn to Young; he had a big house and was the first to buy everyone’s drink. PreventaGenix had a back door, and before long employees started noticing that some female patients would come in through it and go directly to Young’s office. Young seemed to have been expecting them. As many as three women a day allegedly came to his office for sex, though one former employee said Young might have had sex with more women after hours. Former employees speculated that he met the women in bars. Young would call these liaisons “nooners” or say it was “tap-that-ass Tuesday,” according to court testimony. (One employee, Karla Wright, testified later that she had never seen Young have sex with women at the office.) Young’s sexual desires and need to please patients allegedly soon blurred together. He messaged at least five female patients about sex and filling prescriptions, prosecutors would later say, detailing the anonymized encounters in court. (They relied on messages obtained by agents during the investigations into Young.) When one patient told Young over Facebook Messenger that she was “in shitty health and about to jump off a bridge,” he prescribed her a cocktail of several different drugs, including fentanyl. “I accept all insurance,” he told her. “Will be glad to take the balance out of your ass.” He asked another patient, to whom he prescribed the opioid hydrocodone, to come in for a “checkup” the following day and “wear a short skirt and no panties.” Young was sometimes even more direct. To a different patient, he wrote, “Come fuck me at my office right now.” It is not illegal for doctors to have sex with their patients, though it’s considered unethical. Some of the doctors who have been accused of exchanging drugs for sex in recent years threatened patients that they would cut off their supply of painkillers if they didn’t gratify them. Young appeared to operate more subtly. One former employee told me it’s not clear whether Young was “exchanging” prescriptions for sex or just giving his many girlfriends the medications they asked for. “Thank you for taking care of me, not just the sex and satisfaction but the Soma too,” wrote one patient, referring to a muscle relaxer. Some female patients opted for a service the clinic offered that Young called “VIP status,” in which they paid $500 a year to skip the waiting room and get Young’s cellphone number, one former employee said. Other female patients’ checkout sheets simply said “No charge.” Though he portrayed himself as harmlessly vulgar, Young could, in fact, get violent with women. He has been arrested several times, though not convicted, for assaulting women. According to police reports and court records, his second ex-wife, Dawn, claimed that throughout their relationship Young repeatedly pushed, threatened, and attempted to rape her. In 2011, the couple got in a fight while visiting Panama City Beach, Florida, and “it was determined that Young did throw, or shove, Mrs. Young from the bed to the floor,” the police report reads. (Dawn did not press charges at the time, and she declined to speak with me for this story.) Some of Young’s dalliances with his patient-friends similarly took a dark turn. A woman I’ll call Stephanie developed a friendship with Young a few years ago when she was regularly seeing him for swelling in her throat. (Stephanie asked me to use a pseudonym for her because she doesn’t want her name associated with the case.) In addition to steroid shots, Young prescribed her oxycodone, Xanax, and Adderall for her various medical issues. Stephanie would accompany him to different clubs in the area, and wherever he went, she said, he was surrounded by hired bodyguards and friends she called “bouncers,” who were around for the times when he drank too much or flirted with women and got into fights with their boyfriends. Stephanie had been in an abusive relationship and dealt with a slew of other traumas. Being around Young made her feel emotionally safe, she said. During one club night, Young bought Stephanie two drinks and his friends handed them to her. Minutes after finishing the second drink, Stephanie fell face-first onto the floor. Rather than call for help, Young “walked away and left me on the ground,” she told me. Two bouncers made sure she got home, but when she woke up in bed the next morning, her eyes were black, her nose was broken, and her mouth was bleeding. She doesn’t think Young was the one who drugged her, but she believes nevertheless that she was drugged. Even after this, she returned to Young as a patient. 
She wasn’t the only patient to stick by him. Long after the criminal charges against him became known, many of Young’s patients and friends came to his defense—including some whom he had seemingly wronged. Lots of people refused to talk to me because they fear Young, but many others refused because they love him. To date, none of the alleged victims in Young’s court case has come forward publicly to speak against him. One person with knowledge of the case gave me a list of several women who, the person believed, were having sex with Young in exchange for drugs. (Court records do not contain the names of Young’s alleged victims.) Of the women who returned my calls, none wanted to speak on the record under her real name, but all denied that Young had sexually abused them. One admitted that Young had flirted with her. Another compared Young to “a brother” and called my reporting “disrespectful.” Young’s devotees have maintained for years that he was a great man on a noble mission, and that people who spoke against him didn’t understand his radical approach. Whenever he ran into trouble, his fans would fill his social-media feeds with pledges of support. “I am sick of people only judging you by what you do in your personal life,” one woman wrote on his Facebook page in September 2016, when Young was charged with assault after a woman claimed that he had screamed at her in the parking lot of his office. (The case did not result in a conviction.) Several people suggested suing for defamation a news station that reported on the incident. Many people in Jackson seemed to see themselves in Young. They liked his plainspoken approach to medicine, a profession typically associated with jargon and elitism. They described Young to me as intelligent, as knowing almost as much as a doctor would know—or maybe even more. He found diseases, for example, that other doctors missed. One of his patients, Helena Louvaris, told me that Young “saved her life” by putting her on a diet plan. She appreciated that he asked about her grandkids. The “Rock Doc” affectations, Louvaris said, merely show that he’s different from other doctors. “He didn’t pull any punches,” she said. “He didn’t mind saying a curse word or two.” Dan Reaves, a local radio host on whose show Young occasionally appeared as part of a marketing plan, described Young as medically gifted. It’s a shame, he told me, that Young got into so much legal trouble; think of all the people he might have helped. Several others dismissed the notion that Young could be sexually coercive. His friend Melanie Lupino, a local bartender, said he got girlfriends easily, so she was baffled by the notion that he would have to give people drugs to get sex. She doesn’t believe the allegations against him, and chalks them up to pure jealousy. It’s a small town; people talk. Stephanie, who returned to Young’s clinic after the incident at the club, said Young helped her more than any doctor she’s ever seen. No one else seemed capable of treating all her problems—throat swelling, high blood pressure, attention issues. Though both she and Reaves said Young should be held accountable for anything he did wrong, Stephanie told me that she forgave him. Young cared for all kinds of people, some of whom didn’t have money or health insurance. His Rock Doc persona helped him connect with patients who might never have felt comfortable in a traditional doctors’ office. Most doctor appointments, after all, average a nerve-racking 17 minutes, in which you spill out a complicated medical history and pray the doctor has a good solution. To have a medical provider be polite to you, accept you, maybe even dig through your charts to find the root cause of your ailments—it can be validating. Even if the treatment doesn’t work, it feels good to be listened to when you’re used to being ignored. At the same time, building