|
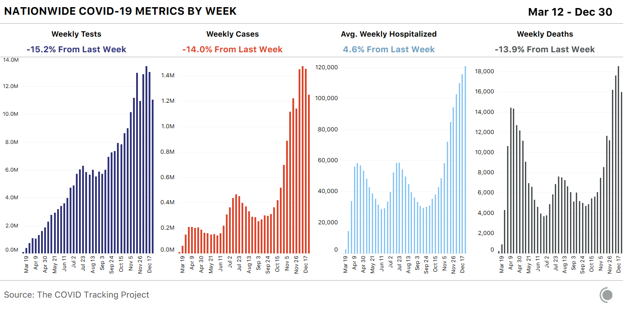
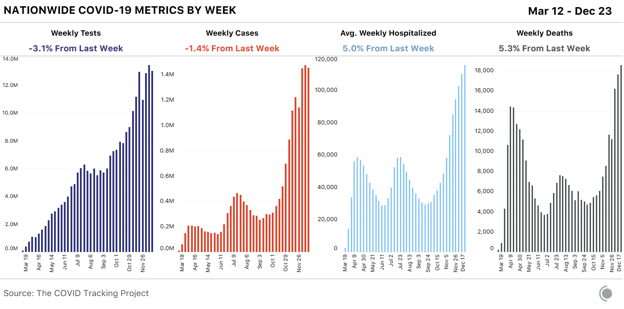
Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. On weekends, some of the people in labs, health departments, hospitals, and medical examiner’s offices who do the work of translating individual illnesses and deaths into data points get to go home. On Sundays and Mondays, when weekend COVID-19 data are reported, we see drops in most of the metrics we compile from states, then higher numbers during the rest of the week. Major US holidays act like super-size weekends: For most metrics, we see big drops followed by equally big spikes—neither of which are likely to be accurate measures of what’s actually happening across the country. Since Christmas, reported cases, tests, and deaths have all declined sharply. Cases and deaths are once again rising, but given that the New Year’s holiday weekend will also cause data disruptions, we aren’t expecting a return to normal reporting until closer to the middle of January.
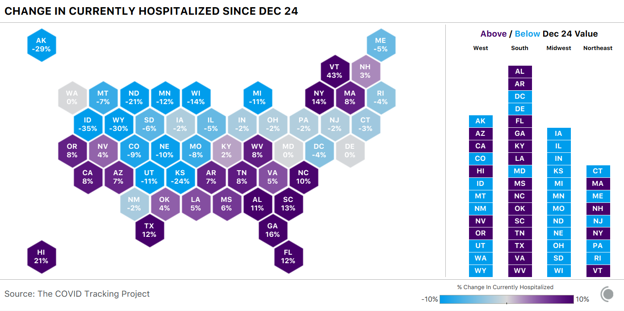
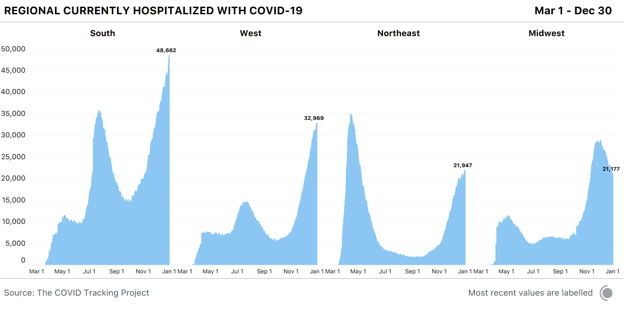
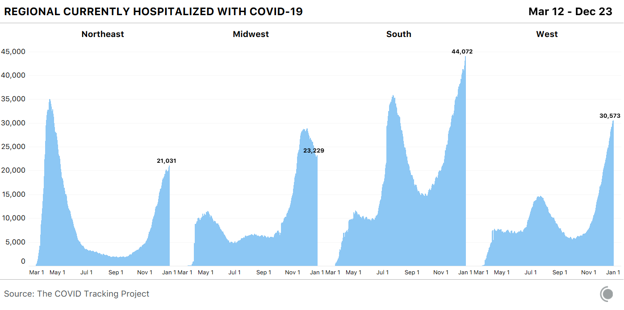
Of our four top-line metrics, only hospitalization counts remain relatively stable through holiday data disruptions. There’s no responsible way to interpret the other major metrics until holiday backlogs have come and gone, so for this final update of the year, we’re focusing on hospitalizations, which show only mild and transient holiday reporting artifacts. Across US regions, we see sharply differing hospitalization figures. COVID-19 hospitalizations continue to drop across the entire Midwest. In the West, hospitalizations have been declining across the Mountain West since December 24, but rising down the Pacific Coast and in the Southwest. We see a similarly mixed picture in the Northeast, where five states reported small declines in hospitalizations, and four—including New York—reported increases. Hospitalization increases across the South suggest that many southern states are experiencing worsening outbreaks: Fourteen of the 17 states in the region reported more people hospitalized with COVID-19 today than one week ago.
