|
The human brain makes decisions in two basic modes. One is analytic, which involves carefully weighing costs and benefits and choosing the best option. The other mode is intuitive: doing what feels right. Both have their merits. Intuitive thinking allows us to make split-second decisions. It helps guide our romantic lives and our lunchtime sandwich choices. But it is not the mode that should inform a strategic response to a pandemic. Even casual observers of President Donald Trump’s mode of thinking long ago abandoned hope that he might embrace analytic reasoning (sometimes referred to simply as “science”). But if there were ever a possibility that he might at least come to terms with the power of the coronavirus, it would have been when it sent him to the hospital. Barely a month ago, recall, we had cause to speculate that the president might soon be dead. Although details of Trump’s illness remain concealed—including abnormalities in his chest CT scan and the date that he first tested positive for the virus—the known facts of his case indicate that it was not mild. He received supplemental oxygen to keep his red blood cells saturated, and he was prescribed dexamethasone, which is recommended only in serious cases. Many patients emerge from illness having had a come-to-Jesus moment that reorients their thinking. Former New Jersey Governor Chris Christie, for one, issued a mea culpa last week after he was discharged from a COVID-19 hospitalization that included a week in the intensive-care unit. “When you get this disease, it hits you how easy it is to prevent,” he wrote under the headline “I Should Have Worn a Mask” in The Wall Street Journal. “We are asked to wear cloth over our mouth and nose, wash our hands and avoid crowds. Seldom has so little been asked for so much benefit.” Trump had no such revelation. Instead, in the weeks since his illness, he has escalated from downplaying or neglecting the virus to outright denialism. After returning to the White House and sanctimoniously removing his mask, he has centered his reelection campaign around the notion that the pandemic is over. “With the fake news, everything is COVID, COVID, COVID,” he said at an Omaha, Nebraska, rally this week. “I had it. Here I am, right?” He cited the illness of his son Baron—who contracted the virus shortly after his father tested positive—as being extremely mild. He did not mention the first lady, Melania, who described having COVID-19 as “a rollercoaster of symptoms,” the experience of which “gives you a lot of time to reflect” and reminded her of the need for “compassion and humility.” At a few points in the pandemic, Trump displayed these qualities. He regularly stood beside the doctors on his task force, such as Anthony Fauci and Deborah Birx, and nodded as they warned that this disease is indeed serious (even if he contradicted them later at rallies, and ignored their recommendations about masking). Now, Trump has taken to mocking social distancing and pushing a conspiracy theory wherein the basic facts of people dying are an attempt to hurt him. He has accused doctors of exaggerating the disease, and vilified them as enemies in his crusade to return to “normal,” even as the daily death toll has topped 1,000 people in recent days. [Read: The pandemic is in uncharted territory.] To look on, inert, as Americans suffer and die is one thing; to deny that it is happening is another. This is a clear and ominous glimpse of how the pandemic will continue to play out if Trump remains in power. During America’s final lurch into the election, the president has become an even darker caricature of himself, laying bare his willingness to abandon Americans’ health and well-being for his own self-preservation. He is now even more dangerous as a vector of disease than when he was actively shedding the virus. On Wednesday, Brett Giroir, an assistant secretary of health and human services, appeared on the Today show and made the rare move of directly contradicting the president’s claims. “The cases are actually going up,” he said. “They’re real.” When a public-health official has to go on TV to debunk a conspiracy theory, it is not typically one that originated with his boss. But Trump has embraced the bizarre idea in recent days that doctors are inflating case numbers for profit. He has also repeated his old standby lie that the counts are increasing simply because of more testing throughout the country. Giroir clarified that in fact it’s not just the case numbers that are rising, but the numbers of people who are hospitalized and dying each day. He held up a mask and implored Americans to wear one. To suggest anything less in this moment seems unconscionable and unimaginable. In the past week alone, more than 5,000 Americans have died of COVID-19. The country is on pace to experience some 400,000 excess deaths this year, directly or indirectly attributable to the pandemic. The virus’s global surge this month has compelled leaders across Europe to order curfews and lockdowns. Trump, meanwhile, has been crisscrossing the country and holding mass gatherings. He has continued promising that we are “rounding the turn.” Although in the past he has recommended that people wear masks, in recent weeks, he has repeatedly, falsely claimed that masks are ineffective and that experts