himself up as a renegade nurse practitioner seems to have allowed Young to sweep his faults under the rug of unconventionality. Of course other doctors don’t write as many prescriptions, the implication seemed to be. Other doctors don’t post pictures of themselves with motorcycles and scantily clad women, either. Young’s story raises the question of where care crosses into harm. How far can medical providers go in giving patients what they want? Despite some patients’ praise for Young, the evidence that he routinely walked far over that line remains alarming. And the consequences might have gone beyond sexual abuse and addiction. In 2014, Young began seeing a patient identified as “MY” in a letter from Tennessee’s department of health—a letter that would ultimately lead to a nursing-board hearing for Young. MY came to PreventaGenix complaining of lower-back pain and numbness in his left arm, and asked for refills of pain medications. Without doing a physical exam, Young diagnosed MY with chronic lower-back pain and anxiety, the letter details. He refilled MY’s prescriptions for Percocet and Valium, and also prescribed him hydrocodone. Throughout Young’s year-long treatment of MY, Young failed to conduct pill counts, consult a state database meant to monitor the dispensing of controlled substances, and discuss with MY the risks of combining these drugs, according to the document. In August 2015, Young prescribed MY what the letter calls a “dangerous combination” of an opioid, a benzodiazepine, and a muscle relaxant. MY died on August 25, 2015, from an apparent drug overdose. He was found in his bedroom, where the ambulance service discovered an empty syringe under his pillow and empty pill bottles on his bedside table that had been filled that month. Some of the pills had been prescribed by Young. The cause of death, according to the letter, was “a probable cardiac event due to polypharmacy, or the simultaneous use of multiple drugs.” Rather than suffer any real consequences for his allegedly reckless prescribing, Young continued to work as a medical provider for years. Over that time, his online following grew. Having hordes of fans seems to have allowed Young to buy more deeply into his own rock-and-roll fantasy, which in turn gave him the confidence to broadcast his life through even more videos and updates. “If a patient would text him a compliment, he would blast it all over Facebook,” one former employee told me. Young had an active channel on Periscope, where he and Phillips drank and waxed philosophical. “Am I a misogynist, or do women just like rough sex?” Young asks himself in one video. In another, he totters around with an empty bottle of bourbon and pans the camera over to Phillips, who is asleep on the couch. “He’s so cute … that’s my brother and my best friend,” Young says, giving Phillips a gentle kiss. Young was by no means nationally or even regionally known. His followers across social-media accounts numbered in the low thousands—higher than a casual user’s, but a trifle compared with even a C-list celebrity’s fan base. Young did seem to be famous enough in Jackson, however, to reinforce his own grand vision of himself. His small fiefdom of followers created a mini echo chamber, feeding back approval and encouragement. This social-media stardom appears to have helped inoculate him against concerns that his loose approach to medicine could harm anyone. Young’s pursuit of fame culminated in his attempt to launch the Rock Doc television show. The cameraman who shot the pilot, who requested anonymity because he doesn’t want to be associated with Young’s case, heard about Young through a mutual friend and visited him several times to shoot footage for what he hoped could become a reality show. He gave Young total control over what was recorded. Though Young at first just seemed to go along with the project, he grew more invested after the first visit, the cameraman told me. The resulting videos are typical scenes from a medical practice—people donning gloves, waiting in chairs—spliced together over a heavy-metal soundtrack. The camera follows Young as he treats patients, talks on a local radio station, dances with women at a club, and brags about drinking. The scenes are meant to serve as a testament to the effectiveness of Young’s “work hard, play harder” ethos. Supposedly candid confessions from Young about his life are interspersed with complimentary interviews with patients. An obese man explains that Young helped him with his swollen leg. “I swear he didn’t look at my leg for 30 seconds, and he told me exactly what it was,” he says. The man says if he were ever shot, he would go to Young before going to the hospital. But tonally, much of the footage betrays him. Young cries at his son’s fifth-grade graduation, then explains that he’s so emotional because his nurses are having their periods. Young and Phillips, both longtime musicians, reveal that they’re working on some rap songs about Young’s “haters,” then ponder how to do gang signs. People who criticized Young swiftly became his enemies. “You may not like my rock and roll, you may not like my piercings, you may not like my sexy-ass beard, but you know what? You can all suck my dick!” he yells at the camera in one Periscope video, a stethoscope around his neck and a cigar in his hand. He raises a glass filled with red wine, as if in a toast. When one video was apparently manipulated by one of his detractors and posted online, Young threatened whoever might have done it. “Trust me, I got people,” he says to the camera. “We’re tracing your fucking account now, so you better be prepared to reap the whirlwind of your bullshit.” As he gathered followers, Young began to deploy his social-media presence to hunt down and intimidate his former employees and ex-friends, some of whom told me they felt threatened by Young and his followers. Some sought counseling, slept under their beds, or carried guns. One former patient who had a falling-out with Young told me he or someone associated with him attacked her on the internet forum Topix, calling her a “whore” and a “drunk.” She said her home address and photos of her adult daughters were posted on the site, along with rape threats directed at her daughters. (Topix has since been shut down.) The former patient told me she became afraid to leave her house. “We can’t live if he’s out,” she said. “We’ll all be killed.” It helped that Young had prominent friends he could call on for help. Some of his patients were police officers whom he would occasionally ask for favors. In February 2016, he texted one of his opioid patients, a police officer named Jay Green. Young wanted information about one of his enemies. “I need you to find this fucker,” he wrote, according to court testimony later reported by The Jackson Sun. (Green, who has since cut ties with Young, would not comment on this when I reached him, but he told the Sun that he asked another officer to look up the information.) Eventually Shirley Pickering, the nursing-board investigator who was looking into the allegations against Young, also grew terrified of him. She would get phone calls at her house, answer, and hear only strange whispers, she said in a court hearing. She would wake up to find that all her car doors had been opened overnight. She once saw someone running across her yard into the woods. “Do you feel safe with Mr. Young being out there?” a prosecutor on the case, Andrew Pennebaker, asked Pickering in court. “I am very nervous about it,” she replied. How was a nurse practitioner whose behavior was so outrageous allowed to treat patients for so long? Despite the accumulation of evidence suggesting that Young was running his practice recklessly and endangering patients, he remained licensed to write prescriptions for five years after PreventaGenix opened its doors. Officials were well aware of the allegations surrounding him over this period: The state’s health department had received at least 13 complaints about Young since 2015. But none of these barred the Rock Doc from getting drugs into the hands of patients. Years before the launch of PreventaGenix, Young had already been accused of abusing his nurse-practitioner license. By 2012, Young was allegedly supplying testosterone without a clear medical reason to high schoolers who wanted to bulk up. One young man told me he went to Young’s house that year to pay cash for a