|
Professional runners have to endure extraordinary deprivation, pain, and pressure to reach the Olympics. Professional-running fans, meanwhile, have to endure the question of which athletes actually deserve to be there. This summer, before the U.S. trials for the Tokyo Olympics had even finished, fans were forced to digest the fact that two of America’s track-and-field athletes most likely to medal wouldn’t be headed to the Games. Not because they’d lost to better athletes, but because they’d been caught in the snare of the anti-doping system, for better or worse. Many would say for worse. One of the cases is fairly cut-and-dried. The sprinter Sha’Carri Richardson ingested marijuana after getting the news that her biological mother had died. Although sentiments in the United States about marijuana have shifted considerably, and the idea of THC being performance-enhancing for her particular discipline is spurious at best, the drug is clearly banned during competition. Richardson admitted fault and accepted her penalty. The other case is much more complicated. The distance runner Shelby Houlihan tested positive for the anabolic steroid nandrolone, a drug that can increase muscle strength and red-blood-cell count. She claims that she inadvertently ingested the drug from a burrito. This might seem absurd, but as testing protocols have become more and more sensitive—now reliably measuring down to the level of a picogram, which is one-trillionth of a gram—meat has been shown to cause the odd failed drug test. Travis Tygart, the CEO of the United States Anti-Doping Agency, who did not handle the Houlihan case, told me that the agency has handled, on average, one of these cases a year, with most of the athletes getting off with what is called a no-fault violation. Controversies and complications involving banned substances are really just the tip of the iceberg of track spectators’ woes. Professional running is caught in the middle of a bona fide fairness crisis. Athletes’ performances are shaped by a dizzying array of factors, both legal and illegal, that have little to do with tradition or any supposed values of equal competition. The result, for anyone who actually wants to enjoy these races, is brain-scrambling. This is not to say that being a sports fan hasn’t always been a fraught enterprise. The ancient Olympians, who were all men, competed in the nude; any woman caught in the Olympic Festival was punished by getting thrown to her death from a cliff. A reported 96.4 million viewers tuned in to the 2021 Super Bowl, despite what football does to young men’s brains. The closer you look at your favorite sport, the more likely you are to find impediments to pure, unadulterated fandom. And as the modern Olympiad’s competitions continue this week in Tokyo, running fans in particular are grappling with an ever-growing set of conflicts. For journalists, like myself, who love running, trying to make any sense of these conflicts is all but impossible. I’ve spent much of my career exploring the unsavory corners of professional endurance sports, and everything I’ve learned has inevitably proved more complicated and nuanced than I could have imagined. We have to live with the knowledge, for example, that the world-champion sprinter Justin Gatlin’s first doping offense was caused by a substance he had been prescribed since childhood for his attention deficit disorder. But before you get too comfortable with the idea that he’s a clean athlete done wrong, remember that five years later, he failed a doping test for testosterone, and claimed that he’d been sabotaged by his massage therapist. (Gatlin was banned from sport for four years and continues to claim his innocence.) The line of dubious claims by athletes who have been caught cheating is long: My twin died in the womb, and that’s why I have someone else’s blood cells in me; I kissed (or made love to) someone who did the drugs; someone spiked my beer with steroids; I drank too much whiskey last night, and it boosted my testosterone; there must have been strychnine in my pigeon pie. Even if we put aside the specter of performance-enhancing drugs in running, issues of fairness exist with funding, access to training facilities, and now, equipment. Some Nike-sponsored athletes who dominated the podium at the last Olympics wore shoes that were technically illegal because they hadn’t been widely available to the public prior to the race, as World Athletics rules stipulate they should be. Nike went so far as to apparently color its road-running shoes to look like a different model in an effort to hide them from authorities. It worked. By the time lab tests proved that the shoes bestow a 4 percent efficiency benefit, on average, the races were over, and athletes who’d worn other shoes had no recourse. This issue has gotten only more fraught since then. As other brands race to catch up, Nike has built track shoes with similar technology that have already begun rewriting the record books. The beauty of a running race, whether on a playground or in an Olympic stadium, is that it’s primal, basic, and easy to comprehend. And the lack of affecting technology has meant, historically, that you can compare current times to those of past generations. But now, professional running has reached a place of dissonance so deep that it’s overpowering. When an athlete achieves a new record or wins a gold medal, fans are now plagued with insuperable questions. Is that person doped? Did their shoes make the difference? How many performance-enhancing prescription drugs are they on that they don’t actually need? It’s that last one that I found so insidious during my reporting. When drug-testing advancements made doping with illicit substances harder to hide in the wake of the Lance Armstrong era, teams began employing doctors to prescribe substances that their athlete patients might not need medically, but that sure did help with oxygen transport, energy levels, recovery, and weight loss. This immense gray area remains untouched by the anti-doping agencies. Even so—and I’m shaking my head as I write this—I can’t turn away. There is something so naturally dramatic about a footrace. The Olympics are an opportunity for athletes in a sport such as running, which Americans mostly forget about in the years between the Games, to completely change their lives by performing on the world’s biggest stage. The years of sacrifice and toil on display are genuinely breathtaking. And the excitement I feel when witnessing this is real, regardless of how mad it makes me. For now, it’s enough--just enough—for me to keep enduring the pain of being a fan. from https://ift.tt/3yacgTv Check out http://natthash.tumblr.com
0 Comments
The CDC’s color-coded coronavirus case map, if you can find it, is easy enough to read. It’s a county-by-county snapshot of viral transmission—the agency’s new fallback for advising fully vaccinated people on whether they need to don a mask indoors. The parts painted in those scary shades of orange or red are areas of substantial or high transmission, respectively; they’re the places where you should be shielding your face indoors, regardless of how shot-fortified your immune system is. According to the agency, not everyone has to mask up again, so the map is, in theory, something inoculated Americans could check like a weather forecast to decide their face’s fate. Use the map, CDC Director Rochelle Walensky advised in a press briefing this week. It’s updated daily. Today, the CDC is expected to publish data, leaked last night and reported by The Washington Post, hinting at the increased dangers of the Delta variant—a version of the coronavirus that can accumulate in high amounts in the airways of even fully vaccinated people, potentially poising them to spread it to others around them. And while Delta is still less likely to set up shop in someone who’s been immunized, it might be better equipped than other variants to cause severe symptoms when it does. Delta is clearly a far more formidable foe than its predecessors, which makes a map like this seem an even more necessary tool.
But this check the weather forecast strategy belies the full national pandemic portrait: Nearly half of Americans are still unvaccinated, and the super-contagious Delta variant is flooding every corner of the country. The CDC’s internal document suggests that Delta could be as contagious as the chickenpox virus, a transmissibility trait that potentially outstrips that of other known human coronaviruses, including the original SARS virus, and flu viruses (though statements like this are very difficult to confirm without more data). Vaccinated people, in other words, pose more of a threat to those around them than the CDC had hoped in May, when it said they could shed their masks in most situations. That’s why that same document explicitly called for universal masking to halt Delta’s rampage, The Washington Post reported. In public, however, the agency’s call for map-based masking sends a different message. During a time of public crisis, when so many are looking for guidance from a central authority, the CDC punted decision making to local governments and individuals. “We’re clearly not thinking bigger picture,” Krutika Kuppalli, an infectious-disease physician at the Medical University of South Carolina, told me. (The CDC did not respond to repeated requests for comment.) I spoke with several researchers who agree: Masking up again is warranted, and the CDC’s map is well intended, even useful for some purposes. But as a personal risk-assessment tool, it’s frustrating and confusing—and symbolizes how muddled the messaging on masking while vaccinated has become. Once again, people are being asked to take a “choose your own adventure” approach to public health. With Delta cases rising quickly, we might choose, without the best of intentions, to dig our collective COVID hole deeper. The map itself, after weeks of pulsing in a nearly uniform shade of comforting blue, now highlights in fiery hues how dire the nationwide situation has become. Case rates will inevitably vary geographically; they’ve risen, quite reliably, in places where vaccination rates are low. “There is legitimately higher risk in some places than others,” Whitney Robinson, an epidemiologist at UNC’s Gillings School of Global Public Health, told me. The map does ask people to consider the circumstances around them, which is a step in the right direction. But that sentiment might not go far enough. Neither viruses nor humans are easy to pen in with county lines; risk won’t obey those borders either. People who work and live in different counties with discordant transmission profiles might struggle to adjust; those in low-risk islands, swathed by seas of orange and red, might mask more laxly than they should. “Too often we only focus on the county we live in,” Saskia Popescu, an epidemiologist and infection-prevention expert at George Mason University, told me. “Consider where you work, the general state, and region.” The color-coding system, too, draws some false boundaries. To qualify for “substantial” transmission, a county must record 50 new coronavirus cases per 100,000 people within a seven-day period, or report that more than 8 percent of tests for the virus are positive in that same window. The “high” category kicks it up a notch: 100 new cases, or 10 percent test positivity. Those aren’t unreasonable cutoffs to set, experts told me, and cutoffs have to be set somewhere. But those thresholds still end up turning a spectrum into a binary--above 50 new cases is bad, below that is fine—and obscures when one county is on the verge of ascending to a higher-risk class. “What’s safe? What’s not? How you put a number on that is really hard,” Robinson said. Those numbers also change, frequently and without warning. They offer a glimpse into the past week, but don’t forecast the future, making them harder to parse than weather forecasts. (The way to get a yellow county to morph into an orange one is, of course, by allowing the virus to spread.) “At this point, I’m telling folks in most of the country to mask up indoors,” Megan Ranney, an emergency-medicine physician at Brown, told me. “If you’re not in high or substantial transmission today, you probably will be tomorrow or the next day, given the rate of spread of this Delta variant.” Several experts, including Kuppalli, think the CDC’s new masking guidance should have gone a step further, skipped the geographical contingencies, and asked all vaccinated people to resume covering up indoors—as the agency’s internal document called for. That would’ve generated some whiplash, too, Kuppalli told me, but it would have at least been more straightforward, and might have felt less wishy-washy; it might have signaled a more collective movement, toward a common goal. As it stands, the