are divided over their use; he has even implied that they spread the disease. [Read: How we survive the winter] Trump is no longer simply undermining the voices of his own experts, but baldly urging people to disregard them. According to Fauci, Trump has not met with the task force in months. He has taken to mocking Fauci as weak, fixating on his ability to throw a baseball and his outdated early statements about masks. The president has berated and undermined Robert Redfield, the director of the Centers for Disease Control and Prevention whom Trump himself appointed. He has attacked his election opponent, Joe Biden, by saying, “He’ll listen to the scientists,” as though this were an innately bad thing. By failing to encourage prevention, Trump has all but guaranteed that many state and local officials will have to order shutdowns. At the same time, Trump has left many Americans without the economic stability or political will to close businesses in any unified way, as many places did in March. No bailout package is forthcoming from Congress, and unemployment insurance is running out in many states. The president is supporting a lawsuit that would overturn the Affordable Care Act and cause millions of people to lose their health-care coverage. Insofar as Trump addresses the virus itself, it is to insist that he deserves praise for implementing a travel ban in March, saying he “saved millions of lives.” (The move was prudent, but its impact was probably modest.) He has promised imminent “cures” that do not exist. He has lied about the availability of a vaccine, again and again. The cumulative effect has been the dilution of crucial public-health messaging. Trump is known to use an approach called censorship through noise: a suppression of truth by making ever more bizarre claims. But the extremity of his recent tack is jarring even for a president who has all along insisted on calling it “the China virus” and who has consistently promised that it was “going away.” As the facts accumulated to confirm his wrongness, he has only committed harder to the lies—to sowing confusion to distract from his failures. For the past four years, psychologists and psychiatrists have attempted to fit Trump’s behavior into a diagnosis. They note his textbook disconnection from reality and from the consequences of his decisions as they affect other people. Many have settled on various personality disorders: Narcissistic, antisocial, and borderline have been the most common. Even to the dispassionate scientific mind—the clinicians usually indisposed to weigh in on political matters, attempting to be as objective as possible—Trump can seem to fit the criteria as if the disorders’ Diagnostic and Statistical Manual entries had been written to describe him. But none of the diagnoses stuck. The clinical labels that initially felt so transgressive to apply to a sitting president have lost their gravitas through overuse. Petitions bearing hundreds of signatures from mental-health professionals deeming Trump cognitively unfit for office and a danger to the global population led to no practical end. The extreme abnormality of his behavior faded into simply Trump being Trump. He developed immunity to condemnation by way of lowered expectations. A numbness to Trump’s behavior has emerged again and again, in response to issues like his undisclosed tax returns and the numerous sexual-assault charges against him. Many Americans have become so weary as to tolerate Trump’s denialism as normal regarding public-health emergencies like climate change and gun violence. Now it is happening with an actively spreading and deadly infectious disease. Our neurological capacity to be shocked depends on novelty. As that fades, anything can lose its feeling of absurdity or danger. This is partly for our own health; the stress of living in a state of constant incredulity would kill us young. But this adaptive, self-protective numbness also has the effect of training us to accept the unacceptable—the ridiculous counter-reality that Trump is attempting to construct. [Read: America is trapped in a pandemic spiral.] In any given moment, Trump’s behavior may seem confounding, vexing, self-defeating, unconscionable, unpredictable. But he is behaving exactly as he taught us to expect. In fact, what we know about Trump’s psychology might be understood through the lens of the coronavirus itself. He has met a foe that he cannot bluff into submission or wear down with insults. A virus is a physical force, like gravity or fire. It has no intention. It is not alive, and it cannot think. It can only react to its immediate environment. It can thrive only when it can invade functioning, living cells nearby. The virus forces entry and makes thousands of copies of itself and, having no further use for the cell, destroys it and abandons the remains. All of the flaws in Trump’s character and psychology have come to light through this virus. He reacts to immediate circumstances. He hijacks, pillages, and moves on. He has done this to America’s public-health institutions, which are wobbling and could topple under the continued weight of his negligence. He presides over a country where people are dying all around him, and he appears to see this only as a messaging issue. If Trump were to win a second term, he has made clear how this pandemic would play out. He is to have no moment of revelation. Americans would continue to die by the thousands. The president would devote his time and energy not to lowering that number, but to denying its existence. He has said the virus would disappear, and he would cling to that narrative regardless of the body count. If we joined him in this ignorance, the pathology would be ours. from https://ift.tt/2TFnmNJ Check out http://natthash.tumblr.com