vial, knowing that a traditional doctor would be unlikely to prescribe testosterone to a healthy teenage boy. (Four years later, the health department received a complaint about this testosterone sideline, but the complaint was never assigned to an investigator, according to Pickering.) Around 2013, Young allegedly prescribed hydrocodone, a benzodiazepine, and Adderall for a patient whose visits he described as a “concierge-type thing,” Pickering said in court. Young failed to diagnose the man’s hypertension and overprescribed to him, according to court testimony, and later the patient suffered a stroke. The lack of oversight in the Young case is in keeping with practices seen throughout the opioid crisis. The entire epidemic has been an unending story of doctors, pharmaceutical executives, and public officials blithely ignoring signs of danger. There’s clear evidence that opioid manufacturers knew the drugs were addictive, yet they marketed them aggressively anyway. (The drugmaker that is most often blamed for the epidemic doesn’t agree with this assessment: “Suggesting that activities that last occurred more than 16 years ago are responsible for today’s complex and multifaceted opioid crisis is deeply flawed,” a Purdue Pharma spokesperson, Robert Josephson, said in a statement to The New York Times for a story on this issue.) Early in the epidemic, Purdue gave doctors OxyContin fishing hats and swing-music CDs to encourage them to prescribe more of the drug. American doctors went on to prescribe opioids at much higher rates than their counterparts in other countries. The resulting addictions were blamed on reckless patients, rather than the fundamental chemistry of the opioids themselves. Young benefited from an almost reflexive societal trust in the medical profession. Multiple surveys show that people tend to trust health-care workers more than they trust many other professionals, including police officers and clergy members. “Nurses are consistently rated higher in honesty and ethics than all other professions that Gallup asks about, by a wide margin,” the polling firm said in a January 2020 survey. Many people trust doctors even when they’re harmed by their treatment, and a 2008 study found that people are more likely to spend time researching a new employer or a new car than vetting a new surgeon. At the beginning of the opioid epidemic, “the autonomy of doctors to prescribe opioids was almost limitless,” Keith Humphreys, a Stanford University professor who researches mental-health policy, says. Similarly, Young appeared to get the benefit of the doubt from virtually everyone. States largely rely on medical boards to regulate practitioners, but these entities have a reputation for leniency. They are often too under-resourced and understaffed to keep a watchful eye on all medical providers. Even when they do, the boards are mainly composed of doctors’ and nurses’ peers, who can be reluctant to throw the book at one of their own, says Rebecca Haw Allensworth, a Vanderbilt University law professor who has studied medical boards. Patients, meanwhile, don’t always know that medical boards exist in the first place, or that they can complain to them if they’ve been wronged, Lisa Robin, the chief advocacy officer for the Federation of State Medical Boards, says. Tennessee’s nursing board, the main agency that has power over nurse practitioners in the state, launched its investigation into Young within a year of PreventaGenix opening. But the board has a history of letting suspicious providers go on practicing for years. It moved so slowly in punishing drug-addicted nurses that some were able to get new jobs and steal narcotics while under investigation, an eastern Tennessee news station, WJHL, found in 2016. (In response to a request for comment, a health-department spokesperson noted that, according to state law, the department can’t suspend medical licenses without first giving practitioners the opportunity to demonstrate compliance regarding the allegations against them. This requirement is waived, however, in cases where “public health, safety, or welfare imperatively requires emergency action.”) As the nursing board’s investigation of Young inched along, another agency launched its own probe into the Rock Doc. In July 2016, the Tennessee Bureau of Investigation began looking into allegations that Young was overprescribing opioids. One agent testified in court that the bureau had uncovered Facebook messages such as one sent to Young in August 2016 by someone known in court as “SW”: “My girl for eight years is an addict … You write her any more scripts you’re going to kill her, man.” Meanwhile, many of Young’s patient charts had allegedly stopped being monitored: One supervising physician came in once, reviewed Young’s charts, and withdrew from the supervising agreement immediately based on what he saw. Pharmacists began to refuse to fill his prescriptions. In November 2016, the health department threatened to file charges against Young before the board of nursing. The department suggested that he surrender his license in order to resolve the matter quickly, but according to a report from The Tennessean and The Jackson Sun, a defiant Young rejected that offer. His case before the nursing board stalled for two more years. The first move of any significant consequence for Young came in early 2017, when the DEA raided the clinic. One January morning, officers swarmed the road outside the PreventaGenix building, guns drawn. They entered the office and ordered the clinic’s staffers to lie on the floor. The agents seized about 350 of Young’s patient charts and every computer in the office, according to Gutgsell, the former office manager, and the notice of seizure states that about 10,000 individual doses of hydrocodone were also taken. (The DEA declined to comment on Young’s case for this story.) The agency also searched Young’s cellphone. On it, they found evidence of Young having sex with many different women, one of whom appeared to be motionless and had her eyes closed, a DEA agent testified later. After the raid, Young spent the night in jail on an outstanding warrant, and PreventaGenix closed soon after. But that did not put a stop to Young’s ambitions. He soon opened a new clinic, which he called GeneXis Health. The clinic mostly offered cosmetic treatments, and it was located in a strip mall in a more industrial part of town, next to a chiropractor and a place called Gene’s Tire & Wrecker. Young would continue to prescribe drugs there for two more years. The allegations against Young seemed to take a toll on him, though. Like many actual rock stars, he flamed out on his own extravagant lifestyle. Toward the end of PreventaGenix, the nurse practitioner so many people had praised deteriorated, according to former employees. Patients would spend an hour or two in the waiting room, only to get a rushed exam and prescription. Young began arriving at the clinic smelling rancid, with greasy hair, and the clinic’s money problems mounted. Doctors’ offices make money by billing insurance companies for the services the providers perform, but it was hard to do this at PreventaGenix because the documentation for Young’s visits was so shoddy. He would try to squeeze in even more patient visits each day—sometimes well over 50, former employees say—and would either forget to document services or would document services he hadn’t provided. Young had also allegedly begun siphoning off $100 almost every day from the clinic for his personal expenses, according to former employees. The cost of producing the Rock Doc pilot, about $2,000, was entirely paid for by the clinic, Gutgsell claimed in a deposition. When PreventaGenix closed, Young was alleged to have failed to pay part of the unemployment insurance, federal tax withholdings, and final payroll for the clinic, according to a lawsuit filed by his former partners, Reitz and Patel. After PreventaGenix shut down, Young told his patients on Facebook that they could contact Reitz and Patel’s attorney to get their medical records. Once again, there was an outpouring of support. “I can’t wait to start being your patient again,” one woman wrote. After he opened the new clinic, Young’s sexual behavior with patients allegedly continued, as did the town’s willingness to ignore it. In 2018, a woman told police that Young put his hands down her pants during an office