agency’s new guidance is murky and riddled with contingencies: Even vaccinated Americans in low- and moderate-transmission areas, it states, should consider masking up indoors if they or someone in their household is immunocompromised, at risk for severe disease, or unvaccinated. That last category includes all kids under 12—roughly 50 million Americans who haven’t yet been greenlit for their shots. The CDC’s Tuesday announcement also included a call for universal masking in schools nationwide. “This continues to be exhausting,” Ariangela Kozik, a microbiologist at the University of Michigan, told me. Kozik’s 5-year-old remains unvaccinated, and she said she’s struggling to navigate a community where attitudes toward vaccination and masking are extremely split. Communities are, after all, where many people will acquire their cues on risk, certainly more than from a color-coded map. People will look to their neighbors, their families, their friends, the strangers they see weaving in and out of grocery stores, Ranney said. Mask wearing will encourage more masking—and vice versa. The country’s approach to the pandemic has been, for the past year and a half, a patchwork of attitudes, and by now, it’s fairly easy to see the loophole this creates. Vaccines have been buffering communities against Delta; where immunization rates are high, transmission has been low. But the places where people have been reluctant to line up for their shots are also some of the spots where masks frequently get snubbed. Incentive can also bottom out when people feel like they’re missing out on perks others get to enjoy. If fully vaccinated people in other parts of the country can still eschew masks indoors, shouldn’t everyone who’s gotten their shots, and even some that aren’t, be exempt? At the other extreme, a misconstrued map might signal to vaccinated people in low-risk areas that they’re free to opt out of everyone else’s crisis. A virus travels best when people forget to be considerate of one another. The general messaging on masks, Robinson and others pointed out, oversimplifies in other ways, too. Calls for more vaccination—still our best long-term solution to combat the coronavirus—have been drowned out by debates over personal freedom. Little attention is being paid to the quality of masks, and the high-filtration types that more effectively block inbound virus. Discussions about ventilation, testing access, contact tracing, and other preventative measures have similarly fallen to the wayside. Even people who are ready and willing to mask up again indoors are struggling to figure out what counts as “public” and what groups are “small.” The map is a single tool and, to me, better suited to assessing the national than the hyper-local. Most of New England, where I’m based, is still yellow. But those regions are in a dwindling minority. Some 70 percent of American counties are, according to the map, currently on fire; that percentage will probably tick up before it drops again. For now, I am tracking my pandemic circumstances. But my boundaries for my “community” are bigger than what the map says they are. They don’t stop at my county line, or my state line. They go as far as the virus treads—everywhere. Right now, I’m masking for as many people as I can. from https://ift.tt/3j8QKs3 Check out http://natthash.tumblr.com America’s split with masks turned out to be a brief hiatus. After getting their shots in the spring and early summer, many people figured they could dump their face coverings for good—a sentiment the CDC crystallized in May, when the agency gave fully immunized people its blessing to largely dispense with masking, indoors and out. Yesterday, the agency pivoted back, recommending that even fully vaccinated people wear masks under certain high-risk circumstances, including in public indoor spaces in parts of the country where the virus is surging, Director Rochelle Walensky said in a press briefing. (She specified places where new case numbers exceed 50 per 100,000 people in the past seven days; that currently includes about two-thirds of U.S. counties.) With an ultra-contagious SARS-CoV-2 variant rampaging, face coverings are being called upon to once again supplement the protection offered by vaccines. The CDC’s decision, which many public-health researchers have been anticipating for weeks, might look like a flip-flop or a fumble, some sort of masking mea culpa. But to me, and the experts I talked with, redonning masks (or simply keeping them on, as many people have) is not some shameful regression to the dark ages of the pre-vaccination era. Nor is it an indictment of the COVID-19 vaccines, which are doing an extraordinary job of curtailing the global burden of disease. Instead, it’s a doubling down on two defenses that we know work, and work well together. [Read: 4 reasons I’m wearing a mask again.] Like any dynamic duo, masks and vaccines share a goal—preventing infection, disease, and virus transmission—and they accomplish it in complementary ways. “They should be seen hand in hand, as helping one another,” Abraar Karan, an infectious-disease physician at Stanford University, told me. We now understand this notion better than ever before, and many experts think anyone who wants to reduce their risk of catching and passing the virus should use both, CDC criteria notwithstanding. Masks, after all, are reemerging in response to the fast-changing conditions around us—offering another layer of protection at a time when we need it most, in much the same way we seek out umbrellas when it rains, sunscreen when it’s sunny, and better security systems when our neighborhood crime rates tick up. “With Delta being such a dominant force, we need to include every layer we can think of,” Akiko Iwasaki, an immunologist at Yale University, told me. The vaccines are excellent. But while so many people remain vulnerable, and the virus continues to shape-shift, shots can’t shoulder the burden of protection alone. Our understanding of masks is evolving; for now, they still have a crucial role to play, as a partner to the shots we'll be depending on long term. Partnering masks and vaccines is, in many ways, a natural move. If an unmasked, unvaccinated body is like an unprotected bank, vulnerable to burglars, these two tools are akin to the different high-security measures used to prevent a heist. Shots steel the institution from the inside out, papering its walls with most-wanted posters and alerting bank personnel to upswings in local crime. Supersensitive alarms get installed at windows; extra security guards are stationed throughout the building; the local sheriff’s office is put on speed dial. Should thieves try to force their way in, they’ll be recognized as familiar foes and get arrested on the spot, maybe before any real damage can be done. COVID-19 vaccines have proved themselves ace at deploying these safeguards and preventing symptomatic disease, especially in its most severe forms, even when tangoing with variants. That is the classic vaccination modus operandi: fortifying our defenses so a pathogen has higher hurdles to clear. But even vaccinated immune systems can be somewhat foiled when local conditions change. A well-armored bank will still be better off than an unsecured one, but could struggle to thwart career criminals—ones who are savvy enough to show up en masse, move fast, and use brutal tactics. And more of those robbers might make it out of the scuffle unscathed and eager to hit up a neighboring bank. Vaccine-prepped immune systems are still mostly clobbering Delta, the SARS-CoV-2 variant that’s now found in 80 percent of the virus samples being sequenced across the nation: People who have gotten all their shots are a lot less likely to experience symptoms, hospitalization, or death, and don’t seem to be responsible for much virus transmission. But Delta also appears to be especially good at accumulating in airways, and seems to eke past some of our immune defenses. These troubling traits might make it easier for the virus to mildly sicken some inoculated individuals, and perhaps spread from them as well. Vaccines are an imperfect shield; variants like Delta find their way through the cracks. Masks cut down on all of this risk. If vaccines shore up security from the inside, face coverings (which, you know, literally cover your face) erect a sturdy blockade around the bank’s exterior—fences, bars, better locks, and ID checks at an intruder’s typical point of entry. Masks are physical barriers; they’re “great at preventing exposure to large doses of virus” before the invaders even enter the premises, Iwasaki said. And in the same way that it’s easier for security guards to incapacitate just a few crooks busting through the door, “the less virus you need to fight off, the better—I think that’s pretty clear,” Marion Pepper, an immunologist at the University of Washington, told me. Masks, in other words, curb the amount of labor our immune systems are forced to do—in some cases, maybe eliminating the threat entirely. In that way, they accomplish something vaccines can’t: Unlike immune cells, they don’t have to wait until after the virus has broken into the body to act. That’s an especially big asset for people whose bodies are less equipped to respond to vaccines, including the elderly and the immunocompromised, populations the CDC says should mask more vigilantly indoors, regardless of where they live. [Read: Mask mandates will come and go.] Masks might be a particularly important pairing for our current vaccines, which are administered in an arm muscle, rather than the nose—SARS-CoV-2’s natural point of entry. The shot’s contents will still effectively school immune cells and molecules all over the body, but they won’t do much to marshal defenders that specialize in guarding the slimy tissues carpeting the airway and gastrointestinal tract. It’s the difference between keeping security guards on retainer in a bank’s back room, and posting agents at the building’s entrance: Defenses will be mounted either way, but fighters who have to scramble from one location to another will probably lose speed and oomph. A barrier that waylays some viral particles, however, might buy these guards time to rush to the fore. Masks reduce the strain on the body, and keep immune cells in a zone where they can comfortably fight. Our vaccines are very powerful, but their performance was first measured in clinical trials while masking was widespread. Study volunteers were “asked to act as if they were unvaccinated, and keep all other protections in place,” Michal Tal, an immunologist at Stanford, told me. The startlingly low rates of illness among vaccinated volunteers in those studies likely aren’t attributable to the jabs alone. Even against an earlier iteration of the virus, the shots were being supported by an entourage of precautions; mirroring that initial tag-team approach might not be a bad idea. The combo of masks and vaccines does a number on outbound viruses as well. Unimmunized, unmasked bodies are good stages for pathogens to reproduce unfettered, then hop into a nearby human. Vaccines coach immune cells to vanquish as many viral particles as they can; masks trap any potential escapees inside. “People need to remember we live in very interconnected societies,” Karan said. While vaccinated people might remain mostly safe from serious disease, plenty of the people around them—especially those who remain uninoculated, including young kids—remain at much higher risk. A virus that keeps spreading, even silently, makes the pandemic that much harder to end. Karan points out that masks are also a great insurance policy. Vaccines still carry uncertainties: Although experts think that COVID-19 shots are reducing all forms of infection and disease, the extent to which they block long COVID remains murky. Researchers also don’t know when vaccine-trained immune cells might start to forget the coronavirus, or when the pathogen might mutate into more evasive forms. If we end up needing boosters or reformulated vaccines, face coverings might keep some people from falling sick while those reinforcements arrive. “I think masks are our lowest hanging fruit to buy us time,” Karan said. Some people are already criticizing the CDC’s announcement as a baffling U-turn, maybe even a bellwether of worse restrictions to come. Experts told me that’s the wrong way to view the update, which should be considered an improvement over the status quo—a step forward, not a step back. Combining masks and vaccines reaffirms that we know how to protect ourselves against this fast-changing virus, and match the curveballs it throws our way. Taison Bell, a critical-care and infectious-disease physician at UVA Health in Virginia, told me he sees masks as empowering—not some handicap he’s been saddled with. “It doesn’t represent something