0 Comments
During the first COVID-19 surge of the spring, the mantra was “Flatten to curve”—to buy time, using every tool available. Seven months later, it’s possible to measure what that time has bought: The death rate for COVID-19 has fallen dramatically. Hospitals in most places are not overburdened, and treatments are improving in many small but cumulative ways. In one study of patients hospitalized in a New York City health system, the adjusted death rate fell from 25.6 percent in March, at the pandemic’s onset, to 7.6 percent in August. This change cannot be explained by COVID-19 patients getting younger and healthier. The study’s authors adjusted the mortality rates for age and other risk factors. “People should take this as validation of all the hard work and sacrifices they have been making,” says Leora Horwitz, an internist and the study’s lead author. “It has made a difference.” Similar patterns hold throughout New York City and in the U.K., and they underscore the reason for flattening the curve. The longer we can prevent infections, the better prepared we will be to treat the people that might eventually get it. What was true about flattening the curve in March is still true now. As the U.S. faces a third coronavirus surge, Horwitz warns that “these numbers are not static.” We are still learning about how to treat COVID-19, and truly game-changing therapies have yet to arrive. When hospitals become overburdened—as they are starting to in El Paso, Utah, Wisconsin—death rates may rise again. The axiom from the beginning of the COVID-19 pandemic still applies today. “If I have to choose to have it, probably the later, the better,” says Sanja Jelic, a pulmonologist at Columbia University Medical Center. [Read: The pandemic is in uncharted territory] Jelic was among the doctors treating COVID-19 patients in New York in the spring, when hundreds of people were turning up at the city’s hospitals everyday unable to breath. Patients were crammed into hallways; doctors were overworked. Normally, Jelic says, she might have seen eight or 10 patients in a day. In April, she and two fellows were responsible for 60, any of whom might crash and need to be intubated. Lack of knowledge about the virus constrained what doctors did. Hospitals initially favored ventilation in part because doctors feared that high-flow therapy oxygen could aerosolize the virus and spread it to staff who didn’t have adequate supplies of personal protective equipment. (Now, of course, we know that the virus can be spread through aerosols generated from just normal talking and exhaling.) In some cases, aggressive intubation might have done more harm than good in patients who didn’t need it. Doctors stopped putting every patient on a ventilator once they realized the benefits of less invasive oxygen therapy and even turning patients onto their bellies, also known as proning. Because COVID-19 can, like many conditions, manifest so differently from person to person, knowing which patients might benefit—or be hurt—by a treatment is a key part of the learning curve. “There isn’t a one-size-fits-all treatment,” says Nicholas Caputo, a doctor at Lincoln Hospital in the Bronx, who was one early advocate of proning. Ventilation is one example of a treatment that can help or hurt depending on the patient. Another is dexamethasone, a steroid that suppresses the immune system. The drug has been shown to reduce mortality in patients with severe COVID-19, whose immune systems have become hyperactive, but might harm patients with milder cases whose immune systems are still trying to clear the virus. [Read: Immunology is where intuition goes to die] Doctors have also learned to watch out for COVID-19’s more unusual symptoms. The disease has been linked to kidney failure; those patients might need dialysis. It’s also linked to blood clots; patients who show warning signs might need blood thinners. Seeing more cases of COVID-19 has also allowed doctors to refine details like the size of tubing used with ECMO, an artificial-lung technology for the sickest patients who aren’t doing well on ventilators. A lot of this experience has been shared in real time and informally. J. Eduardo Rame, a cardiologist at Thomas Jefferson University Hospitals, helps convene a regular Zoom forum where doctors discuss the latest, such as how to use ECMO. “Experiential learning,” as Rame puts it, has been vital for sharing information about a new disease. But doctors are also trained to rely on data and randomized, controlled trials, not anecdotes. “We’re nowhere near the inflection point where we can have medical care dictated by evidence,” Rame says, which puts doctors in a strange position. For now, they have experience to go on, which is better than nothing. But it’s not data. Randomized, controlled trials can be difficult to run in the middle of a