The country’s four most populous states--California, Florida, New York, and Texas—all saw COVID-19 hospitalizations rise in the past seven days. The increases we’re seeing in high-population states have a much greater effect on national numbers than do declines in low-population states. These week-over-week changes tell only part of the story, however—a 10 percent rise in an area where hospitalizations are low produces a smaller strain on health-care systems than a 10 percent rise in an area where hospitalizations are already very high. In absolute numbers, the South has by far the highest COVID-19 hospitalizations of any region, accounting for almost half the country’s total—but the South is home to more than twice as many people as the Northeast and nearly twice as many as the Midwest.
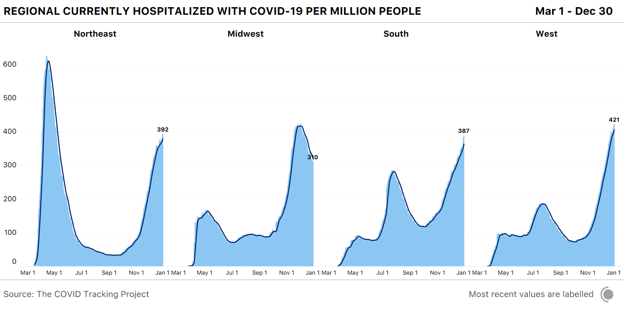
A view that adjusts for population allows us to understand the severity of each region’s overall situation. Driven by catastrophic hospitalization levels in Southern California, the West has reached 421 COVID-19 hospitalizations per million people, and closing in on the Midwest’s worst-ever per-capita hospitalization rate. The Northeast now has 392 people hospitalized with COVID-19 per million—more than either the Midwest (310 hospitalizations per million) or the South (387 hospitalizations per million).
As COVID-19 case and death numbers in the United States continue to oscillate between relatively low and startlingly high numbers because of holiday reporting slowdowns, we suggest that readers remain focused on the relatively stable hospitalization metrics—and on local guidance about how to have a safe and healthy New Year’s holiday. We’ll be back with another update next week as the data backlogs from Christmas and New Year’s Day continue to resolve. from https://ift.tt/3hwQ0vy Check out http://natthash.tumblr.com
0 Comments
As the pandemic enters its second year, the coronavirus has remade everyday life in the United States. More than 19 million Americans have been diagnosed with COVID-19 since March, and at least 330,000 Americans have died of it, according to the COVID Tracking Project at The Atlantic. Yesterday, 3,903 Americans were reported to have died of the virus, the highest death toll since the pandemic began. Yet the U.S. is still making the same two deadly mistakes that have defined its response since the pandemic began, our ongoing investigation has found. The nation still does not have enough tests to combat the pandemic. And it is still allowing the virus to rampage through nursing homes and other long-term-care facilities. [Read: Where year two of the pandemic will take us] After an early failure in February left the country with growing caseloads and too few COVID-19 tests to track the outbreak, the U.S. has never caught up. By the middle of December, the country tested about 1.8 million people a day for the virus, which was close to an all-time high. But to begin fighting the virus through testing—by, for instance, identifying infected people before they pass the virus to others—the U.S. must test at least 4.4 million people a day, according to the Harvard Global Health Institute. Ideally, given the scale of the pandemic, the country would run 14 million tests a day, the institute posits. By our count, the U.S. has conducted more than 248 million tests since the pandemic began, a staggering total. But the virus is now so widespread that if America were meeting that ideal testing target, it would run about that many tests every two and a half weeks. 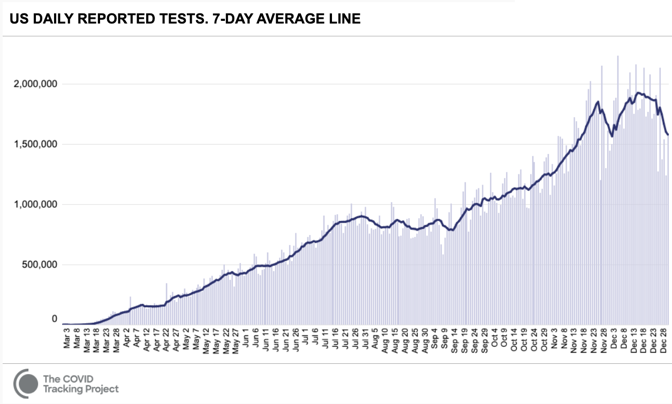