that restricts my freedom,” he said. “It allows me to enter a space and do what I need to do.” The shift in guidance is, in a way, crystallizing a new attitude toward masking, one that will probably stick around in some form or another, even after the pandemic comes to an official close. These past 16 months have underscored the power of masks to prevent all manner of pathogens, and stave off some medical conditions; face coverings might become standard practice, socially, seasonally, as people get more in tune with public health. That’s the upside of crisis. It forces us to react, and hopefully react well. It calls on us to adapt, when we realize our circumstances have changed. from https://ift.tt/3BQyjkw Check out http://natthash.tumblr.com The genome of a mouse is, structurally speaking, a chaotic place. At some point in its evolutionary past, the mouse shuffled its ancestral genome like a deck of cards, futzing up the architecture that makes most other mammalian genomes look, well, mammalian. “I always consider it the greatest outlier,” Bill Murphy, a geneticist at Texas A&M University, told me. “It’s about as different from any other placental mammal genome as you can find, sort of like it’s the moon, compared to everything else being on the Earth.” Mouse genomes are still incredibly useful. Thanks to years of careful tinkering, meticulous mapping, and a bonkers amount of breeding, researchers have deciphered the murine genetic code so thoroughly that they can age the animals up or down or alter their susceptibility to cancer, findings that have big implications for humans. But the mouse’s genomic disarray makes it less suited to research that could help us understand how our own genetic codes are packaged and stored. Which is why some researchers have turned to other study subjects, just one step up the food chain. Cats, it turns out, harbor genomes that look and behave remarkably like ours. “Other than primates, the cat-human comparison is one of the closest you can get,” with respect to genome organization, Leslie Lyons, an expert in cat genetics at the University of Missouri, told me. Lyons and Murphy, two of the world’s foremost experts in feline genetics, have been on a longtime mission to build the ranks in their small field of research. In addition to genetic architecture, cats share our homes, our diets, our behaviors, many of our microscopic pests, and some of the chronic diseases—including diabetes and heart problems—that pervade Western life. “If we could start figuring out why those things happen in some cats, but not others,” Lyons told me, maybe humans and felines could share a few more health benefits as well. Feline genomes are now being mapped essentially end to end, “with a nearly perfect sequence,” Lyons said, a feat that researchers have only recently managed with people. Complete genomes create references—pristinely transcribed texts for scientists to scour, without blank pages or erasures to stymie them. Cats can’t tell us when they’re sick. But more investment in feline genomics could pave the way for precision medicine in cats, wherein vets assess genetic risk for different diseases and intervene as early as possible, giving them “a jump on diagnostics,” Elinor Karlsson, a vertebrate genomics expert at the Broad Institute, told me. Because humans and cats are bedeviled by some of the same diseases, identifying their genetic calling cards could be good for us too. Cats can develop, for instance, a neurological disorder that’s similar to Tay-Sachs disease, “a life-ending disease for children,” Emily Graff, a veterinarian and geneticist at Auburn University, told me. But gene therapy seems to work wonders against the condition in cats, and Graff’s colleagues plan to adapt a treatment for its analogs in kids. [Read: The human genome is—finally!—complete.] The cat genome could fuel more basic science pursuits as well, Lyons told me. Essentially all the cells in our bodies contain identical genomes, but have extraordinarily different developmental fates. Researchers have been trying for decades to untangle the mechanics of this process, which requires cells to force some of their genes into dormancy, while keeping others in frequent use. One of the most dramatic examples of this phenomenon is the silencing of one of the two X chromosomes in female cells. “We still don’t have a good sense of how genes get turned on and off,” Sud Pinglay, a geneticist at New York University, told me. “This is an entire chromosome.” X inactivation is what dapples the coats of calicos. These cats are almost exclusively female, and must be genetic mutts: One of their X chromosomes carries an orange-furred gene, and the other, a black. In any given cell, only one chromosome stays awake. That decision happens early in a cat’s development, and the cells that split off from these lineages stay faithful to the color their parent cells picked, creating big patches of color. “That helped us put together that the inactivated X chromosome was relatively stable, and kept stable for many rounds of cell division,” Sundeep Kalantry, an X-inactivation expert at the University of Michigan, told me. “That’s why the calico cat holds such an exalted place in X inactivation.” Genomes can be so stubborn about X inactivation that they will hold their ground even after being moved into other cells. The first cloned cat, named Carbon Copy, or CC for short, was genetically identical to a classically colored calico named Rainbow. But CC was born sporting only shades of brown and white: She had, apparently, been created out of a cell that had shut its orange X off, and had refused to reverse the process. Many of the vagaries of gene and chromosome silencing—their relative permanence or impermanence in different contexts, for instance—are still being worked out in different species by researchers including Kalantry, whose lab website features a fetching photo of a calico. But they have long known that the shape and structure of a genome, and the arrangement of the genes within, hold sway over how the contents are expressed. Most of our genome is thought to be annotations and embellishments that shape how the rest of it is read; snippets of DNA can even twist, bend, and cross great distances to punctuate one another. That’s one big area where cats can help us, Lyons told me: If their genes are organized like ours, maybe they’re regulated like ours too. “Maybe this is where the cats get to step in,” she said. [Read: A much-hyped COVID-19 drug is almost identical to a black-market cat cure] Some people might feel uneasy about the idea of studying felines in the lab. But Murphy notes that lots of genetic work can be done quite gently. His team has gotten very good at extracting gobs of DNA from cat cheek cells, using little wire brushes that they swivel into the animals’ mouths. There are also huge perks to working with popular pets: People in the community are often eager to contribute, either directly or through their vets. When cats get sick, researchers can sample them, and in many cases, help them get healthy again. “I’d say about 90 percent of studies on cats are done on naturally occurring disease models,” Murphy told me. And the cats who pass through Lyons’ lab in Missouri, she told me, get adopted after they’ve retired from their scientific careers. Mice are easy and cheap to breed and house in labs, and they’ve had a hell of a head start in scientific research already. Cats are unlikely to outpace them; they might not even surpass dogs, which are especially eager to work with humans, and have done so extensively, Gita Gnanadesikan, a canine researcher at the University of Arizona, told me. As research volunteers, cats tend to be more sullen and reserved. (Canines, too, come with drawbacks. We know a lot about their genomes, but dog breeds have been so genetically siloed that their populations “are not diverse, so they’re not as good a model for humans,” Karlsson told me.) But cats have their place, experts told me—as a member of an entire menagerie of animals that humans would benefit from understanding better. “In genetics, there’s this tension: Do you try to learn everything you can about a small number of organisms, or do you branch out and try to learn little bits about a larger number of species?” Gnanadesikan told me. “I think one of the answers to that is just … yes.” from https://ift.tt/3f4GX59 Check out http://natthash.tumblr.com A new dichotomy has begun dogging the pandemic discourse. With the rise of the über-transmissible Delta variant, experts are saying you’re either going to get vaccinated, or going to get the coronavirus. For some people—a decent number of us, actually—it’s going to be both. Coronavirus infections are happening among vaccinated people. They’re going to keep happening as long as the virus is with us, and we’re nowhere close to beating it. When a virus has so thoroughly infiltrated the human population, post-vaccination infections become an arithmetic inevitability. As much as we’d like to think otherwise, being vaccinated does not mean being done with SARS-CoV-2. Post-vaccination infections, or breakthroughs, might occasionally turn symptomatic, but they aren’t shameful or aberrant. They also aren’t proof that the shots are failing. These cases are, on average, gentler and less symptomatic; faster-resolving, with less virus lingering—and, it appears, less likely to pass the pathogen on. The immunity offered by vaccines works in iterations and gradations, not absolutes. It does not make a person completely impervious to infection. It also does not evaporate when a few microbes breach a body’s barriers. A breakthrough, despite what it might seem, does not cause our defenses to crumble or even break; it does not erase the protection that’s already been built. Rather than setting up fragile and penetrable shields, vaccines reinforce the defenses we already have, so that we can encounter the virus safely and potentially build further upon that protection. To understand the anatomy of a breakthrough case, it’s helpful to think of the human body as a castle. Deepta Bhattacharya, an immunologist at the University of Arizona, compares immunization to reinforcing such a stronghold against assault. Without vaccination, the castle’s defenders have no idea an attack is coming. They might have stationed a few aggressive guard dogs outside, but these mutts aren’t terribly discerning: They’re the system’s innate defenders, fast-acting and brutal, but short-lived and woefully imprecise. They’ll sink their teeth into anything they don’t recognize, and are easily duped by stealthier invaders. If only quarrelsome canines stand between the virus and the castle’s treasures, that’s a pretty flimsy first line of defense. But it’s essentially the situation that many uninoculated people are in. Other fighters, who operate with more precision and punch—the body’s adaptive cells—will eventually be roused. Without prior warning, though, they’ll come out in full force only after a weeks-long delay, by which time the virus may have run roughshod over everything it can. At that point, the fight may, quite literally, be at a fever pitch, fueling worsening symptoms. Vaccination completely rewrites the beginning, middle, and end of this story. COVID-19 shots act as confidential informants, who pass around intel on the pathogen within the castle walls. With that info, defensive cells can patrol the building’s borders, keeping an eye out for a now-familiar foe. When the virus attempts to force its way in, it will hit “backup layer after backup layer” of defense, Bhattacharya told me. Prepped by a vaccine, immune reinforcements will be marshaled to the fore much faster—within days of an invasion, sometimes much less. Adaptive cells called B cells, which produce antibodies, and T cells, which kill virus-infected cells, will have had time to study the pathogen’s features, and sharpen their weapons against it. While the guard dogs are pouncing, archers trained to recognize the virus will be shooting it down; the few microbes that make their way deeper inside will be gutted by sword-wielding assassins lurking in the shadows. “Each stage it has to get past takes a bigger chunk out” of the virus, Bhattacharya said. Even if a couple particles eke past every hurdle, their ranks are fewer, weaker, and less damaging. In the best-case scenario, the virus might even be instantly sniped by immune cells and antibodies, still amped up from the vaccine’s recent visit, preventing any infection from being established at all. But expecting this of our shots every time isn’t reasonable (and, in fact, wasn’t the goal set for any COVID-19 vaccine). Some people’s immune cells might have slow reflexes and keep their weapons holstered for too long; that will be especially true among the elderly and immunocompromised—their