pandemic. Hospitals under stress might not have the time and resources. Doctors may be loath to deprive patients of an experimental drug that just might help, as is necessary for placebo-controlled trials. These trials, though, are valuable for identifying not just what works but what common experimental treatments don’t work and might even cause harm. The list of drugs that have failed in rigorous trials includes hydroxychloroquine, tocilizumab, sarilumab, interferon, and antivirals already used to treat HIV. Nearly all of the trials in this first group have involved repurposing drugs used to treat other conditions. [Read: The president’s silver bullet] Another set of clinical trials involve monoclonal antibodies, which mimic the proteins the human body naturally makes against pathogens. Monoclonal antibodies are the best near-term shot for a targeted therapy against COVID-19. President Trump gave them a huge boost of visibility after receiving Regeneron’s antibody infusion, which very early data now suggest could reduce doctor visits for COVID-19. The trials still need to run to completion though, and availability will be limited, because antibodies are particularly difficult to manufacture. Regeneron said in early October it has doses for 50,000 patients, which is fewer than the number of people getting COVID-19 each day in the U.S. right now. Antibody therapy will get better in the future too, as researchers try to engineer cheaper and more potent versions. All of this means that COVID-19 treatments are likely to become both more effective and more accessible in the future. And eventually there will be a vaccine. At some point, COVID-19 will become a manageable disease, akin to the flu. There will never be a good time to get the coronavirus, but getting it later will almost certainly be better than getting it today, tomorrow, next week, or even next month. from https://ift.tt/2JoAtkF Check out http://natthash.tumblr.com 
Kurtis, a young accountant in McKinney, Texas, likes the thing that many people hate about Donald Trump: that the president has left the pandemic response almost entirely up to local officials. “He left it up to each state to make their own decision on how they wanted to proceed,” Kurtis told me recently. Most experts think the absence of a national strategy for tackling the coronavirus has been a disaster. But Kurtis argues that North Dakota, for example, shouldn’t have to follow the same rules as New York City. Kurtis voted for Trump in 2016, and he plans to do so again this year. Some 82 percent of Republicans approve of Trump’s coronavirus response—a higher percentage than before the president was diagnosed with the virus. This is despite the fact that more than 220,000 Americans have died, and virtually every public-health expert, including those who have worked for Republican administrations, says the president has performed abysmally. Experts offer a few different explanations for the spell that Trump has cast over his supporters. The simplest is that Trump voters like Trump, and as is often the case with people we like, he can do no wrong in their eyes. “We might just as easily ask why Trump opponents think he is doing a horrible job with the pandemic,” says Richard Harris, a political scientist at Rutgers University. In academic terms, this is called “my-side bias”—objective reality looks different through the lens of your home team. (Sometimes literally: A famous 1954 psychology study found that undergraduates at Dartmouth and Princeton Universities had completely different perceptions of a football game played between the rival schools.) In fact, this tendency to approve of one’s own side might become self-reinforcing. If someone doesn’t support Trump and all that he does, they might stop considering themselves a Republican, and thus stop showing up as one in surveys, says Robb Willer, a sociologist at Stanford University. Other wrinkles of our current political moment could further explain why so many Trump supporters approve of the president’s pandemic response. Katherine Cramer, a political scientist at the University of Wisconsin at Madison, says the most consistent theme on the right-wing talk-radio shows she’s been listening to is a desire to trust people to make their own decisions, rather than trusting the government to make decisions for people. Shana Kushner Gadarian, a political scientist at Syracuse University, pointed out that understanding the failures of Trump’s pandemic response might require intimate knowledge of other countries’ public-health systems—a tall order for the average person. But another prominent scholar of the American right believes Trump support among men, in particular, is rooted in something more psychological. Many white men feel that their gender and race has been vilified, says the sociologist Arlie Russell Hochschild. Their economic prospects are bad, and American culture tells them that their gender is too. So they’ve turned to Trump as a type of folk hero, one who can restore their sense of former glory. Exposing themselves and others to the coronavirus is part of that heroism. Or as Kurtis told me when I asked him how he felt about Trump getting the coronavirus, “Trump’s willing to accept that risk to win for the American people. And Joe Biden is sitting in his basement.” 