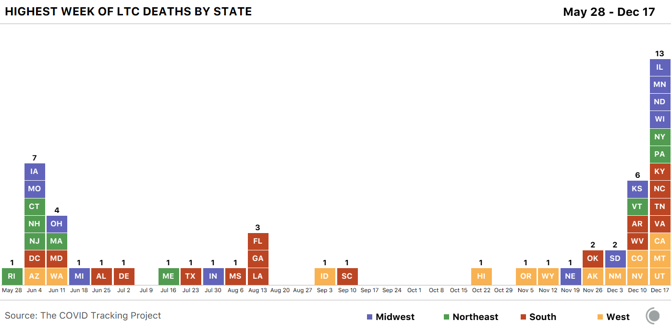
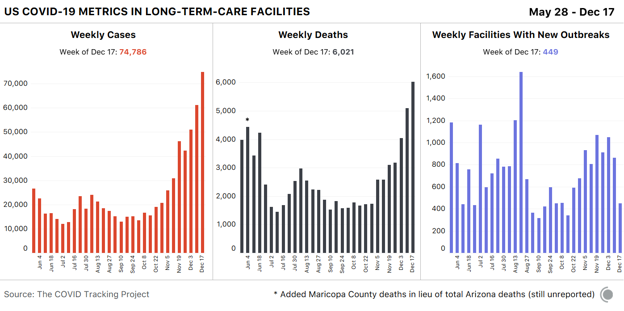
The U.S. has never tested as many people as it needs to in order to keep the pandemic in check. It has gone weeks at a time—from late July to mid-September, most strikingly—without increasing the number of people tested every day. At moments when infection has been especially widespread, companies have taken days or even weeks to process test results. Federal regulators have been slow to approve rapid virus tests that could be used at home without a prescription, similar to pregnancy tests. This has compounded a second crucial failure. In the spring, the country learned that the virus is deadliest in long-term-care facilities such as nursing homes. Though these facilities house less than 1 percent of America’s population, they have seen at least 38 percent of the nation’s COVID-19 deaths, our data show. (Some states report incomplete data for these facilities, meaning that this number likely undercounts the true toll originating in these settings.) The Trump administration has claimed that saving lives at such facilities is core to its pandemic strategy. Scott Atlas, a neuroradiologist who advised Donald Trump on virus policy for much of the summer and fall, argued that there was little risk in allowing the virus to spread through the general population as long as officials focused on “protection of the vulnerable” in nursing homes. [Read: The last days of loneliness] Yet the country has never succeeded at protecting the vulnerable, our data show. In December alone, at least 20,455 people have died in long-term-care facilities and nursing homes, the greatest toll since the COVID Tracking Project began collecting long-term-care data in late May. And in every region of the country but the Northeast, more people died in long-term-care facilities in the summer and fall than in the spring. 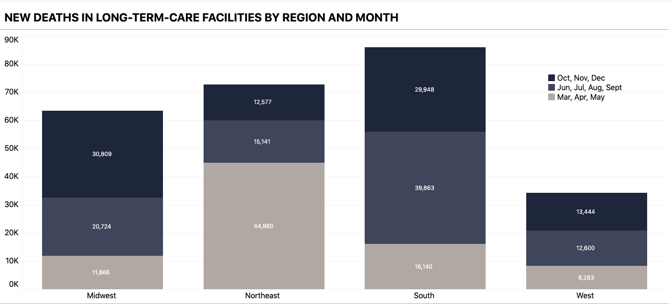
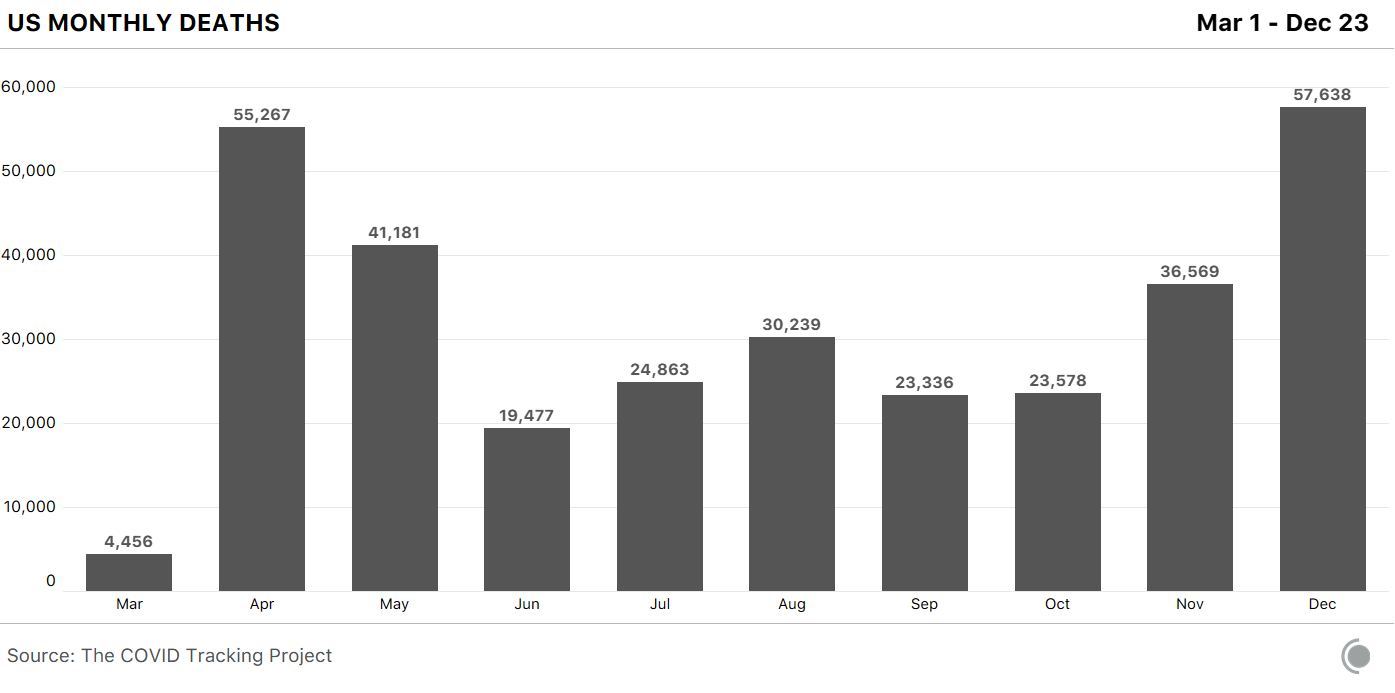
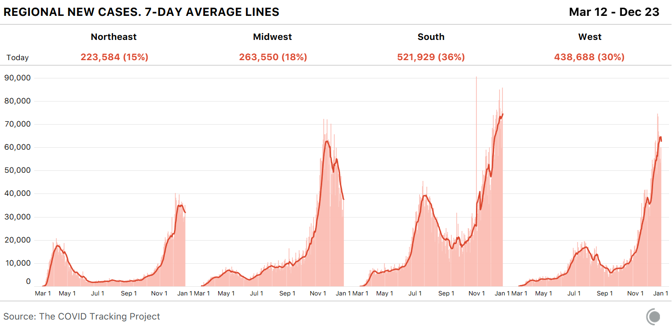
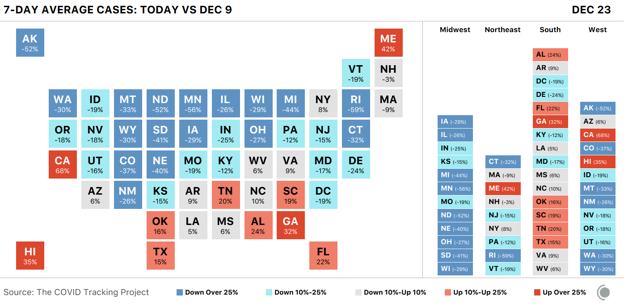
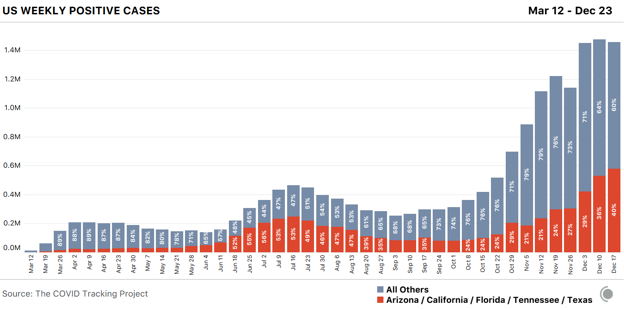
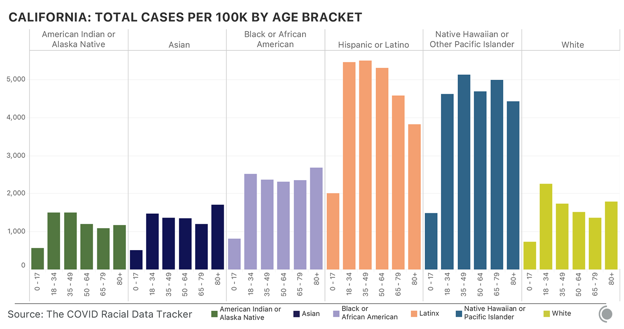
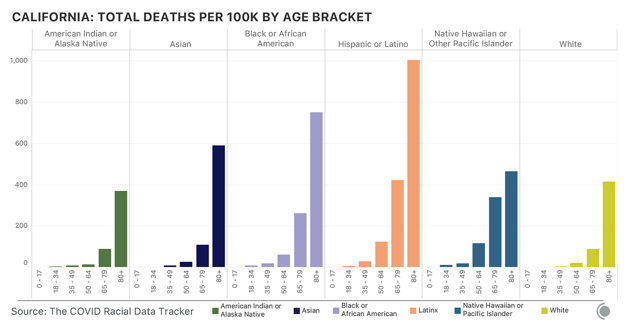
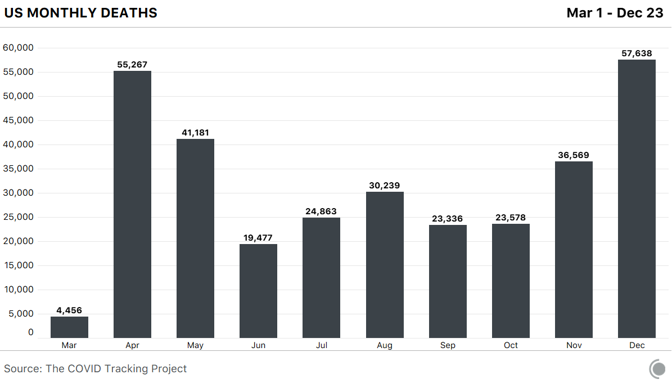
These two debacles have preyed on the effectiveness of the American pandemic response from the start. At the end of the year, the U.S. has more diagnosed COVID-19 cases than any other country, and it ranks fourth worldwide in COVID-19 deaths per capita. And December has been the deadliest month of the pandemic so far, our data show. Its death toll has exceeded that of April by 29 percent. These data were collected by the COVID Tracking Project at The Atlantic. For each of the past 299 days, a team of