fighters will still rally, just to a lesser extent. Changes on the virus side could tip the scales as well. Like invaders in disguise, wily variants might evade detection by certain antibodies. Even readily recognizable versions of the coronavirus can overwhelm the immune system’s early cavalcade if they raid the premises in high-enough numbers—via, for instance, an intense and prolonged exposure event. With so many factors at play, it’s not hard to see how a few viral particles might still hit their mark. But a body under siege isn’t going to throw its hands up in defeat. “People tend to think of this as yes or no—if I got vaccinated, I should not get any symptoms; I should be completely protected,” Laura Su, an immunologist at the University of Pennsylvania, told me. “But there’s way more nuance than that.” Even as the virus is raising a ruckus, immune cells and molecules will be attempting to hold their ground, regain their edge, and knock the pathogen back down. Those late-arriving efforts might not halt an infection entirely, but they will still curb the pathogen’s opportunities to move throughout the body, cause symptoms, and spread to someone else. The inhospitality of the vaccinated body to SARS-CoV-2 is what’s given many researchers hope that long COVID, too, will be rarer among the immunized, though that connection is still being explored. Breakthroughs, especially symptomatic ones, are still uncommon, as a proportion of immunized people. But by sheer number, “the more people get vaccinated, the more you will see these breakthrough infections,” Juliet Morrison, a virologist at UC Riverside, told me. (Don’t forget that a small fraction of millions of people is still a lot of people--and in communities where a majority of people are vaccinated, most of the positive tests could be for shot recipients.) Reports of these cases shouldn’t be alarming, especially when we drill down on what’s happening qualitatively. A castle raid is worse if its inhabitants are slaughtered and all its jewels stolen; with vaccines in place, those cases are rare—many of them are getting replaced with lighter thefts, wherein the virus has time only to land a couple of punches before it’s booted out the door. Sure, vaccines would be “better” if they erected impenetrable force fields around every fortress. They don’t, though. Nothing does. And our shots shouldn’t be faulted for failing to live up to an impossible standard—one that obscures what they are able to accomplish. A breached stronghold is not necessarily a defeated stronghold; any castle that arms itself in advance will be in a better position than it was before. There’s a potential silver lining to breakthroughs as well. By definition, these infections occur in immune systems that already recognize the virus and can learn from it again. Each subsequent encounter with SARS-CoV-2 might effectively remind the body that the pathogen’s threat still looms, coaxing cells into reinvigorating their defenses and sharpening their coronavirus-detecting skills, and prolonging the duration of protection. Some of that familiarity might ebb with certain variants. But in broad strokes, a post-inoculation infection can be “like a booster for the vaccine,” Su, of the University of Pennsylvania, told me. It’s not unlike keeping veteran fighters on retainer: After the dust has settled, the battle’s survivors will be on a sharper lookout for the next assault. That’s certainly no reason to seek out infection. But should such a mishap occur, there’s a good chance that “continuously training immune cells can be a really good thing,” Nicole Baumgarth, an immunologist at UC Davis, told me. (Vaccination, by the way, might mobilize stronger protection than natural infection, and it’s less dangerous to boot.) We can’t control how SARS-CoV-2 evolves. But how disease manifests depends on both host and pathogen; vaccination hands a lot of the control over that narrative back to us. Understanding breakthroughs requires some intimacy with immunology, but also familiarity with the realities of a virus that will be with us long-term, one that we will probably all encounter at some point. The choice isn’t about getting vaccinated or getting infected. It’s about bolstering our defenses so that we are ready to fight an infection from the best position possible—with our defensive wits about us, and well-armored bodies in tow. from https://ift.tt/3kXXThq Check out http://natthash.tumblr.com Earlier this month, I pulled a mask out of the bin of hats, scarves, and gloves I keep by the door; strapped it on; and choked. I had inhaled a mouthful of cat hair—several weeks’ worth, left by my gray tabby, Calvin, who has been napping on a nest of face coverings since I largely dispensed with them in May. I’ve been fully vaccinated for two months. I spent the end of spring weaning myself off of masking indoors, and exchanging, for the first time, visible smiles with neighbors in the lobby of our apartment building. I dined, for the first time in a year and a half, at a restaurant. I attended my first party at another (vaccinated) person’s home since the spring of 2020. I am, after all, now at very low risk of getting seriously sick should SARS-CoV-2 infect me, thanks to Pfizer’s vaccine. But the pandemic is once again entering a new phase that feels more dangerous and more in flux, even for the people lucky enough to have received their lifesaving shots. A more transmissible variant—one that can discombobulate vaccine-trained antibodies—has flooded the world. It’s wreaking havoc among the uninoculated, a group that still includes almost half of Americans and most of the global population. After a prolonged lull, the pandemic’s outlook is grimmer than it’s been in months. I am, for the foreseeable future, back to wearing masks in indoor public places, and there are four big reasons why. 1. I don’t want to get COVID-19.Let me be clear: My chances of getting sick are low, very low, especially if I’m thinking about the disease in its worst forms. The vaccines are spectacularly effective at blocking COVID-19, particularly cases that lead to hospitalization or death, even when squaring off with Delta and other antibody-dodging variants. I expect this to hold true for some time: These vaccines were tested primarily for their power to curb deadly illness, and that’s what they’re accomplishing against every version of the coronavirus they face. But no vaccine is perfect. Some immunized people will end up infected with the virus; a small subset of this group will fall ill, occasionally severely so. The proportion of vaccinated people who catch the coronavirus might tick up in the presence of certain mutations that make the virus less recognizable to vaccinated immune systems, and thus harder to purge. The longer the virus sticks around in the body—the more opportunity it’s given to copy itself and mosey through our tissues—the more likely it is that symptoms will arise as immune defenders rally to fight. (Delta might be extra well equipped to accumulate in airways.) Most post-vaccination infections, or breakthroughs, appear to be asymptomatic or mild, a sign that the vaccines are doing their job. But mild illness still isn’t desirable illness, especially given the threat of long COVID, which reportedly can happen in vaccinated people, though researchers aren’t yet sure how widely. Masks slash the risks of all of these outcomes. Breakthroughs are more common when the immune system faces a ton of inbound virus—when there’s an ongoing outbreak, or when the people around me aren’t immune. A mask reduces my exposure every time I wear one. Some variants, including Delta, might be more transmissible, but they’re still thwarted by physical barriers such as cloth. I’m not duping myself into thinking that I’ll stave off this virus forever; SARS-CoV-2 is here to stay. But as hospitals in several states once again start to fill up, I’m in no rush to rendezvous with the coronavirus, especially because … 2. I don’t want people around me to get COVID-19.If I get infected, that affects more than just me. I worry about the strangers I encounter—many of them maskless—whose immune status I don’t know. I worry about the youngest kids in my social network, who aren’t yet eligible for shots, and the elderly and immunocompromised, whose defenses may be weaker than mine. I worry about the people in my community who have been structurally barred from accessing the vaccines, or who are reluctant to take the shots. My risk of getting COVID-19 is low. Theirs is very much not. The COVID-19 vaccines come with the delightful perk of blocking some asymptomatic infection, but researchers are still figuring out how often vaccinated people can pass on the pathogen. The math gets all the messier with more contagious variants such as Delta. Inbound virus affects me directly, but it can also turn me into a pathogen pit stop, potentially allowing outbound virus to bop into someone with less immunological armor. “Masks protect both us and the people around us,” Krutika Kuppalli, an infectious-disease physician at the Medical University of South Carolina, told me. In the United States, inoculation rates have taken a serious dip. The proportion of vulnerable people is stagnant, yet still too high. During a pandemic, personal safety can’t be the only consideration, as my colleague Ed Yong has written. The disease we’re dealing with is infectious; the repercussions of our behavior ripple to those around us. Many unvaccinated people belong to populations that have been marginalized by the country’s fractured health-care system. Saddling them with any increased COVID-19 risk, even indirectly, threatens to widen disparities. Going maskless indoors still feels like a gamble, especially because … 3. I trust the vaccines, but I understand their limits.My pivot back to masks says nothing about my continued confidence in the vaccines and what they’re capable of. But although vaccines are an excellent tool, they are also an imperfect one, and they’ll perform differently depending on the context in which they’re used. Consider, for example, the effectiveness of sunscreen, another stellar yet flawed preventive. Certain brands, including those with higher SPF, will be better than others at blocking burns and cancer. Mileage may vary even with the same tube of sunscreen, depending on who’s using it (how much melanin is in their skin?), how they’re behaving (are they dipping in and out of the shade, or spending all day soaking up rays?), and local conditions (is it a cloudy day in a wooded park, or a sunny day on a snow-speckled hill?). Vaccines are similar. Breakthroughs are more likely in people with a weakened immune system and those who mingle frequently with the virus; they may happen more often with certain variants. Asking a vaccine to shoulder the entire burden of protection felt all right a month ago, when case rates were plunging. Now they’re ticking back up. The vaccines don’t feel different, but the conditions they’re working in do. Maybe now’s not the best time to rely on them alone. “That’s putting a lot of pressure on the vaccines,” Jason Kindrachuk, a virologist at the University of Manitoba, told me. The virus has upped the ante, and I feel the urge to match it. When it’s extra sunny out, I’m probably going to reach for sunscreen and a hat, especially because … 4. Wearing an accessory on my head doesn’t feel like a huge cost to me.Don’t get me wrong. I don’t enjoy wearing a mask, and all else equal, I’d still prefer to keep it off. But for me, it’s not a big sacrifice to make for a bit more security: I’ll mainly be using one indoors when I’m around strangers, a situation in which the risk of spread is high. And I’ll keep checking pandemic conditions like I would a weather forecast—hospitalizations, variants, immunization rates, and the behaviors of people around me—and adjust as needed. The idea is that this state of affairs will be short-lived, until vaccinations climb and the virus retreats again. I live in New England, where things are relatively calm. I could probably get away with resuming normal life, whatever that is. But the status quo feels tenuous. It will take work to maintain. As Delta dominates the nation and case rates rise, we may already be losing our grip. Kuppalli said that although she’s concerned about our current menagerie of variants, she’s also trying to ensure that more problematic versions of the virus don’t have the opportunity to arise. The stakes in her community are particularly high: In South Carolina, where vaccination rates are relatively low, “it’s a free-for-all,” she said. “When I walk into a supermarket, I’m the only one in a mask. People look at you like you’re crazy.” Vaccines have sometimes been billed as an option to supplant the nuisance of masks. But making that trade-off at an individual level feels