visit, but that apparently led to nothing. (“There were different Jeff Youngs in [the Records Management System] and I had very little information so he was not added to the report,” the police report states.) According to a medical-board report, one employee recalled Young having sex in his office with a patient who appeared to be drugged; when Young left, she was passed out on the couch. In March 2019, the health department received a complaint that Young had inappropriate sexual contact with patients, and sent him a letter of warning without disciplining him. (Young has denied that he’d had sex with the patient who appeared to be drugged.) November 7, 2018, marked the beginning of legal repercussions for Young. About four years after its investigation began, the nursing board finally held a hearing to consider his fate. Young neither “admits nor denies the following allegations,” Tracy Alcock, a lawyer with the state health department, said at the hearing, but he “acknowledges that the department’s proof would show the following”: From August 2013 to November 2016, Young prescribed controlled substances in amounts and for durations that “were not medically necessary, advisable, or justified for a diagnosed condition.” The board put his license on probation for two years, during which time he could not prescribe certain Schedule II or Schedule III controlled substances, including drugs such as oxycodone, fentanyl, Vicodin, and Adderall. He would still be allowed to prescribe testosterone and cough syrup with codeine, however. In 2020, had he not been indicted, he would have been allowed to petition to have his prescribing privileges reinstated, as long as he agreed to extra monitoring. Though the system came slowly for Young, during the years he was being investigated America underwent a national reckoning about opioids. In the past two decades, overdoses involving prescription opioids have killed more than 232,000 people—the population of Jackson several times over—and the major players in the epidemic are finally being held to account. The manufacturers and distributors of prescription opioids have been sued by dozens of states and municipalities for the damage they’ve allegedly caused. In recent years, the Justice Department has started coming for unscrupulous doctors and pharmacists, too. Though criminal cases against doctors and nurse practitioners like Young are still relatively rare, they are growing more common. Ultimately, what hastened Young’s downfall is that some of the female patients asking him for drugs were undercover officers. On April 17, 2019, officials swept through Appalachia, charging 53 medical professionals, including doctors, nurses, and pharmacists. Young was among them. His indictment implicated him and two of his former supervising physicians, Alexander Alperovich and Andrew Rudin, and alleged that Young’s “motives in prescribing controlled substances to his patients were often to obtain money, notoriety, and sexual favors.” Alperovich and Rudin, the indictment claims, “accepted money derived from the proceeds of the conspiracy in exchange” for their “purported supervision.” (Both have pleaded not guilty. Rudin’s lawyer did not respond to a request for comment. Alperovich’s lawyer declined to comment.) At this point, the people of Jackson knew the full extent of officials’ suspicions about Young. Yet he still attracted patients at GeneXis prior to his detention hearing in May 2019. Weeks after the indictment made national news, the clinic was packed with people coming and going, one woman who worked in a building with a view of the parking lot told me. (She did not want to be named for fear of jeopardizing her business.) When I visited the clinic shortly before the hearing, Young had just finished up with a patient. A staffer, who declined to talk on the record, asked me why I was writing about him. “This is a bunch of bull crap,” she said. For the occasion of his detention hearing, Young wore a cerulean suit and a comb-over. His black shirt collar didn’t quite hide the tattoos on the back of his neck. As the court spent two days scrutinizing his years of alleged misdeeds, he sat mostly silently. Occasionally he would glare at his ex-wife Dawn, who was in the gallery. “By the end of this hearing, you will be asking what on Earth took the medical board so long,” Pennebaker, the prosecutor, said in court. After the hearing, Young was jailed pending his trial, which is currently scheduled to be held this spring. Part of the judge’s reasoning was that Young’s Facebook posts showed “a propensity for violence.” Young continued blogging from jail, somehow managing to write a few posts for a website that promotes medical providers’ rights to prescribe opioids freely. In one post, tagged with “American holocaust,” he writes, “I have always been a survivor and have scars of significance to symbolize thus, and this is where they have underestimated me and my resolve.” In March 2020, after the coronavirus pandemic broke out, Young petitioned the court to be released to house arrest because he was on immunosuppressive drugs for a kidney transplant he had years ago and was concerned about the risk of complications from COVID-19. The judge denied this request, in part because, he wrote, “Young has chosen to not wear a mask or practice social distancing consistently in jail.” In September, Gutgsell, Young’s former office manager, was indicted for aiding Young in prescribing opioids without a legitimate medical purpose. She pleaded guilty. With Young at least temporarily behind bars, some of his fans seem to have reached a point of disillusionment with the Rock Doc—or, at least, a point of fatigue. “Watching this makes me really sad,” one YouTube user commented on the Rock Doc pilot in 2019. “Dang, Jeff … What happened?” Helena Louvaris and Melanie Lupino, two of Young’s staunch defenders, both declined to speak with me when I called them back to see if they still supported him after he was jailed. Meanwhile, LeAnn Naylor, the secretary of Jackson’s former mayor, first told me over email that she stood by Young after his hearing, but then recently said she’d started having doubts because Young would frequently hit on her adult daughter. However, many of Young’s online supporters have remained loyal. When the local news station, WBBJ, posted a story about Young’s case on Facebook, the usual chorus of defenders raised their voices. “He’s a great doctor and never has he acted any way towards me but professional!” one woman wrote. “He’s prescribing drugs that people want,” another man added. “So what? Who cares?” All throughout the past few months, Young’s fans have papered his Facebook wall with loving messages. “Never give up … God is full of second chances,” one woman wrote. Another said, “I was thinking of you today and how much you have helped me.” We won’t know if Young is guilty of everything the government says he is, or how much additional time, if any, he will serve, until later this year. But the allegations against him point toward what can be permissible, even celebrated, in a medical system built on profit. Whether or not Young is convicted, the perverse incentives for doctors to see patients for short visits and to prescribe too many unnecessary drugs will remain. The opioid epidemic—which appears to only be getting worse—has made clear that wherever pain exists in America, grifters will follow. from https://ift.tt/39ow37G Check out http://natthash.tumblr.com