volunteers and project members has watched press conferences, tracked social-media posts, and combed through dozens of government websites to compile the COVID-19 data that each U.S. state and territory provides. The project now records nearly 800 individual statistics. The resulting database is a patchwork, built from the individual components that each state’s data systems capture and from the numbers that local political leaders allow to be published. Fusing together 56 state and territorial data sets can be a fraught, complex process, and the project publishes exhaustive documentation of what the numbers mean, how they compare to one another, and what we still don’t know, because of the variability of state reporting. One of the most obvious elisions is the toll that the pandemic has taken on Black, Latino, and Indigenous people. The pandemic has disproportionately killed people in these communities, our data show. At least one in every 800 Black Americans has died of COVID-19, and Black people have died of COVID-19 at 1.7 times the rate of white people. Nationwide, Indigenous people and Alaska Natives have died of COVID-19 at 1.4 times the rate of white people. [Read: The virus is showing Black people what they knew all along] Yet the full scale of this damage is not quantifiable, because many states still do not track enough data by race and ethnicity for us to identify the full, disparate impact. Texas, for instance, reports race and ethnicity data for only 4 percent of cases. New York has never reported race and ethnicity data, which obscures our understanding of the first surge in particular, when New York’s numbers dominated every national statistic. Only seven states report the racial breakdown of testing data, an important tool in detecting how large outbreaks are overall, because knowing the fraction of a population that has been tested can indicate the breadth of the virus’s spread. Because of such inconsistencies and gaps, the COVID Tracking Project team has also communicated with state and federal officials hundreds of times over the past 10 months to clarify the meaning of specific numbers and to push for higher data quality and more public transparency. This effort meant that, for months, the COVID Tracking Project published the only public database of testing and hospitalization data. Today, it is the only data set detailing each state’s and territory’s daily case, testing, hospitalization, and death numbers since the pandemic began. The federal government, including the White House Coronavirus Task Force, has used data from our investigation because it has had no alternative. The CDC Advisory Committee on Immunization Practices has repeatedly cited our data on long-term-care facilities in the course of deciding that residents of those places should get vaccinated first. [Read: What the vaccine’s side effects feel like] Today, the federal government publishes data on many of the same metrics we began tracking in March. But for many of these metrics, our data remain the only independent check on that federal data. The COVID Tracking Project has repeatedly identified issues with the data