overly simplistic in a population where so many people are neither immune nor covered up. I also didn’t get vaccinated because I wanted to stop masking. I got vaccinated because I wanted to reduce my chances of getting sick with this virus and transmitting it to others. Masking is a complementary means to the same end. My return to it isn’t an indictment of vaccination. It’s an insurance policy. It’s a small price to pay for more protection, especially once I’ve washed the cat hair away. from https://ift.tt/3kYTURR Check out http://natthash.tumblr.com Last week, CDC Director Rochelle Walensky said that COVID-19 is “becoming a pandemic of the unvaccinated.” President Joe Biden said much the same shortly after. They are technically correct. Even against the fast-spreading Delta variant, the vaccines remain highly effective, and people who haven’t received them are falling sick far more often than those who have. But their vulnerability to COVID-19 is the only thing that unvaccinated people universally share. They are disparate in almost every way that matters, including why they haven’t yet been vaccinated and what it might take to persuade them. “‘The unvaccinated’ are not a monolith of defectors,” Rhea Boyd, a pediatrician and public-health advocate in the San Francisco Bay Area, tweeted on Saturday. Boyd has been talking to underserved communities about COVID-19 vaccines since November, before any were even formally authorized. Together with several partner organizations, she co-developed a national campaign called The Conversation, in which Black and Latino health-care workers provide information (and dispel misinformation) about the vaccines. She has spoken virtually to dozens of community groups, including churches and schools, fielding their questions about the shots. I reached out to Boyd because I wanted to know what she has learned through all these encounters about why some people are still unvaccinated and what to do about it. Our conversation has been edited for length and clarity. Ed Yong: You recently spoke with people in southern Georgia who had many lingering questions about vaccines. On Twitter, you said, “Every question they asked was legitimate and important.” Tell me more about the event and the questions you were getting. Rhea Boyd: It was a tele-townhall, and around 5,000 people participated. I would have imagined that people who stayed on would be unvaccinated, but the people who asked questions were a mix. I had one gentleman who was vaccinated with Johnson & Johnson and he asked, “Did I get a safe shot?” We affirmed for him that this far after his vaccination, he’s likely safe, but that opened my eyes. If you’ve heard about that serious side effect and are worried if you’re at risk, you’re probably not encouraging the people around you to be vaccinated. Yong: That’s fascinating to me. There’s a tendency to assume that all vaccinated people are pro-vaccine and all unvaccinated people are anti-vaccine. But your experience suggests that there’s also vaccine hesitancy among vaccinated people. [Read: America is now in the hands of the vaccine-hesitant] Boyd: Yes, and we tend to hear similar questions among people who are unvaccinated. They may also have heard common threads of disinformation, but they’re still asking basic questions. The top one is around side effects, which are one of the main things we talk about when we give informed consent for any procedure. If people aren’t sure about that, it’s no wonder they’re still saying no. A lot of vaccine information isn’t common knowledge. Not everyone has access to Google. This illustrates preexisting fault lines in our health-care system, where resources—including credible information—don’t get to everyone. The information gap is driving the vaccination gap. And language that blames “the unvaccinated” misses that critical point. Black folks are one of the least vaccinated groups, in part because they have the least access to preventive health-care services. Yong: I’m glad you raised the issue of access. Everyone age 12 and up is now eligible for vaccines, and President Biden promised that 90 percent of people would have a vaccination site within five miles of their home. I’ve heard many people doubt that vaccine access is still an issue and, by extension, that anyone who is still unvaccinated must be hesitant or resistant. Do you disagree? Boyd: Availability and access aren’t the same thing. If you have to walk the five miles, you’re going to rethink getting vaccinated, especially if you’re elderly, or you have chronic disease, or the round trip is interfering with other things like work. [Much of] our paid workforce doesn’t have flexibility about hours, or couldn’t take a day off if they wanted to. And if you don’t have paid sick leave to deal with the vaccine or the potential side effects of the second dose, you’ll skip it because feeding your family is more important right now. Child care is also an enormous issue. If you don’t have someone to watch your children, then what do you do? Many of these things the Biden administration has tried to address. They have programs involving Uber and Lyft. Child-care organizations have signed on to help with vaccine appointments. There are tax breaks for companies that offer paid sick leave. These are incredible, but they may not filter down to your area. We need to think about local interventions to help stretch them. [Read: The surprising key to combatting vaccine refusal] Yong: If these barriers to access were all addressed, do you have a sense of the proportion of people who would then get vaccinated? Boyd: The truth is we don’t know. If you’re not getting vaccinated, we have even less data on you than if you are vaccinated. But we know that these barriers exist for even basic care. How do we make sense of the fact that some people won’t get critical medications, like their diabetes medications? Or that some people forgo necessary medical care even as they experience complications from chronic illness? It’s not that those individuals don’t want basic medical care! It’s that groups face structural barriers to accessing that care, including rural folks, underinsured folks, and Black folks in particular. Those structural barriers are likely at play for vaccinations too. This is a problem for health care more generally. We’ve been willing to move on without people, while leaving them without resources to fend for themselves. Yong: What about people at the other extreme, who do have easy access but who are vitriolically opposed to vaccines—people who could more reasonably be described as anti-vaxxers? Boyd: Anti-vaxxers are incredibly vocal, and because of that, they’ve been a disproportionate focus of our vaccine outreach. But I think that they represent a small part of people in this country, and especially in our communities of color, an irrelevant part. In our work, we haven’t given much credence to their bluster. But the rampant disinformation that’s put out by this minority has shaped our public discourse, and has led to this collective vitriol toward the “unvaccinated” as if they are predominantly a group of anti-vaxxers. The people we’re really trying to move are not. Yong: I’ve never thought of it that way. We’re used to thinking of anti-vaxxers as sowing distrust about vaccines. But you’re arguing that they’ve also successfully sown distrust about unvaccinated people, many of whom are now harder to reach because they’ve been broadly demonized. Boyd: Yes. The language we use around unvaccinated people comes with a judgment—a condescension that “you’re unvaccinated and it’s your choice at this point.” That attitude is papering Twitter. It’s repeated by our top public-health officials. They’re railing on the unvaccinated as if they’re holding the rest of us back from normalcy. But unvaccinated people aren’t a random group of defectors who are trying to be deviant. They’re not all anti-vaxxers. They’re our kids! Any child under 12 is in that group. Yong: Okay, but even if extreme cases are a minority, we can’t ignore them. When I reported on the ongoing surge in Missouri, a hospital chief told me that one patient spat in a nurse’s eye because she told him he had COVID-19 and he didn’t believe her. How do you think about folks who have gotten to that point? [Read: Delta is driving a wedge through Missouri] Boyd: These very contentious encounters are driven by people really staunchly holding on to something that they are served by in some way. Maybe it’s the source that belief came from, and they need to believe other things that source says. Maybe they want camaraderie or collegiality with people around them, so they can feel that they’re in an in-group. People need to believe that what they believe is true. They feel threatened when challenged about something to which they feel beholden. The best way to address that may not be to actually challenge them one-on-one, but to shift what people around them are talking about. If you hear enough stories in your Facebook feed or from strangers in the store that reinforce the science, it’ll make what you’re saying less reasonable to you. And less useful to you. And once you don’t need to hold on to it, you can let it go. Yong: Which is why community-based efforts are so important. People who will be swayed by Anthony Fauci are already listening to him. But, for example, public-health professionals I spoke with in Missouri are trying to get pastors, firefighters, and community leaders to act as trusted voices for their own people. Boyd: Exactly. At the beginning of the pandemic, we drew on data about how physicians of color were trusted messengers for communities of color. But there are so few of us—only 5 percent of our physician workforce is Black. That isn’t enough. But I think we’re too limited in our thinking about who is a trusted messenger. People use informal communication chains: They have side conversations with the grocery-store clerk, or their niece and nephew. People will believe anecdotal health-care information that their family member suggests over the credible info that a health-care professional is giving. We’ve talked to virtual faith-based groups on Sundays. We’ve talked to barbershops, after-school organizations, and boys’ and girls’ clubs. Some of these groups are small—hundreds of people, or sometimes just 20. People are then much more specific about their concerns without the things they usually have bluster around. I wonder how many people arrogantly respond about vaccinations during more formal conversations, but then come to our events and share something vulnerable in these protected settings where they’re surrounded by their pastor and people they know. Yong: This has the added benefit of promoting vaccinations among groups of people who are likely to encounter one another. My concern, however, is that this is slow work—and Delta is moving fast. Does it feel like you’re stuck in a war of attrition against misinformation, while time is running out? [Read: The 3 simple rules that underscore the danger of Delta] Boyd: It’s true. Now that vaccines aren’t novel, we’ve lost some of that early momentum when people would go to their local Walgreens. Now we have to do the heavy, high-touch work, making sure that we proactively reach out to everyone. And we can only go as fast as people are willing to go. That’s concerning, and it’s why we need to reimplement mitigation strategies, like indoor masking, in addition to vaccination. That’ll give us the time to do the work. No form of mitigation will block transmission 100 percent, but we have to use them together. When the cavalry arrives, it’s not like all the other soldiers on the field just leave. Yong: When I talk to people about the vaccination challenge, the main emotions I hear are frustration and despair. So perhaps the most surprising part of this conversation for me is that you sound … hopeful? Boyd: Yes. I feel enormously hopeful. If I was only going off what I saw online, I’d probably agree that everyone who wasn’t vaccinated is being selfish and difficult. But talking to people like those church groups has changed how I feel completely. Often, I see an entire family on the other side of the screen—kids and grandparents. People come. They come in groups. They’re willing to be vulnerable. They have questions. And their questions are all ones we have answers for. It’s not undoable. from https://ift.tt/36V9UM9 Check out http://natthash.tumblr.com At a county health department near my hometown in rural Arkansas, almost everyone who comes in for a COVID-19 test is congested and short of breath, with a sore throat and muscle aches. They might have the flu, except for the added telltale symptom of this coronavirus: the loss of taste and smell. Many of the patients now are younger than those in previous months; a nurse who works there told me she saw