Dear Dr. Hamblin, I’m a 65-year-old art teacher who has non-Hodgkin’s lymphoma and rheumatoid arthritis. My small town in Georgia issued a mask mandate, but it was overruled by the governor, so I’m still avoiding stores. When I have had to venture out, I see many fools without masks. When I go to the drive-in at my pharmacy, the young lady covering the window has consistently had her mask pulled below her nose and, sometimes, below her mouth. Not wanting to be considered a “Karen,” I’ve kept my concerns to myself. How should I say something? Anonymous Georgia Dear Anonymous, I understand the impulse to confront this person. At the same time, I agree if complaining about retail workers is typically gauche, doing so during a pandemic can be vulgar. Although some of us have been able to safely work at home, many millions have continued doing high-risk jobs, often for low wages, without sick leave or hazard pay. Many are asked to wear a mask for the entire time they are at work. Wearing a mask all day, every day is a significantly greater imposition than wearing one only when briefly leaving home. That said, the woman you describe is working in a pharmacy. That means she is coming into regular contact with sick people, and with people who have chronic conditions, like you. Your dilemma involves more than just considering your own welfare, or hers. So, unlike asking to speak to someone’s manager because he forgot to hold the pickles, there’s a moral case for speaking up. Silence means tacit approval of a situation that puts other people—especially other workers—at risk. We shouldn’t be so concerned about mishandling the situation that we choose to do nothing at all. [Read: Why aren’t we wearing better masks?] In the absence of legal mandates, social codes are the way we establish and maintain norms. A mask is a medical device, but also a symbol of empathy and unity. Ideally, that’s enough to reinforce the code: Everyone wears a mask so everyone else wears a mask. But the world is not ideal. When people inevitably break the code, an intervention needs to be done in a way that doesn’t further degrade the mutual respect on which this code depends. The answer definitely doesn’t involve stopping to berate every maskless person you pass on the sidewalk, no matter how therapeutic that may feel. Whether or not maskless people “deserve” to be reprimanded, criticizing or glaring at them could very well make the problem worse. The goal is to convince people to care—to be conscious and thoughtful of others, to help keep everyone safe. It’s not a goal we’ll reach, but in a situation like yours, we can nudge ourselves in that direction in small ways. I see three ways that you might work toward that end. Ideally, if you have a rapport with this person, there’s a way to explain your position to her. You’re a high-risk individual and you’d really appreciate it if she could pull her mask up. Statements of genuine concern followed by a request for help are generally more effective than anything that feels like scolding. Keep in mind that many people decline to wear masks because they resent being told what to do. Telling them what to do—louder or more aggressively—is unlikely to solve the problem, and likely to make it worse. This can be difficult and awkward, especially with someone you don’t know, and especially when you don’t want to have a prolonged conversation with this maskless woman. A second option is to consider writing a note to her. This can seem passive-aggressive, so you would have to be doubly or triply sincere in showing that you’re simply concerned and that a change in behavior would mean a lot to you. Maybe include some candy. A third option is to go over this person’s head. Doing it tactfully is not impossible, though there are many wrong ways to approach it. This is where things could quickly escalate into a “Karen” attitude—one that reveals callous entitlement and assumes that the world exists to serve you, in your attempt to summon the force of entrenched power structures to exact revenge over some perceived slight. The employee may get reprimanded by her boss, and may even lose her job, not because the infraction justified it, but because the customer’s show of dissatisfaction was so extreme. So, yeah, don’t be that person. [Read: How ‘Karen’ became a coronavirus villain] If you’re going to speak to an owner or a manager, do so in a way that serves a greater goal than attempting to target just this woman’s behavior. If an employee isn’t wearing a mask, treat it as an oversight of the business and its management. Without naming anyone specific, call and say that you’ve been at the store several times recently and noticed employees who weren’t wearing masks. Express your genuine concern and say that you won’t feel comfortable continuing to do business there if this doesn’t change. The key to avoiding Karen-ness seems to be remembering that you’re not interested in exacting punishment, and that it’s not even within your purview. It’s also not your job to achieve 100 percent mask compliance everywhere you go. All you can do is make your concerns known, with maximum empathy, in a way that leads to an outcome that could potentially help save lives. If you can’t bring yourself to speak up, there is power in the collective action of consumers who refuse to patronize places that don’t keep customers and employees safe. If you and enough others can take your business elsewhere, the message will be clear in the one language to which we know the profit-driven health economy does respond. “Ask Dr. Hamblin” is for informational purposes only, does not constitute medical advice, and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. By submitting a letter, you are agreeing to let The Atlantic use it—in part or in full—and we may edit it for length and/or clarity. from https://ift.tt/2M30jMK Check out http://natthash.tumblr.com A few months ago, when millions of Americans were watching the Netflix series Emily in Paris because it was what we had been given that week, I cued up the first episode and was beset almost immediately by an intense longing. Not for travel, or for opportunities to wear beautiful clothes—two commonly cited high points in an otherwise charmless show—but for sports. Specifically, watching sports in a packed bar, which is what the titular character’s boyfriend is doing when the viewer meets him. The scene is fleeting, and it’s also pretty bad. It doesn’t come close to capturing the sweaty intensity of a horde of nervous fans, poised to embrace each other in collective joy or drink through despair. I know this because I am, sometimes unfortunately, a person who has spent a good chunk of her adult social life watching sports in bars, both with my actual close friends and with 500 or so fellow travelers at the New York City bar that hosts expatriated University of Georgia alumni during college-football season. During the pandemic, I’ve been able to maintain, on an outdoor TV, the ability to watch a game with a couple of my closest buddies, which is a balm. But the other experience—the one Emily in Paris was trying to portray—has been lost entirely. In noticing all the ways the show misunderstood its joys, I realized how much I missed it, and especially how much I missed all of those people I only sort of know. Of the dozens of fellow fans and bar employees I’d greet with a hug on a normal fall Saturday, I follow only a handful of them on social media; for most of the others, I know only the first names, if that. But many comforted me through mutual, bone-deep disappointment, or sprayed champagne at me in exhilaration. In the weeks following, I thought frequently of other people I had missed without fully realizing it. Pretty good friends with whom I had mostly done things that were no longer possible, such as trying new restaurants together. Co-workers I didn’t know well but chatted with in the communal kitchen. Workers at the local coffee or sandwich shops who could no longer dawdle to chat. The depth and intensity of these relationships varied greatly, but these people were all, in some capacity, my friends, and there was also no substitute for them during the pandemic. Tools like Zoom and FaceTime, useful for maintaining closer relationships, couldn’t re-create the ease of social serendipity, or bring back the activities that bound us together. Understandably, much of the energy directed toward the problems of pandemic social life has been spent on keeping people tied to their families and closest friends. These other relationships have withered largely unremarked on after the places that hosted them closed. The pandemic has evaporated entire categories of friendship, and by doing so, depleted the joys that make up a human life—and buoy human health. But that does present an opportunity. In the coming months, as we begin to add people back into our lives, we’ll now know what it’s like to be without them. American culture does not have many words to describe different levels or types of friendship, but for our purposes, sociology does provide a useful concept: weak ties. The term was coined in 1973 by the Stanford sociologist Mark Granovetter, and it comprises acquaintances, people you see infrequently, and near strangers with whom you share some familiarity. They’re the people on the periphery of your life—the