shared at the state and federal level. For instance, in the spring the CDC made the state of the pandemic less clear by lumping together two different types of tests—antibody tests, which detect past infection, and diagnostic tests, which detect present illness. Test-positivity statistics, widely used to make decisions about pandemic restrictions, still show massive variability, we have found, which make them extremely difficult to use when setting interstate policy. Now the millions of inexpensive, rapid tests that the Trump administration purchased and directed to vulnerable populations are not being reported at either the state or federal level. Over the past 10 months, we have seen the federal government struggle to acquire, present, and analyze the data necessary to understand the pandemic. This could change in the coming weeks: The incoming Biden administration has said that it plans to make a National Pandemic Dashboard. What will matter, then, is not only having the data, but using them to save lives. from https://ift.tt/3nbqM7n Check out http://natthash.tumblr.com Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. Three weeks ago, the COVID-19 winter surge was well under way and terrifyingly broad. Every day, the Northeast, South, and Midwest were seeing more than 100 deaths per million people, and the West was just shy of that, at 94 per million, with deaths increasing. The winter surge was the first time conditions had worsened nationwide; previously, the spring saw cases concentrated largely in the Northeast, followed by a summer surge across the South and West. But by early October, all four regions, as defined by the census, saw climbing hospitalizations. Now, the pandemic’s geography is fracturing again. Hospitalizations in the Midwest peaked on December 1, and have maintained a precipitous decline ever since. Hospitalizations continue to rise in the Northeast, but they are still at about 60 percent of the spring’s awful totals. The hardest-hit areas right now, as indicated by hospitalizations per million residents, are in the South and Southwest. The hotspots are primarily in the Sun Belt, including California, Nevada, Mississippi, Alabama, Tennessee, and Georgia. New York is also a cause for concern again. In other words, we’re returning to a patchwork pandemic. Nationwide, the most stable indicator—the number of hospitalizations—is still rising, though not as quickly as it was from November through mid-December, thanks to declines in the Midwest. Focusing on hospitalizations is particularly useful right now because holidays, like weekends, depress the reporting of cases and deaths across the country, while sick people continue to enter the hospital as they would on any other day. So even though cases are down compared to last week in most states, with a similar trend in the seven-day average of daily deaths nationwide, that’s likely a data lag that won’t clear up until the first week or two of the new year. And hospitalizations tell a more complex story. Over the seven days ending December 29, the measure fell in 28 states and the District of Columbia and rose in 21 states (it was unchanged