two cases of young children in one day. (The Atlantic agreed not to name the nurse, because, as a state employee, she is not authorized to speak with the media.) Even worse, though, is that almost every potential case she saw was avoidable. Almost none of the eligible adults she tested had had one of the vaccines. Arkansas has one of the lowest vaccination rates in the United States, and one of the worst case rates for COVID-19. Our neighboring states--especially Missouri—are seeing similar trends. Case counts have been increasing at the highest rates since February, and we have the most new cases per capita in the nation. On Monday, we saw the highest single-day increase in hospitalizations, 79 new patients, of the entire pandemic. Test-positivity rates are also high, suggesting that infections are undercounted. In my county, Van Buren County; in the more rural Searcy County to the north; and in the more densely populated Faulkner County to the south, the daily case totals are, respectively, 119 percent, 142 percent, and 191 percent higher than their averages over the previous two weeks. Because new cases show no sign of slowing down, we likely have more illness ahead. My local Facebook feed has again become a steady stream of families asking for prayers and making announcements for memorial services. The nurse at the health department told me that she and her co-workers had expected that some people would resist vaccination, but that “seeing that resistance persist despite education, despite outreach” had left her and her colleagues depressed and downtrodden. “Why are they not understanding how this is putting people’s lives in danger?” she asked. Like her, I’ve been haunted by this question. Sixty-two percent of my neighbors remain unvaccinated for complicated, interrelated reasons that map onto existing, bitter divisions. Any solutions, equally complicated, will likely come only after we’ve seen more death. I had expected some amount of vaccine hesitancy in my hometown, a small place of about 2,500 residents, called Clinton, on the southern edge of the Ozark Mountains, because of the way this pandemic has unfolded from the beginning. Although schools and many restaurants temporarily shut down here, my region is full of people who have been reluctant to wear masks, stay at home, and otherwise adapt to new recommendations from health authorities. Big stores such as Walmart enforced mask wearing, but many smaller establishments didn’t. Many schools went partly remote, but ball games continued. The community seemed split between people who were taking the pandemic seriously and people who thought the disease was a hoax, or no worse than the regular flu. That split remains today, as unvaccinated people continue to go about their life as if this pandemic never happened, even as the Delta variant’s presence makes the virus as dangerous as ever. Those of us who rushed out to get vaccinated feel personally safe but remain cautious. Persisting in this contradiction can seem like living in the distorted reality of a fun-house mirror, as we watch those least protected from the virus take the most risks, likely ensuring the disease’s continued spread. My small county has had 24 COVID-19 deaths throughout the pandemic, and statewide that number has passed 6,000 (for comparison, in recent years, flu deaths ranged between 620 and 720). News of these deaths trickled out among friends and family—I found out about a former teacher’s death because of a group email. We haven’t set aside a time to mourn the community’s loss together, and we haven’t had a COVID-19 memorial. Unlike my friends who live in Washington, D.C., and New York City, I never experienced nights filled with the sounds of sirens, and many of my neighbors never saw the death and devastation up close. The virus spread primarily through family networks because people continued to see their families, but rural life can be atomized and isolating. That kept us from feeling the full force of the pandemic’s effects, and also provided a small amount of protection from the disease itself. Now the virus’s increased ability to spread, hitting just as we’ve reopened, has finally collapsed that rural space. Suddenly, we’re racing against time, trying to get more and more people vaccinated before hospitals become too full and start turning patients away. The strain on health-care facilities is especially worrisome in rural areas, which have few hospitals and ICU beds. Our most serious medical cases are typically sent to Little Rock, and on Saturday, the University of Arkansas for Medical Sciences announced that its hospital, a public facility ranked among the best in the state, was full. During last year’s relative isolation, more people went online, especially to Facebook, for socialization and information; today, that is where the vaccines’ loudest opponents announce why they’re not getting the shots. People I know seemed concerned about the fact that the vaccine was approved only for emergency use. They also believe that people have died from the vaccines in large numbers, that the vaccines themselves have caused illness, that they’re responsible for the Delta variant, that they’re made with fetal tissue from aborted babies, that they alter your DNA, that they cause infertility, that the government’s eagerness to offer incentives for vaccination is suspicious, and that because the vaccines are new, their use amounts to a government experiment on the citizen population. There is some understandable distrust of the pharmaceutical industry because of the U.S. opioid epidemic, and of the government because of this country’s history with medical racism. Every vaccinated friend of mine who has tried to champion vaccines to the disbelievers said they end up sad, disappointed, and frustrated, caught in circular arguments that rely more on ideology than facts, and in which every piece of evidence is taken as more proof of conspiracy. More often, the reasons people give for skipping vaccination are less extreme and more personal. Last Tuesday, I met up with Courtney Patrick, my partner’s co-worker at a medical-cannabis facility. She had just received her first dose of the Moderna vaccine. She is 31, and had avoided vaccination until last week because she doesn’t like needles, and because she wasn’t very concerned about contracting COVID-19. “I still have that false sense of ‘I’m young; I’ll be okay,’” she said. She knows that this isn’t exactly true, because the flu made her very sick three years ago. In her previous job, Patrick worked as a veterinary technician (she still rescues turtles in her spare time), preaching to patients that they should get their dogs and cats vaccinated every year. She knows that vaccines work and believes in them. The push she needed to overcome her fear came from her family. Patrick’s grandmother was diagnosed with breast cancer, and will need help with errands—plus, Patrick wants to be able to visit her grandmother without putting her at risk, which she couldn’t do without getting vaccinated. Before that, she said, “it was just low on my list.” And nothing around her signaled that that should change. The state has been treating the pandemic as though it’s essentially over. Restaurants were allowed to resume operations at full capacity in February, our mask mandate was lifted in March, and the pandemic unemployment-assistance programs ended on June 26. Although the governor, Asa Hutchinson, still gives regular COVID-19 briefings and encourages people to get vaccinated, we lost a sense of urgency just when we needed it most. In this context, getting vaccinated has meant acting on our own volition. Although every county has a walk-in center for free vaccines, many are open only during business hours on weekdays, and they’re located in population centers. Two of the three biggest clinics in our county are located here in Clinton—it’s the county seat. From the rural outreaches of the county, the trip can be almost an hour each way. In elderly and low-income rural populations, many people are unable to drive or do not have regular access to a working car, and our county hasn’t made a widespread effort to take mobile vaccination sites out to community centers, churches, or firehouses. Deborah Shoenberger Brennan, a retired veterinarian who volunteered with the county’s wellness committee—which was disbanded last year to avoid meeting during the pandemic—thinks we need them. “We veterinarians, we go out into the whole county to, like, 12, 15 different stations … to vaccinate for rabies. I’d like to see our public-health professionals or our doctors or physician assistants do that,” she told me. Making vaccinations easier might pull in some people who are simply hesitant because of inertia, like Patrick. The Delta variant’s threat is also pulling a few more people in. On Thursday, a pharmacist in Clinton, Marinda Bryan, who has been vaccinating patients since the shots became available, said on a local radio show that she’s now seeing 10 to 15 people coming in every day for their first dose. (On Friday, the state health department reported its largest daily dose total since May 21.) Bryan said many people falsely believe that the vaccines cost money, but more people arrive with medical misinformation. She and her staff have been able to allay their concerns in most cases. At her pharmacy, all customers are reassured that they are free to make their own choices, but are also asked whether they’ve had a COVID-19 vaccine. If they have not, they get a reminder: It’s always available. Still, how many people will keep resisting, no matter what? If people also resist mask wearing or other public-health mandates, the idea that getting the vaccine is a matter of personal choice takes on a different valence. “Your choice is your choice, but you don’t have the freedom to force your choice on other people,” Shoenberger Brennan said. For the 33 percent of people in our county who have already been fully vaccinated, living with that tension has been frustrating: Many of us feel that our neighbors are continuing to put others in danger. Breakthrough cases among vaccinated patients are rare—nationally and in the state, more than 99 percent of current deaths are among the unvaccinated—but they’re more common in populations with high numbers of unvaccinated people. Those of us who were vaccinated early have reluctantly begun wearing masks in stores again. “If something doesn’t change, I will never be able to leave the house!” a friend, Lisa Ray, who is a professor at the University of Central Arkansas, told me. Courtney Patrick thinks more people won’t be moved to get the vaccine until a health problem affects them personally, like her grandmother’s cancer did her. One Arkansas mother named Angela Morris was interviewed by the Little Rock CBS affiliate, THV 11, from Arkansas Children’s Hospital, where her 13-year-old daughter had been on a ventilator because of COVID-19 for 12 days. That day, the children’s hospital had six other pediatric COVID-19 patients, two of them on ventilators. (By Tuesday, the children’s hospital said it had 12 COVID-19 patients.) “I just want people to get their kids their shots. Everybody just needs to get the shot. It’s a much better route than the one we’re in,” Morris told the station. But I’ve seen other cases in which personal tragedies haven’t changed anyone’s mind. A friend forwarded me a message from a new COVID-19 widow preparing to bury her middle-aged husband. “I truly believe God has had our time planned for a long time before that day comes,” she wrote. “If you are meant to go, you will despite anything you try to prevent it.” Many white evangelicals had already begun to shun vaccines altogether, and part of their rationale is this sense of predestination. The message of these anti-vaxxers builds on a basic idea: God built your body, and the immunity that nature gave you is better than any medicine. Sometimes, doctors repeat these messages. Bryan, the local pharmacist, told me that two doctors in our hometown are not discouraging their patients from getting the vaccines, but they are also not advocating for them. Some are more blatant in their opposition—Amy Beard, who practices telemedicine and is licensed in the state, has been outspoken about treating COVID-19 patients instead with medication typically used to prevent heartworms in dogs, cows, and goats. On her Facebook page, she called the shots “mutant factories,” in response to comments about the vaccines creating variants. Someone who had recovered from COVID-19 in January asked her about “natural” immunity; Beard responded, “Before Covid, natural immunity was the BEST immunity. And it still is.” For the nurse at the county health department and other health-care professionals, this strain of resistance began with President Donald Trump and has been the hardest to fight. “I think that this would be a totally different story had it been addressed appropriately in 2020, at the very beginning,” the nurse told me. When Trump and other leaders questioned health professionals and epidemiologists, those uncertainties led more people to feel empowered to question them as well. Individual reasons for avoiding vaccination keep shifting—whatever it takes to stay on that side of the political divide. Meanwhile, the rest of us have to reckon with what it means that so many of our neighbors have been reluctant to act in the public good, and what that augurs for our sense of community, now and whenever this is over. from https://ift.tt/3kCL4ZH Check out http://natthash.tumblr.com When Kishana Taylor welcomes her twins into the world this December, she’ll be pretty confident that they won’t be carrying the virus that causes rubella, an infection that can be disastrous in infants. Thanks to a vaccine she received as a child, Taylor, a virologist at Carnegie Mellon University, is still immune to the pathogen decades later. She was able to confirm that in June through a simple test that searched her blood for antibodies that recognize the rubella virus, and then added them up. If her antibody counts were above a certain level, called a correlate of protection, she and her babies would be considered well shielded from disease. “You are considered immune with a titer of 9.9 to rubella,” she tweeted last month, referring to her antibody levels. “My titer? 