guy who’s always at the gym at the same time as you, the barista who starts making your usual order while you’re still at the back of the line, the co-worker from another department with whom you make small talk on the elevator. They’re also people you might have never directly met, but you share something important in common—you go to the same concerts, or live in the same neighborhood and frequent the same local businesses. You might not consider all of your weak ties friends, at least in the common use of the word, but they’re often people with whom you’re friendly. Most people are familiar with the idea of an inner circle; Granovetter posited that we also have an outer circle, vital to our social health in its own ways. During the past year, it’s often felt like the pandemic has come for all but the closest of my close ties. There are people on the outer periphery of my life for whom the concept of “keeping up” makes little sense, but there are also lots of friends and acquaintances—people I could theoretically hang out with outdoors or see on videochat, but with whom those tools just don’t feel right. In my life, this perception seems to be largely mutual—I am not turning down invites from these folks for Zoom catch-ups and walks in the park. Instead, our affection for each other is in a period of suspended animation, alongside indoor dining and international travel. Sometimes we respond to each other’s Instagram Stories. [Read: The pandemic has remade friendship] None of the experts I spoke with had a good term for this kind of middle ground—the weaker points of Granovetter’s proposed inner circle and the strongest of the weak ties—except for the general one. “Friend is a very promiscuous word,” William Rawlins, a communications professor at Ohio University who studies friendship, told me. “Do we have a word for this array of friends that aren’t our close friends? I’m not sure we do, and I’m not sure we should.” The extent to which individuals are separated from their moderate and weak ties during the pandemic varies by their location, employment, and willingness to put themselves and others at risk. But even in places where it’s possible to work out in gyms and eat inside restaurants, far fewer people are taking part in these activities, changing the social experience for both patrons and employees. And even if your job requires you to come in to work, you and your colleagues are likely adhering to some kind of protocol intended to reduce interaction. Masks, though necessary, mean you can’t tell when people smile at you. Friends are sometimes delineated by the ways we met or the things we do together—work friends, old college buddies, beer-league-softball teammates—but they’re all friends, and Rawlins thinks that’s for the best. “Living well isn’t some cloistered retreat with just a few folks,” he told me. “The way worlds are created is by people sharing with and recognizing each other.” Many different kinds of relationships are important, he says, and man does not thrive on close friendships alone. This realization, new to me, is also somewhat new in the general understanding of human behavior. Close relationships were long thought to be the essential component of humans’ social well-being, but Granovetter’s research led him to a conclusion that was at the time groundbreaking and is still, to many people, counterintuitive: Casual friends and acquaintances can be as important to wellbeing as family, romantic partners, and your closest friends. In his initial study, for example, he found that the majority of people who got new jobs through social connections did so through people on the periphery of their lives, not close relations. Some of the most obvious consequences of our extended social pause could indeed play out in the professional realm. I started hearing these concerns months ago, while writing a story on how working from home affects people’s careers. According to the experts I spoke with, losing the incidental, repeated social interactions that physical workplaces foster can make it especially difficult for young people and new hires to establish themselves within the complex social hierarchy of a workplace. Losing them can make it harder to progress in work as a whole, access development opportunities, and be recognized for your contributions. (After all, no one can see you or what you’re doing.) These kinds of setbacks early in professional life can be especially devastating, because the losses tend to compound—fall behind right out of the gate, and you’re more likely to stay there. [Read: The pandemic is changing work friendships] The loss of these interactions can make the day-to-day realities of work more frustrating, too, and can fray previously pleasant relationships. In a recent study, Andrew Guydish, a doctoral candidate in psychology at UC Santa Cruz, looked at the effects of what he calls conversational reciprocity—how much each participant in a conversation talks while one is directing the other to complete a task. He found that in these situations—which often crop up between managers and employees at work—pairs of people tended to use unstructured time, if it were available, to balance the interaction. When that happened, both people reported feeling happier and more satisfied afterward. Now Guydish worries that reciprocity has been largely lost. “Zoom calls usually have a very defined goal, and with that goal comes defined expectations in terms of who’s going to talk,” he told me. “Other people sit by, and they don’t get their opportunity to give their two cents. That kind of just leaves everybody with this overwhelming sense of almost isolation, in a way.” This loss of reciprocity has extended to nondigital life. For example, friendly chats between customers and delivery guys, bartenders, or other service workers are rarer in a world of contactless delivery and curbside pickup. In normal times, those brief encounters tend to be good for tips and Yelp reviews, and they give otherwise rote interactions a more pleasant, human texture for both parties. Strip out the humanity, and there’s nothing but the transaction left. The psychological effects of losing all but our closest ties can be profound. Peripheral connections tether us to the world at large; without them, people sink into the compounding sameness of closed networks. Regular interaction with people outside our inner circle “just makes us feel more like part of a community, or part of something bigger,” Gillian Sandstrom, a social psychologist at the University of Essex, told me. People on the peripheries of our lives introduce us to new ideas, new information, new opportunities, and other new people. If variety is the spice of life, these relationships are the conduit for it. The loss of these interactions may be one reason for the growth in internet conspiracy theories in the past year, and especially for the surge in groups like QAnon. But while online communities of all kinds can deliver some of the psychological benefits of meeting new people and making friends in the real world, the echo chamber of conspiracism is a further source of isolation. “There’s a lot of research showing that when you talk only to people who are like you, it actually makes your opinions shift even further away from other groups,” Sandstrom explained. “That’s how cults work. That’s how terrorist groups work.” Most Americans were especially ill-prepared for the sudden loss of their weak ties. The importance of friendship overall, and especially friendships of weak or moderate strength, is generally downplayed in the country’s culture, while family and romantic partners are supposed to be the be-all and end-all. The physical ramifications of isolation are also well documented. Julianne Holt-Lunstad, a psychologist and neuroscientist at Brigham Young University, has found that social isolation increases the risk of premature death from any cause by almost 30 percent. “The scientific evidence suggests that we need a variety of kinds of relationships in our lives, and that different kinds of relationships or social roles can fulfill different kinds of needs,” she told me. People maintain hygiene, take their medication, and try to hold themselves together at least in part because those behaviors are socially necessary, and their repetition is rewarded. Remove those incentives, and some people fall into despair, unable to perform some