in New Mexico); it fell by 10 percent or more in 10 states, suggesting a substantial change in the state’s conditions, and rose by 10 percent or more in 12. [Read: California has lost control] California is one of the five states—along with Arizona, Florida, Tennessee, and Texas—that account for 40 percent of new cases from December 17 to December 23, according to the COVID Tracking Project. Of the five, California has by far the highest number of hospitalizations, which beyond their general stress on the health-care system augur high death tolls to come. California had 21,240 people in hospitals on December 29, accounting for 17 percent of all hospitalizations nationwide. Twice as many Californians were hospitalized on December 29 as on December 6. Texas is also seeing a rise in hospitalizations—it had 11,775 on December 29—but its numbers are only up by about 2,800 since the first week of December. Hospitalizations are also up in Arizona. Its hospitalization rate, at 615 people per million, is higher than California’s 538 per million. Arizona has now surpassed its devastating summer surge; while 3,517 people were hospitalized on July 14, that number was 4,475 on December 29. Nevada, whose population is centered in Las Vegas between the hotspots of Arizona and Southern California, has the highest hospitalization rate in the country, at 626 per million. [Read: America’s patchwork pandemic is fraying even further] Just behind Nevada and Arizona in hospitalizations per million is Alabama. During its summer surge in early August, Alabama had about 1,500 hospitalized COVID-19 patients per day; it now has 2,804. The state’s seven-day average of deaths (which, because of the problems with holiday reporting, is quite volatile) has also recently been higher than in the summer. On December 23, the state reported 135 deaths, more than double the peak of 61 it suffered on July 27, and reported another 89 deaths on December 24. Hospitalizations are also up in neighboring Georgia, which reached a new record of 4,839 on December 29, one-third higher than its previous July peak. In this patchwork, which includes clusters in the West and South, the country’s original epicenter is also back on the map. New York is nowhere near the dire conditions of the late winter and early spring, when the state had more than 18,000 people hospitalized and was recording more than 750 deaths per day, but there are worrisome signs. The seven-day average of hospitalizations more than doubled between December 1 and December 29, when it hit 7,184. Cases and deaths are also up. And unlike in the spring, the problem is statewide. According to New York State data, 2,717 people in New York City were hospitalized with COVID-19 on December 28, plus another 1,358 in Long Island. Those two regions are far below their spring peaks, as is the mid-Hudson region, which encompasses the area just north of the city, including its suburbs, while every other part of the state is at its highest level yet—there are more than 400 people hospitalized in the central New York area, for example, about five times higher than at any other point in the pandemic. There