116. I love my immune system sometimes.” The term correlate of protection doesn’t exactly roll off the tongue, but it’s one of the sexiest concepts in the field of vaccinology. Correlates are biological benchmarks—measurements of a single immune molecule or cell—that can show that a vaccine is achieving its desired effect. With a correlate in hand, researchers can confirm how well a shot is working and identify the rare individuals in whom it doesn’t take; they can suss out the need for boosters and fast-track the development of new vaccines. At their most powerful, correlates of protection boil down the complexities of an immune response to a single value—one that can confidently affirm that a person won’t get infected or seriously sick. “It’s kind of a magic number,” Ali Ellebedy, an immunologist at Washington University in St. Louis, told me. “It’s the big holy grail,” Emory University’s Sri Edupuganti says. “It’s what we dream about,” Cornell’s Sallie Permar told me last month. In recent weeks, the correlate community has been buzzing louder than ever. Scientists are on the cusp of confidently defining some correlates of protection against symptomatic disease for the COVID-19 vaccines. If confirmed, these correlates could revolutionize the way we tackle SARS-CoV-2 immunization: Vaccine makers testing a new inoculation may no longer need to follow tens of thousands of people for many months to test their product’s protection. Instead, they could inject just a few hundred people, snag some drops of blood, and see if the elusive correlate is met. That’s how we tee up new flu vaccines every year without the rigmarole of gargantuan clinical trials. But for all their apparent simplicity, correlates of protection are devilishly hard to come by. Try as researchers might, capturing the oomph of vaccine-induced immunity in one number—or several—isn’t always possible. Even as scientists chase them, correlates are a reminder of just how inscrutable our own bodies can be. Even our best vaccines start out as educated guesses. Researchers study people who have recovered from a particular infection, and then try to cook up an inoculation that will prompt protection that’s similar to or better than natural immunity. What ends up entering people is simple—a harmless pantomime of the pathogen. But it leads to a tortuously complex response that marshals the immune system’s many defensive players, including antibodies, B cells, T cells, and more. Finding a correlate means cleaving a single variable out of this mess to act as an envoy for the rest of the immune system. That’s a heavy lift for a single cell or molecule, especially when people react in such different ways to the same pathogen. And not all immune responses can be easily measured. Some of the vaccines we’ve been using for decades still don’t have a concrete correlate, including the shots for mumps, rotavirus, and tuberculosis. That probably won’t be the case for the COVID-19 vaccines. Since the pandemic’s early days, experts have had their eyes on neutralizing antibodies, sometimes nicknamed “neuts,” which can glom on to the outside of viruses and block them from entering cells. Neuts that recognize the coronavirus teem in the bodies of people and laboratory animals that have successfully fought off coronavirus infections. The molecules’ disease-fighting powers have made them the workhorses of antibody-based treatments, such as convalescent plasma and monoclonals. Levels of these neuts also soar after vaccination, and seem especially high in people who don’t come down with COVID-19 after getting all their shots. By now it’s clear that neut numbers do correspond pretty well with protection—the more neuts someone has, the more likely it is that they’re safe from disease. “As far as I’m concerned, the data are clear,” Stanley Plotkin, a vaccine expert at the University of Pennsylvania, told me. “Neutralizing antibodies are it.” Establishing that this trend exists, though, isn’t the same as zeroing in on a cutoff for protection, above which most vaccinated people would likely be guarded from illness. “We know lower neutralizing titers predict more infection,” Taia Wang, an immunologist at Stanford, told me. “What we’re looking for now is a little more precision.” To suss out a more specific set of numbers, researchers need to repeatedly sample the blood of shot recipients, some of whom have to get sick so researchers can get a sense of what falls below the threshold they’re looking for. “The more breakthroughs you have, the easier it is to determine,” Katy Stephenson, a physician and vaccine expert at Beth Israel Deaconess Medical Center, in Boston, told me. A great irony of vaccinology is that it’s easier to define the success of a vaccine that’s prone to regularly fail—one of the only downsides of our extraordinary shots. Another hurdle that correlate chasers need to clear is a lack of consistency across vaccine trials, which were conducted at different times in different populations using different inoculation recipes, different criteria for defining COVID-19 severity, and different brands of antibody tests. Aggregating and analyzing all the evidence to produce one unifying correlate requires some serious statistical gymnastics. By now, though, enough people have been vaccinated, and enough blood samples drawn, that preliminary numbers are starting to emerge. One group of researchers in the United Kingdom has proposed a correlate of protection against COVID-19 for AstraZeneca’s vaccine; two others, one in Australia and another in the United States, have taken a stab at pinpointing measurements that will hold true across several different shots, including the three available to Americans. (Representatives from Moderna, Pfizer, and Johnson & Johnson told me that they didn’t yet have their own correlates to report, but were continuing to investigate.) But the case isn’t closed. “We have some strong leads, but I would not say we have a correlate yet,” Holly Janes, a biostatistician at the Fred Hutchinson Cancer Research Center, in Seattle, told me. While neuts have certainly hogged the spotlight so far, they could still be unseated by another molecule or cell. And even if neuts are the real deal, having one correlate doesn’t preclude defining another that captures an additional element of the immune system. Flu vaccines, for instance, seem to come with a bunch of measurable metrics of success, some of which are still being confirmed in research labs. Other, non-neutralizing antibodies exist, and their levels also seem to ratchet up in lockstep with COVID-19 vaccine efficacy. Many researchers are hoping for more data on T cells, immune cells that support the production of antibodies or annihilate virus-infected cells on their own. Compared with antibodies, T cells are fragile, reclusive, and a pain to measure, Smita Iyer, an immunologist at UC Davis, told me. But they seem fundamental to the success of well-established vaccines, including those for chicken pox and tuberculosis. Against the coronavirus, T cells are known to pick up the protective slack when neuts and other antibodies fail. “There’s not only one immune response that protects you, which is good,” Florian Krammer, a vaccine expert and virologist at the Icahn School of Medicine at Mount Sinai, told me. “If one fails, another can take over.” That redundancy is great for us, but frustrating for researchers looking for a simple portrait of protection. Things could get even thornier. As is the case with any vaccine, the success of a COVID-19 shot hinges on a multitude of factors—including the strength of the immune system it’s bolstering, the mutability of the virus it’s counteracting, and the exact ingredients in the shot itself. Kids, whose immune systems are still finding their footing, might need correlates of their own; so might older adults and immunocompromised people, whose immune systems are less easily marshaled by vaccines. The numbers we settle on could also vary among vaccine brands because different shots rile up different subsets of immune cells. Then there’s the biggest wild card of all: the coronavirus itself. It’s continuing to splinter into new variants, some of which have already revealed themselves to be quite capable of dodging certain antibody-based defenses. A neut level that keeps us safe from Alpha won’t necessarily thwart Beta or Delta to the same extent. (There’s at least good news on T cells, which are much harder to stump with mutations—another reason these cells are looking so attractive to some scientists.) “We’re starting to get numbers now, but there are going to be asterisks because of the variants,” Lisa Gralinski, a virologist at the University of North Carolina at Chapel Hill, told me. Because correlates take so long to determine, “whatever number we come up with today is really talking about the past,” Stephenson, of Beth Israel, said. SARS-CoV-2 will always mutate far faster than humans can conjure new correlates. We may well end up with an entire menagerie of correlates against COVID-19, each tailored to its own combination of population, variant, and vaccine. (And that’s all just in the realm of blocking COVID-19 disease; stopping asymptomatic infection would require its own set of correlates as well.) But the mere possibility of hitting protection pay dirt is reason enough to keep plugging away. Having a strong correlate of protection against COVID-19 would allow researchers around the world to more quickly bring new vaccines to market in countries where they are sorely needed. A correlate would also give scientists the chance to monitor the natural wane of immune responses and deploy boosters that could rapidly buoy those defenses, if need be. It could act as a guidepost for new shots that fight specific variants before they outsmart the jabs we already have. The need for correlates is so urgent, the FDA has already gambled that antibodies are the answer: In recent guidance, the agency noted that it would consider green-lighting updated, variant-specific versions of vaccines if they’re able to prompt the production of adequate levels of neuts. It’s a hastier move than some researchers would like. But with variants such as Delta surging amid a largely unvaccinated global population, the shortcut offered by these correlates has never been more appealing. The big hope, researchers told me, is that COVID-19 vaccines will be able to follow in the footsteps of flu shots, which are reformulated seasonally to keep pace with the strains du jour. Vaccine makers can debut new vaccines by simply checking inoculated people’s blood for the telltale markers of protection, rather than waiting to see how these individuals fare against the virus itself. Spinning the idea of correlates into a personal guarantee of immunity is tempting, especially with antibody tests so readily available. But correlates are just that--correlates--patterns gleaned from large groups of people. Levels of certain immune fighters could track with protection against disease without being directly responsible for our vaccines’ success on a person-by-person basis. “We’re talking about measurements that apply better to populations than to individual people,” Plotkin said. Some correlates can be tested in individuals, such as in the case of the rubella-antibody test that Taylor took in June, after