of the crucial tasks of being alive. In people at risk for illness, lack of interaction can mean that symptoms go unnoticed and arrangements for medical care aren’t made. Humans are meant to be with one another, and when we aren’t, the decay shows in our bodies. The small joys of running into an old co-worker or chatting with the bartender at your local might not be the first thing you think of when imagining the value of friendship—images of more intentional celebrations and comforts, such as birthday parties and movie nights, might come to mind more easily. But Rawlins says that both kinds of interactions meet our fundamental desire to be known and perceived, to have our own humanity reflected back at us. “A culture is only human to the extent that its members confirm each other,” he said, paraphrasing the philosopher Martin Buber. “The people that we see in any number of everyday activities that we say, Hey, how you doing? That’s an affirmation of each other, and this is a comprehensive part of our world that I think has been stopped, to a great extent, in its tracks.” Rawlins describes the state of American social life as a barometer for all that is going on in the country. “Our capacity for—and the possibilities of—friendship are really a kind of measure of the actual freedom we have in our lives at any moment in time,” he told me. Friendship, he says, is all about choice and mutual agreement, and the broad ability to pursue and navigate those relationships as you see fit is an indicator of your ability to self-determine overall. Widespread loneliness and social isolation, on the other hand, are usually indicative of some kind of larger rot within a society. In America, isolation had set in for many people long before the pandemic, making it one of the country’s many problems both exacerbated and illuminated by extended disaster. In some senses, that means there’s cause for optimism. As more Americans are vaccinated in the coming months, more people will be able to return confidently to more types of interactions. If the best historical analogue for the coronavirus outbreak is the 1918 flu pandemic, the Roaring ’20s suggest we’ll indulge in some wild parties. In any case, Rawlins doubts that many of the moderate and weak ties people lost touch with in the past year will be hurt that they didn’t get many check-in texts. Mostly, he predicts, people will just be so happy to see one another again. All of the researchers I spoke with were hopeful that this extended pause would give people a deeper understanding of just how vital friendships of all types are to our well-being, and how all the people around us contribute to our lives—even if they occupy positions that the country’s culture doesn’t respect very much, such as service workers or store clerks. “My hope is that people will realize that there’s more people in their social networks that matter and provide some kind of value than just those few people that you spend time with, and have probably managed to keep up with during the break,” Sandstrom said. America, even before the pandemic, was a lonely country. It doesn’t have to be. The end of our isolation could be the beginning of some beautiful friendships. from https://ift.tt/3chbCLR Check out http://natthash.tumblr.com The Grants Pass Clinic in southern Oregon is more than ready to administer the COVID-19 vaccine to its 20,000-some patients. It has seven exam rooms devoted to vaccination. The staff has ordered fridges and syringes. The phones ring nonstop, with patients calling to ask when they can come in to get their shot. But the clinic has barely any doses to give out. Christi Siedlecki, the CEO of the clinic, has tried to get them. She registered her clinic’s interest in providing vaccinations with the state, and the state told her she was approved. But still: no vaccine. She asked the local health department for some doses. They gave her 30. “Obviously, that won’t get us far, but at least it’s something,” she told me recently. The only reason she’s getting them, she suspects, is because of “all the begging and bugging I do every day.” Most primary-care doctors haven’t received doses of the COVID-19 vaccine to dispense to their patients, according to two different trade groups for small-practice doctors. (Federally Qualified Health Centers, which get federal funding to provide care in underserved areas, have had better luck, and are part of the Biden administration’s vaccination plan.) Like Siedlecki, many primary-care doctors are begging their local and state health departments for doses, but mostly without success. Primary-care doctors see themselves as ideal foot soldiers in the battle to vaccinate America. After all, they know the extent of their patients’ preexisting conditions, are accustomed to soothing fears about vaccines, and can reach elderly patients quickly for an appointment. In Pennsylvania, a family doctor named Kevin Wong told me he has a 100-year-old patient who won’t leave his house. If he had the vaccine, Wong would be willing to make a house call. That would be a smoother experience than the one many seniors have had as they’ve sought vaccination in recent weeks. Some people are walking into their local health department to ask for the vaccine, only to be turned away and told to call an overwhelmed phone line. “I have been calling my doctor, my hospital, my insurance, and the Health Department since the beginning of December to get a COVID-19 vaccination,” a Floridian named William Klein wrote to his local paper. “No one had any information.” A 75-year-old named Betty told a Los Angeles Times reporter recently that though she would like to get the vaccine, “I have no idea where.” Another Florida man said he had to click 800 times to enter his date of birth on a cantankerous county website. “The most vulnerable populations, just like the ones that are most affected by COVID, are not necessarily the ones that are going to be able to scour the internet to find a place to go,” says Anders Gilberg, senior vice president at the Medical Group Management Association, which represents doctors in private practice. Many people already get their flu vaccine at their primary-care doctor’s office. So why not the COVID-19 vaccine? The reason, in short, is that there is simply not enough of the vaccine to go around. Seniors might be frustrated, but so are local and state health departments, governors, doctors, and pretty much everyone else I’ve called in the past week. They’re all saying the same thing: They wish they could get more doses of the vaccine—especially the Moderna version, which does not have to be kept at ultra-low temperatures. They also want it sent to them by the federal government on a more predictable schedule. The Biden administration might help with both of these problems, but so far, it has been a long and bitter month of waiting. “We desperately want to put vaccines in the hands of providers. But we can’t give them vaccines until we receive them,” says Michael Weber, who runs the health department in the county where Siedlecki’s clinic is located. Before last week, the health department had received a total of just 300 doses of the vaccine. Let’s back up to the halcyon days of December, when it was thought that there was a chance—a chance!