are 964 hospitalized in the Finger Lakes region, 4.4 times the previous peak. [Read: The terrible déjà vu of COVID-19’s winter surge] Nationwide, the picture is certainly better than it was at the beginning of December, or even a week or two ago. Conditions in the Midwest have improved substantially. They’ve actually improved in most states in the West, even if California, Nevada, and Arizona are driving the top-line numbers up. The situation in the South and Northeast is mixed—some, but not all, states are struggling, and there’s a hint that the increase in hospitalizations in both regions could be slowing. Still, the U.S. is far from out of the woods, and the murkiness of the data that will stretch into the first few days of 2021 makes it harder to see the path through it. The improvements in some places are real, especially in the Midwest, as hospitalizations indicate. In other places, falling case and death counts are just as likely to be the result of reporting lags. Even if the worst of the winter surge is, in fact, receding, the lack of clarity that could result from America’s new patchwork risks further confusion, complacency, and disjointed responses. With widespread vaccine access on the horizon, the end really is in sight, but a false dawn could lead to even more misery. from https://ift.tt/2WYTTzQ Check out http://natthash.tumblr.com Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. The influenza pandemic that began in 1918 killed as many as 100 million people over two years. It was one of the deadliest disasters in history, and the one all subsequent pandemics are now compared with. At the time, The Atlantic did not cover it. In the immediate aftermath, “it really disappeared from the public consciousness,” says Scott Knowles, a disaster historian at Drexel University. “It was swamped by World War I and then the Great Depression. All of that got crushed into one era.” An immense crisis can be lost amid the rush of history, and Knowles wonders if the fracturing of democratic norms or the economic woes that COVID-19 set off might not subsume the current pandemic. “I think we’re in this liminal moment of collectively deciding what we’re going to remember and what we’re going to forget,” says Martha Lincoln, a medical anthropologist at San Francisco State University. The coronavirus pandemic ignited at the end of 2019 and blazed across 2020. Many countries repeatedly contained it. The United States did not. At least 19 million Americans have been infected. At least 326,000 have died. The first two surges, in the spring and summer, plateaued but never significantly subsided. The third and worst is still ongoing. In December, an average of 2,379 Americans have died every day of COVID-19—comparable to the 2,403 who died in Pearl Harbor and the 2,977 who died in the 9/11 attacks. The virus now has so much momentum that more infection and death are inevitable as the second full year of the pandemic begins. “There will be a whole lot of pain in the first quarter” of 2021, Anthony Fauci, the director of the National Institute of Allergy and Infectious Diseases, told me. [Read: Hospitals know what’s