discovering she was pregnant. But these tests don’t offer absolute certainty. Every trend will have exceptions—some people whose SARS-CoV-2 antibody levels are bonkers-high may still end up getting sick; others with low titers will stay safe. Antibody stocks, after all, naturally dwindle over time, but the body retains the ability to replenish them. Thresholds aren’t hard lines between unprotected and protected; everyone always carries some relative risk, especially amid a pandemic this devastating. “There are no sharp edges in biology,” Iyer told me. Correlates, while useful, can’t actually encompass everything our immune systems are capable of. Without the right amount of nuance, they risk making black and white out of a situation that operates entirely in shades of gray. from https://ift.tt/2TsFM7W Check out http://natthash.tumblr.com America’s vaccination rates have fallen off a cliff, and nothing seems to help. On June 2, President Joe Biden announced a frantic plan to reverse what already seemed to be an awful, exponential slide: At the peak of the country’s vaccine rollout in mid-April, almost 3.5 million doses were being put into arms every single day, but that number had quickly dropped by half, and then by half again. Biden’s “month of action” came and went, and nothing really changed; or rather, the situation kept on changing for the worse. Demand for vaccinations shrank in July, as it had in May and June. Even statewide vaccination lotteries, described here and elsewhere as a great idea, had turned out to be a flop. [Read: America is now in the hands of the vaccine-hesitant] With every passing day, the pace of vaccinations only seems to drag a little further toward the gutter. As of July 12, it had fallen off by half again. The Great Vaccine Decline now appears to be an ugly force of nature. If it continues, further horrors are all but guaranteed to follow. Sadly, those horrors may be the only thing that stops it. The problem, it’s been said, is that we live in two Americas, riven by both ideology and immunology: In blue America, vaccination rates are standing up just fine; in red America, they’re slouchy and exposed. Indeed, the latest vaccine numbers show that 17 states have now provided at least one dose to more than 60 percent of their population—and every single one of them voted for Biden in the last election. Another 16 states are struggling to reach a rate of 50 percent; all but one of those went for Donald Trump. But there’s another, better way to think about what’s happening here: If the distribution of vaccines keeps slowing down, it’s not because America is divided but because we’re running out of people who think vaccines will save their lives. [Read: America’s vaccine future is fragmenting] It certainly hasn’t helped the vaccination drive that Fox News and other right-wing outlets are sewing fear about the safety of the COVID-19 shots, and about the efforts to distribute them. Still, the recent wave of right-wing propaganda hasn’t clearly made the problem worse. Going by the numbers that we have so far, Tucker Carlson’s summer monologues aren’t really changing many minds. In fact, enthusiasm for the vaccine has been growing, overall, in both Americas alike. According to the Kaiser Family Foundation, which has been carefully following vaccine attitudes and behaviors since December, almost half of Democrats were saying that they planned to get immunized as soon as possible (if they hadn’t done so already) at the end of 2020; by June, that rate had nearly doubled, to 88 percent. Republicans started from a lower baseline, but they’ve also gotten more accepting: Just like the Democrats, the proportion saying that they wanted the vaccine almost doubled over time, from 28 percent to 54 percent. Party rhetoric notwithstanding, the overall partisan gap in vaccine enthusiasm has been holding steady, at a little more than 30 points, through all of 2021. Rather than diverging politics, people’s willingness to get vaccinated might best be understood as a function of how they perceive risk. Although there are more noble reasons to be immunized than self-protection, surveys show that they’re not the ones most often cited. Kaiser finds that among those who have gone in for their shots, more than half say the “main reason” was to reduce their personal risk of illness. Meanwhile, among the unvaccinated, one-half assert that COVID-19 case rates are now so low that further vaccinations are unnecessary. Risk perception is just one of many factors that determine vaccine uptake. You could be terrified of getting COVID-19, for example, and desperate to be immunized, but still find yourself unable to reach a distribution site. A person’s sense of danger could also modulate these other factors, at least for some people: The time and effort that it takes to get vaccinated may matter less to those who worry more. [Read: The fundamental question of the pandemic is shifting] Risk certainly seems to help explain the other major gap in vaccination rates across the U.S. population, between the gray America of retirees and the green one of Millennials. Some 85 percent of seniors have now been vaccinated, versus 55 percent of young adults—a gaping, 30-point spread that matches up, almost perfectly, with the spread between Democrats (86 percent) and Republicans (52 percent). If these two Americas of old and young are making different choices about vaccines, it can’t be just because they’re watching different cable talk shows, or because they vary in their trust in institutions, or because they disagree about the legal merits of Jacobson v. Massachusetts. No, old people are much more likely than young people to get their COVID-19 shots because old people are much more likely to die from the disease, and they know it. The same pattern holds for uptake of the flu shot every year: Seniors, who are at the greatest risk of influenza, are much more likely to be immunized. (The age gap for the flu shot, like the one for COVID-19 vaccination, is roughly 30 points.) Since the very start of the pandemic, Republicans and Democrats have differed widely in their sense of the virus’s dangers. From March of 2020, the Pew Research Center has been asking American adults whether the coronavirus outbreak represents a “major threat to the health of the U.S. population as a whole”—and from March of 2020, Democrats have almost always been about twice as likely to say yes. In May last year, 82 percent of Democrats agreed that it was a major threat, compared with 43 percent of Republicans. Politicians were working hard, from March of 2020, to shape those very perceptions among their constituents, and it worked: The partisan worry gap was in place long before any vaccines were ever tested, and long before the right-wing media started talking up the risks of deadly side effects. It hasn’t budged for months and months and months. [David A. Graham: It’s not vaccine hesitancy. It’s COVID-19 denialism.] Differences in risk perception are not as clearly linked to other important (and somewhat narrower) vaccination gaps, such the one between Black and white Americans. But looking at the numbers overall, you can see some hints of how these factors might have played out into the timing of America’s Great Vaccine Decline. It’s clear enough that vaccinating people drives down the spread of COVID-19: Over a period of about six-months, the number of new cases recorded every day in the U.S. has dropped by 95 percent, while the number of Americans who have been fully vaccinated increased a hundredfold. But the effect might also go the other way, with a decline in COVID-19 cases driving down the rate of vaccination. On March 11, Biden announced a huge expansion of the vaccine rollout, and over the next month, the number of doses being given out per day increased by 25 percent. But case rates were increasing too, by about the same amount. Then, around April 12, both trend lines hit a ceiling: From that point on, fewer Americans were getting sick, and fewer were getting vaccinated. By the end of June, both rates had fallen off by more than 80 percent. 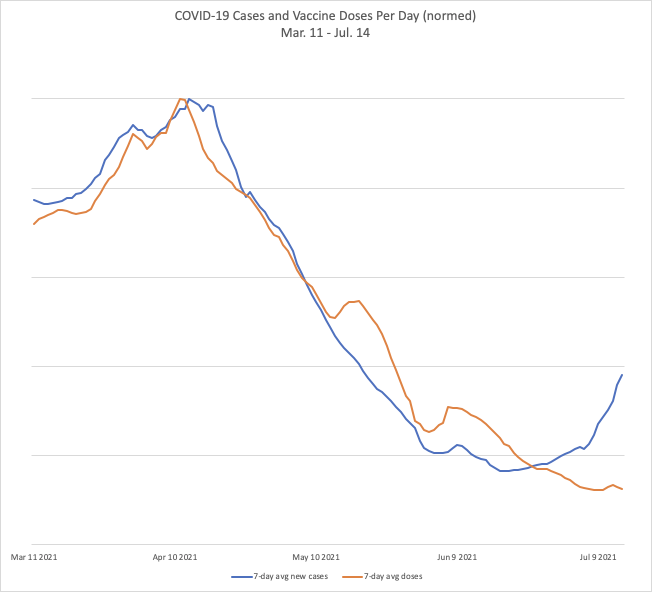
It’s not surprising that demand for vaccination would tend to fall off over time, given that the most enthusiastic people line up first. Once they’ve gotten all their doses, the pace can only slow. But the coincidental timing of the drop in case rates hints that people’s sense of risk could be a factor too. Imagine that you’re not so sure about getting the vaccine yourself, and then you hear that the pandemic is receding. Maybe that makes you somewhat less inclined to take the day off work and find a mobile clinic. Maybe it’s a reason to wait a little longer. “One of the main problems that vaccination programs face is that they’re effective,” Noel Brewer, a psychologist who studies health behaviors at the University of North Carolina, told me. “And their effectiveness undermines people’s interest in vaccination.” If our sense of danger—or lack thereof—is behind the Great Vaccine Decline, then maybe there’s a fix. Should we try to make the holdouts more afraid? Scared Straight programs for vaccines have been tried before, and they haven’t done much good. Studies tend to find that pointing to the dangers of disease will certainly freak some people out—but that feeling is short-lived and doesn’t seem to change behavior. “They found small increases in perceived risk but no increases in vaccine uptake,” Brewer said. “On balance, it’s not going to work.” It’s also possible that some people who are disinclined to get their COVID-19 shots might not be wrong, per se, in their assessment of their own, relative risk of dying from the disease, even if they’re neglecting the bigger picture. Young people really are hundreds of times less vulnerable than seniors, and Republicans are, on average, a lot more realistic than Democrats about a person’s chances of developing severe disease once they’ve been infected by the coronavirus. (At the same time, they’re much less realistic about COVID-19’s harms in aggregate.) In other words, efforts to scare more young people or Republicans into getting vaccinated could end up encouraging them to be less informed about the facts, at least narrowly construed, instead of more so. [Read: Delta is driving a wedge through Missouri] Brewer warns that any form of intervention aimed at people’s “thoughts and feelings” about vaccines isn’t likely to succeed. We know that those thoughts and feelings help determine people’s actions, but that doesn’t mean they can be changed by PSAs or other public-health campaigns. It’s better to focus on behavior, he told me. “We have to help folks take action; we have to help them take time off work; we have to help lower the barriers that are currently preventing them from acting on their good intentions.” It’s important for people’s own doctors to be involved in the process, encouraging and delivering vaccines, Brewer said. Vaccine requirements might make a difference. Full FDA approval for the vaccines could help, too—though how much is debated. Of course, helping folks take action is just the sort of thing that the White House has been pushing, and they haven’t done much good. Brewer acknowledged that the effects have been pretty small so far, but he said that doesn’t mean they’re unimportant. Changing people’s health behaviors tends to be slow and difficult work. “When looking at other vaccines, an increase of 2 percent year over year is a big deal,” he told me. Even tiny bumps like these save lives. But as the Delta variant rips through Arkansas, Florida, Missouri, and the rest of the United States, we may see the vaccination numbers start to rise in tandem. If a drop in cases dampened people’s urge to get vaccinated, then perhaps a surge in cases will do the opposite. If ICUs keep filling up, and COVID-19 deaths increase again, then a growing sense of danger may envelop some among the vaccine-hesitant, nudging them toward action. It’s a pattern that we’ve seen before: In 2019, when measles struck parts of the Pacific Northwest, local rates of measles vaccination tripled in response. The economist Emily Oster has looked at pertussis outbreaks, county by county, going back to 1991, and found that child vaccination rates increased in the years that followed. The two lines plotted on the chart above, for new COVID-19 cases and vaccine doses, have started to diverge. It will be a somber consolation if they come back together in the weeks ahead. A national month of action did little to arrest the Great Vaccine Decline. Now a national month of pain and suffering is all we have. from https://ift.tt/3zihqNg Check out http://natthash.tumblr.com |
Authorhttp://natthash.tumblr.com Archives
April 2023
Categories |
 RSS Feed
RSS Feed

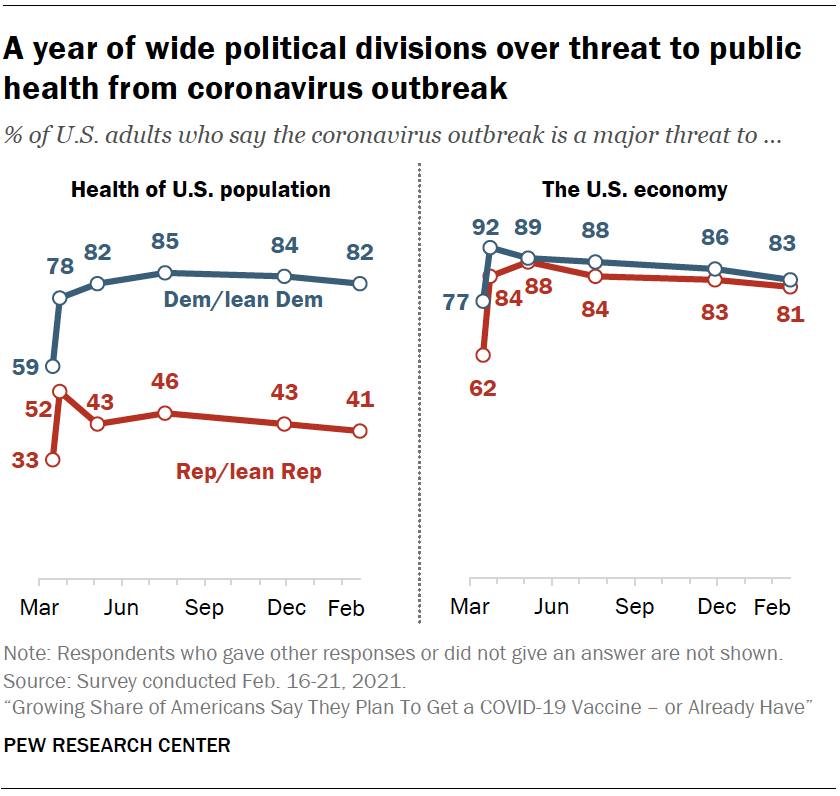{kind=link}
{kind=link}