—that vaccination would go smoothly. The first doses of the vaccine went mostly to hospitals, in part so they could vaccinate their own employees, and in part because hospitals had the ultra-cold storage the Pfizer vaccine requires. It’s also faster to deliver 100 doses of vaccine to one hospital than a few doses of vaccine to 100 doctor’s offices. In addition to hospitals, states sent the vaccine to county health departments because, the thinking was, health departments could get doses into arms quickly. Health departments “know how to do mass-vaccination clinics,” Marcus Plescia, the chief medical officer at the Association of State and Territorial Health Officials, says. They know how to set up a big tent with metal chairs and vaccinate hundreds of people within a few hours. Getting the vaccine to other types of doctors and pharmacies, as I heard over and over in recent days, is impossible until there’s more of it. This shortage of doses is why, in Palm Beach County, Florida, 100,000 seniors were on a waiting list recently for only 4,000 doses of vaccine. In Louisville, Kentucky, 40,000 people have signed up to wait for their dose. Walton County, Florida, opted against even maintaining a waiting list, because it was taking too long to call everyone back to schedule their appointment. These waiting lists might seem strange, given that states supposedly haven’t administered all of the vaccine they’ve been allocated. As of this writing, for example, North Dakota is performing the best, having used 74 percent of the doses it’s received. If states have extra vaccine sitting around, why not give it to Siedlecki or Wong or another doctor to give to some of those patiently waiting seniors? Because those doses, which exist but haven’t been used yet, “are spoken for—they’re gone,” Claire Hannan, executive director of the Association of Immunization Managers, told me. Some are in hospitals, and some are reserved for long-term-care facilities, where CVS and Walgreens are vaccinating residents as part of a federal program. It’s taking the pharmacy chains some time to get through these facilities, making it appear as though there’s a big pile of vaccines sitting there, just waiting to be injected. (Plescia thinks the distribution numbers aren’t accurate, and that state data systems might not be showing the latest immunization figures.) Those numbers look bad for states, which makes health directors less eager to send precious vaccines to a bunch of small-practice doctors, only to risk having more doses of vaccine sit around unused. When the Trump administration earlier this month urged states to begin vaccinating people older than 65 and those with underlying conditions, the public-health world erupted in quiet panic. The federal government hasn’t sent them enough vaccine to cover everyone over 65, and some states haven’t yet finished vaccinating health-care workers—the first-priority group. Health directors are saying that deliveries of the vaccine have been small and unreliable. The problem, they say again, is the supply. Both Moderna and Pfizer are trying to increase vaccine production, according to a White House coronavirus adviser who would only speak to me on the condition of anonymity. But because the technology to make the vaccine is so specific, it doesn’t make sense for the government to build a new factory for manufacturing it, the adviser said. In the time it would take to build a new facility to make the vaccine, the companies could expand their own production lines—something they’re already doing. The best hope for quickly expanding vaccine supply lies with Johnson & Johnson’s vaccine, which should be ready soon. The Biden administration might use the Defense Production Act to increase the production of medical supplies like syringes and needles that health workers need to administer the vaccine. It also plans to treat the pandemic like a natural disaster, giving states money and operational support through FEMA to help get vaccines into arms. But even if the new administration achieves that, it might not make vaccination angst-free for at least a few more months. Hannan, with the Association of Immunization Managers, predicts that it might be April or May before people will be able to receive the COVID-19 vaccine in the comfort of their doctor’s office. The White House adviser I interviewed said it might be even later on, after the country has already reached herd immunity. But eventually, the vaccine will have to flow through doctors’ offices. Doctors are, after all, still the core of American health care. Some seniors are willing to battle through an 800-click website to get themselves immunized, but not everyone is. As Shawn Martin, CEO of the American Academy of Family Physicians, told me, if primary-care doctors aren’t eventually able to administer the vaccine, “I don’t think we’ll ever vaccinate 300 million people.” from https://ift.tt/3r11Phb Check out http://natthash.tumblr.com Today marks two weeks of declining COVID-19 hospitalizations in the U.S., 14 straight days without a blip upward, according to data from the COVID Tracking Project at The Atlantic. Case numbers, too, are declining, and today the seven-day case average is down a third since its peak, on January 12. That day, the count of current hospitalizations was 131,326; it’s now down to 108,957. It’s the first significant decline since September 21, when the climb down from the summer surge stopped just under 29,000. As the country passes the milestone of 25 million cases, it’s a stable indicator pointing in the right direction. During the winter surge, hospitalization numbers bumped over a number of small, false summits, in which hospitalizations declined for a day or two before continuing their rise. They also rose for a couple of days after coming down from January 6’s absolute peak of 132,474. But two weeks of decline indicate that fewer people are getting sick. An average hospital stay as of November for patients with COVID-19 was 4.6 days, down from 10.5 days in March, so if hospital numbers are down it means that people are leaving the hospital without new patients replacing them. And the typical course from symptom onset to death is roughly two weeks. Accounting for the lag in deaths reporting, this substantial decline should start showing up in the daily deaths figure, which has plateaued in recent days and is a mixed picture nationwide. Falling hospitalizations are also occurring across the U.S. By the COVID Tracking Project’s conservative definitions, they’re falling week over week in 36 states and D.C., staying the same in 12, and rising in just three. In two of those states, Vermont and Hawaii, the rise is in double digits, 15 patients in the former and 27 in the latter. The increase in Kansas is greater in raw numbers—an additional 109 patients in the past week—but its hospitalization rate of 243 per million is in the middle of the pack. Among the encouraging news is that California is one of the states in the “falling” category. On January 7, the state peaked at 22,851 hospitalizations. Today it’s at 18,309, a 20 percent decrease in a little less than three weeks—although intensive-care units in Southern California and the San Fernando Valley remain full. California is large enough that changes there translate into changes in national numbers: That decline of 4,542 patients represents 19 percent of the nationwide decline in that period. Hospitalizations across the Northeast, though declining, have dropped just 11 percent in the past two weeks, the smallest decrease in any region. This indicates a point of concern: New York. It’s one of eight states with a hospitalization rate over 400 per million, and unlike the others, its recent hospitalization trajectory doesn’t yet suggest a peak. Two weeks ago, 8,926 people were hospitalized in New York. Today it’s 8,831. And the trends where the worst of the pandemic began, New York City, represent the bulk of the problem. Hospitalizations in the city are currently 3,730, up from 3,318 two weeks ago. There are 1,593 people hospitalized on Long Island, compared with 1,629 on the 12th. In the Mid-Hudson region, north of the city, hospitalizations are at 1,071, compared with 1,044 on the 12th. All these totals are far lower than the region’s spring surge, but they’re considerably higher than the summer and fall numbers, and stagnant hospitalization numbers in the region mean a lot of serious cases. The overall trend is encouraging, but there are significant unknowns. Restrictions are being lifted in many places across the country: California and New York, Chicago and elsewhere in Cook County, Boston. The more infectious and potentially more deadly B.1.1.7 variant has been found in 24 states, though in small numbers. Almost 20 million people have received at least one vaccine dose, as the Biden administration plans to push the number of daily doses given from 1 million to 1.5 million. How all of these factors will interact is impossible to predict, an uncertainty that provides reason for ongoing caution. But for now, the momentum is headed in the right direction: fewer hospitalizations, more vaccines. from https://ift.tt/3iM8Z60 Check out http://natthash.tumblr.com |
Authorhttp://natthash.tumblr.com Archives
April 2023
Categories |
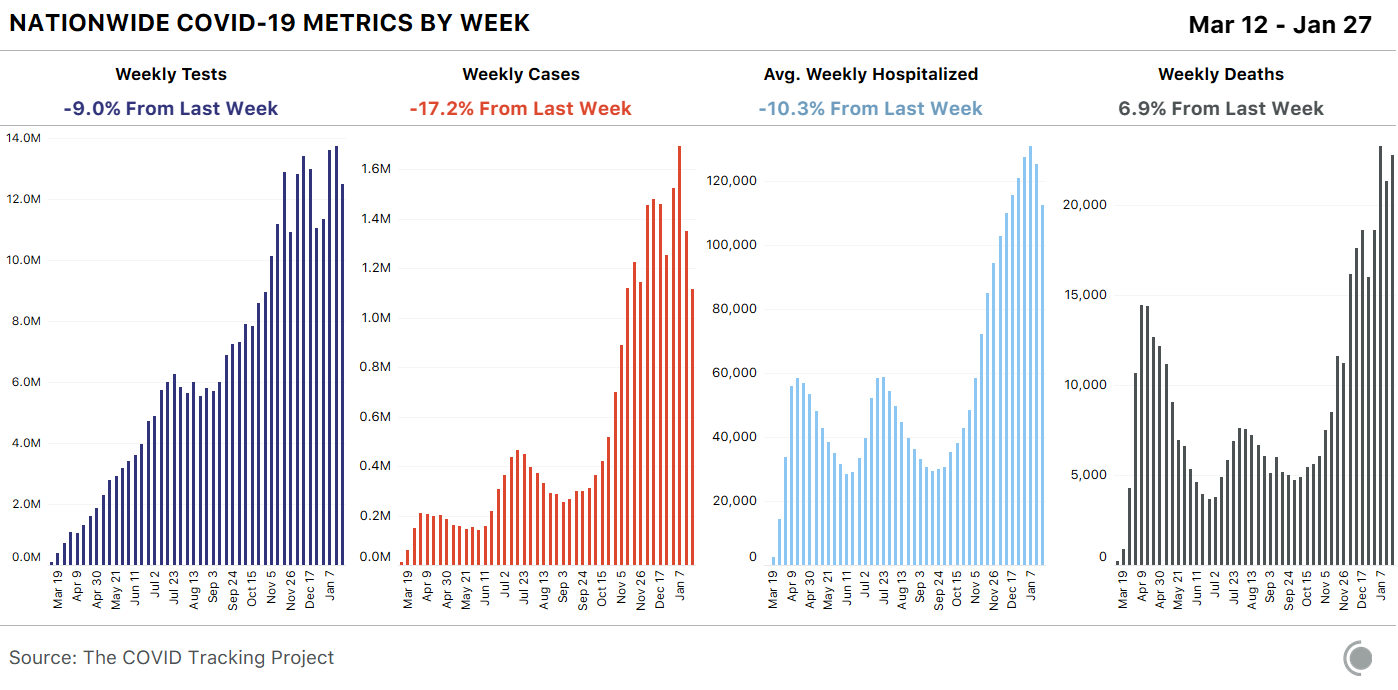
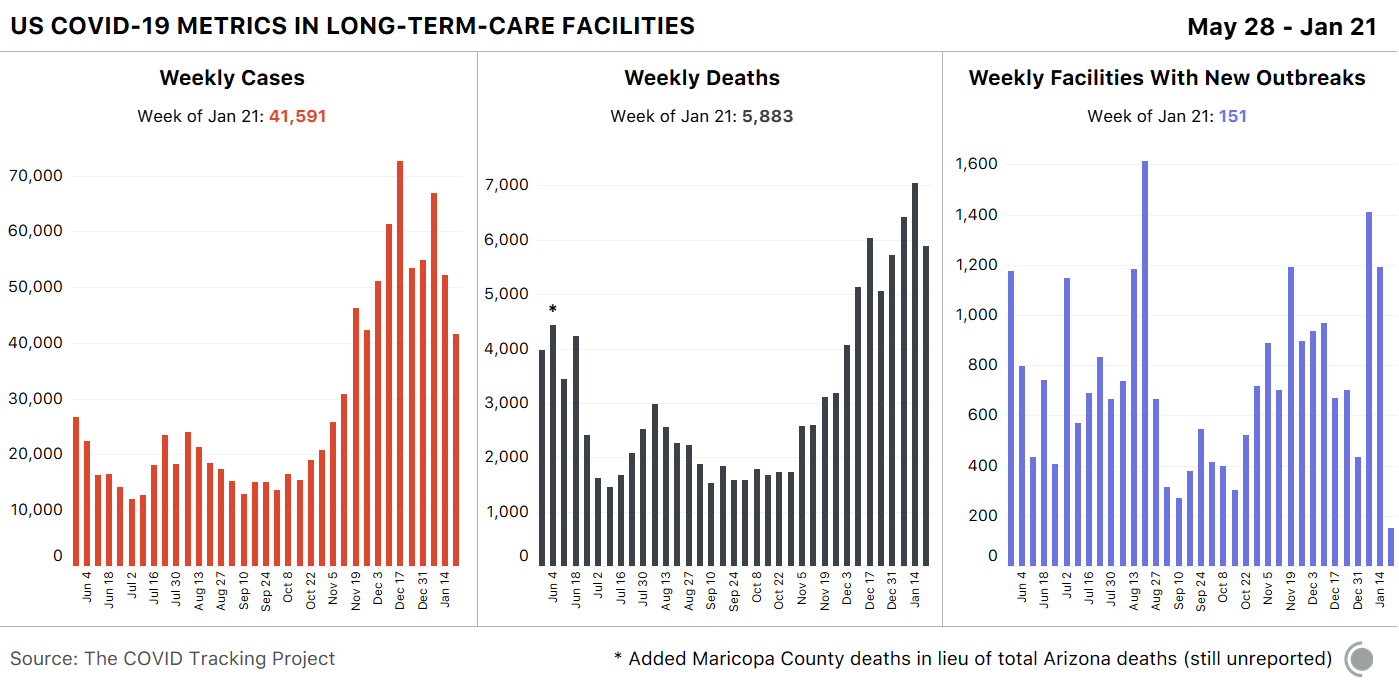
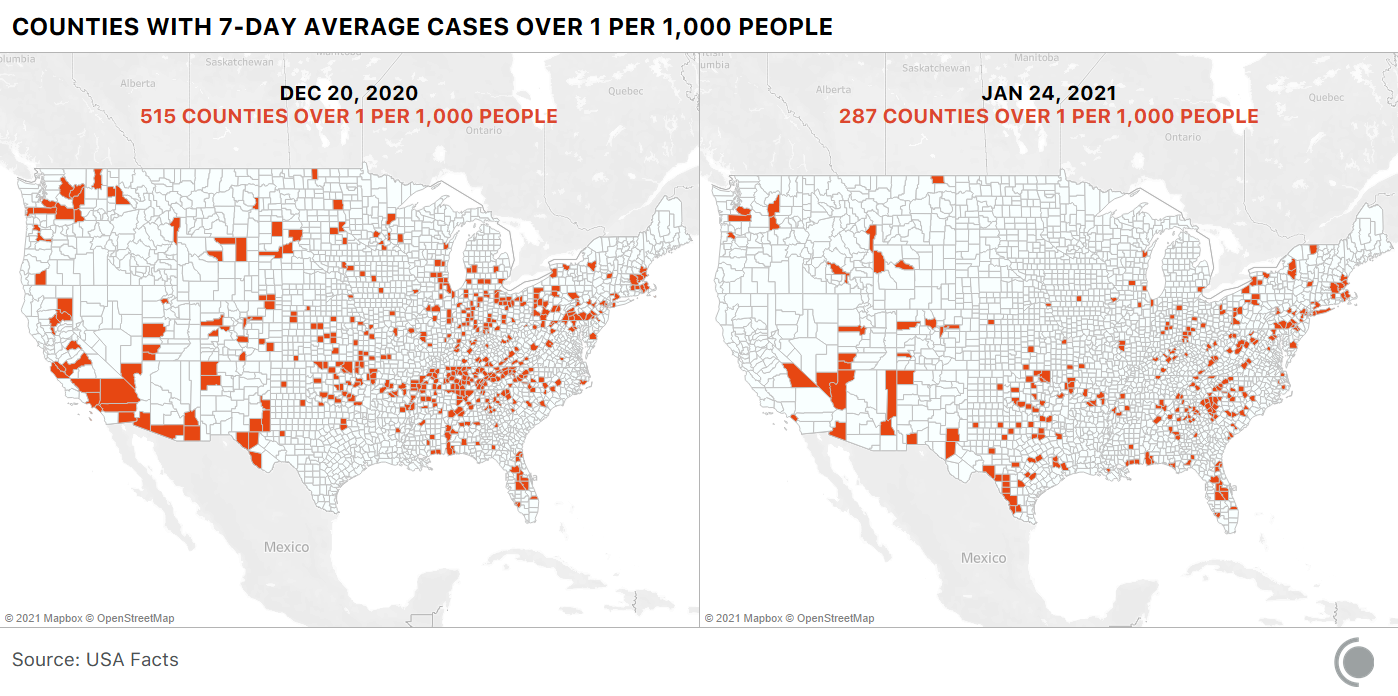
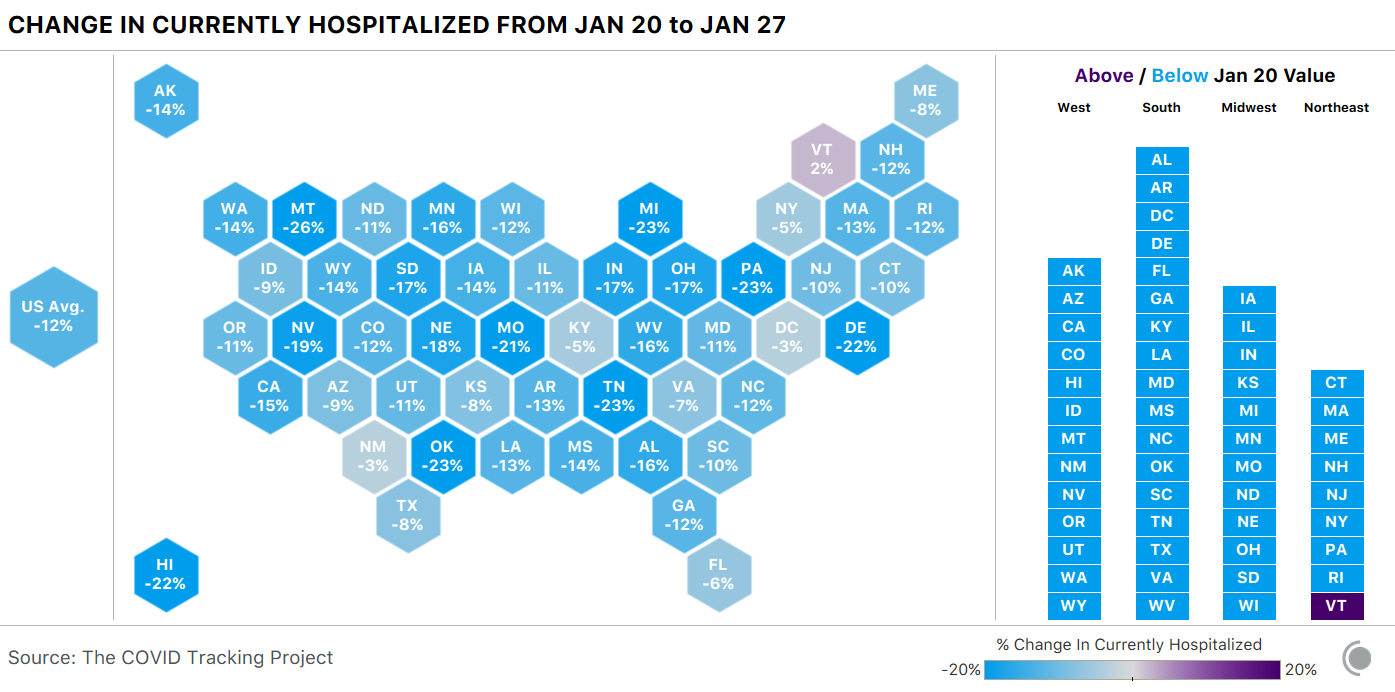
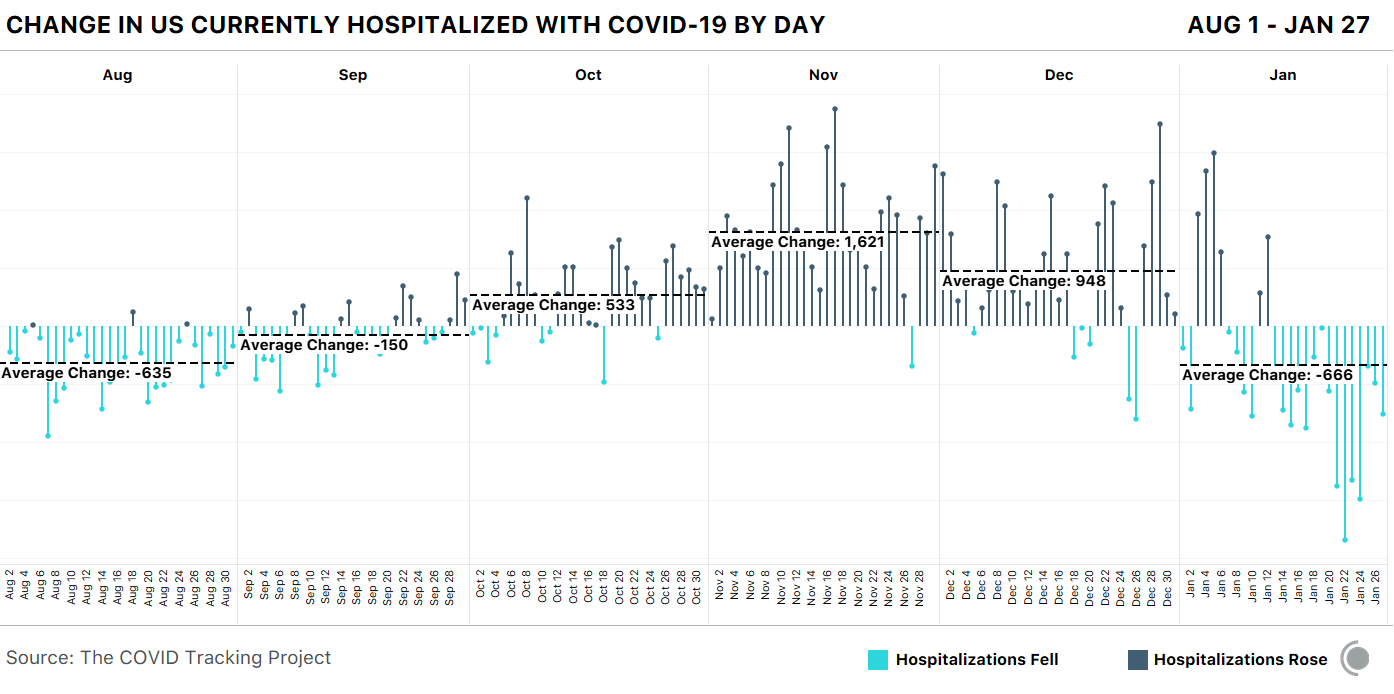
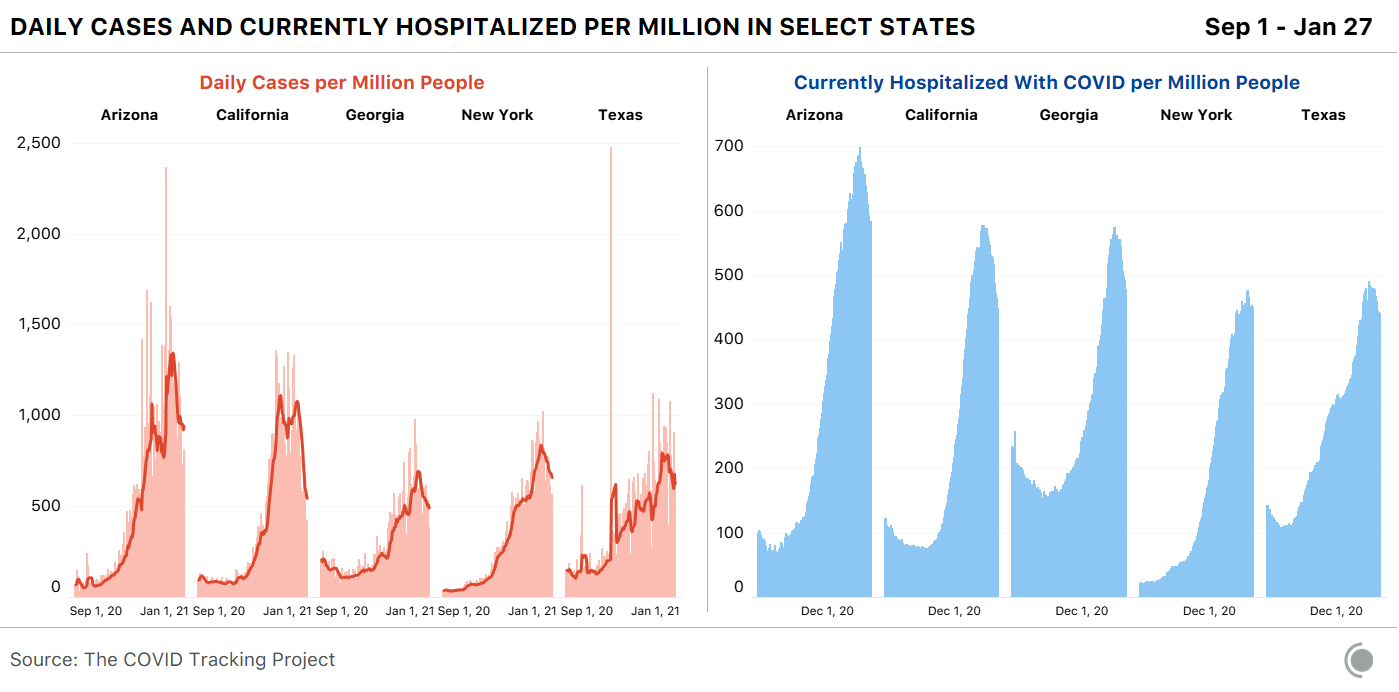


 RSS Feed
RSS Feed