coming] But that pain could soon start to recede. Two vaccines have been developed and approved in less time than many experts predicted, and are more effective than they dared hope. Joe Biden, the incoming president, has promised to push for measures that health specialists have championed in vain for months. He has filled his administration and COVID-19 task force with seasoned scientists and medics. His chief of staff, Ron Klain, coordinated America’s response to the Ebola outbreak of 2014. His pick for CDC director, Rochelle Walensky, is a widely respected infectious-disease doctor and skilled communicator. The winter months will still be abyssally dark, but every day promises to bring a little more light. On the Fourth of July, Ashish Jha wants to host a barbecue at his house in Newtown, Massachusetts. By then, the state expects to have rolled out COVID-19 vaccines to anyone who wants one. The process will be bumpy, but Jha is hopeful. He thinks that the SARS-CoV-2 coronavirus will still be spreading within the U.S., but at a simmer rather than this winter’s calamitous boil. He expects to keep all his guests outside, where the risk of transmission is substantially lower. If it starts raining, they could come indoors after putting on masks. “It won’t be normal, but it won’t be like Fourth of July 2020,” says Jha, the dean of the Brown University School of Public Health. “I think that’s when it’ll start to feel like we’re no longer in a pandemic.” Many of the 30 epidemiologists, physicians, immunologists, sociologists, and historians whom I interviewed for this piece are cautiously optimistic that the U.S. is headed for a better summer. But they emphasized that such a world, though plausible, is not inevitable. Its realization hinges on successfully executing the most complicated vaccination program in U.S. history, on persuading a frayed and fractured nation to continue using masks and avoiding indoor crowds, on countering the growing quagmire of misinformation, and on successfully monitoring and countering changes in the virus itself. “Think about next summer as a marker for when we might be able to breathe again,” said Loyce Pace, the executive director of a nonprofit called the Global Health Council and a member of Biden’s COVID-19 task force. “But there’s almost a year’s worth of work that needs to happen in those six months.” The pandemic will end not with a declaration, but with a long, protracted exhalation. Even if everything goes according to plan, which is a significant if, the horrors of 2020 will leave lasting legacies. A pummeled health-care system will be reeling, short-staffed, and facing new surges of people with long-haul symptoms or mental-health problems. Social gaps that were widened will be further torn apart. Grief will turn into trauma. And a nation that has begun to return to normal will have to decide whether to remember that normal led to this. “We’re trying to get through this with a vaccine without truly exploring our soul,” said Mike Osterholm, an epidemiologist at the University of Minnesota.
|
Authorhttp://natthash.tumblr.com Archives
April 2023
Categories |

 RSS Feed
RSS Feed