T his hero theory of Trump is a continuation of Hochschild’s earlier work. A professor at UC Berkeley, Hochschild soared to the best-seller lists with her 2016 book Strangers in Their Own Land, which came out before the election but proved timely in its focus on the minds of Trump voters. For the book, Hochschild interviews an array of characters across Louisiana in an attempt to unearth what she calls their “deep story”: the emotional, feels-as-if truth of their lives. Hochschild describes her subjects’ deep story in a metaphor of a long line of Americans standing on a hill, waiting to get over the top, to the American dream. But as they stand there, tired and eager, they see that certain people are cutting the line in front of them. Women, African Americans, and immigrants are getting ahead, boosted by the government and its affirmative-action programs. As Hochschild writes, they feel “your money is running through a liberal sympathy sieve you don’t control or agree with.” Many white men, in particular, feel “shoved back in line,” she writes. Unable to draw confidence from their wealth, which is in many cases nonexistent, or their jobs, which are steadily being moved offshore, they turn to their pride in being American. “Anyone who criticizes America—well, they’re criticizing you,” she writes. Trump, meanwhile, has allowed his male supporters “to feel like a good moral American and to feel superior to those they considered ‘other’ or beneath them,” she writes. Trump might not always represent his supporters’ economic self-interest, but he feeds their emotional self-interest. Trump is, in essence, “the identity politics candidate for white men.” For a new book, Hochschild is talking with people in eastern Kentucky, another heavily conservative area. One trend she’s noticed is local white men’s lost sense of pride, and how they turn to Trump to restore it. To them, Trump seems to say, “I’m taking the government back and having it serve you,” she told me. “I’m your rescuer.” In Strangers, some of the Louisianans Hochschild interviewed were upset that women were competing for men’s jobs and that the federal government “wasn’t on the side of men being manly.” Some of her male Kentucky interviewees, many of whom have a family history in coal, feel even more strongly that men’s rightful place in the world is slipping away. Men in this community, she told me, “are starved for a sense of heroism. They don’t feel good about themselves. They feel like they haven’t done as well as their fathers, that they’re on a downward slope.” Coal jobs have evaporated, and liberals, they feel, are making enemies of white men. “Their source of heroism, of status, is humming; it’s fragile,” Hochschild says. This analysis comports with some polls of Trump voters. An Atlantic/PRRI poll conducted in 2016 found that Trump supporters were more likely than Hillary Clinton supporters to feel that society “punishes men just for acting like men.” As far as their leader’s pandemic response, Hochschild’s Kentuckians feel that Trump is doing the best he can, and as good of a job as possible under the circumstances. Though her subjects are worried about catching COVID-19, many see it as one of the unfortunate but acceptable risks of life. Confronting the coronavirus is a way to show stoicism and to feel heroic again. “I’ve heard it said that ‘This is hitting older people, and I’m an older person, but it’s really important to get back to work, and I’ll take the hit,’” Hochschild said. Her subjects think they can handle the virus just like Trump handles everything. “He’s a two-hamburger-a-meal guy,” she said. “He’s kind of a bad boy, and they relate to that.” This part of Trump resonated with Kurtis, who told me he likes that the president “comes off as a man. He doesn’t come off as weak.” Trump’s strength is a benefit in the foreign-policy arena, Kurtis feels. Joe Biden doesn’t give these men the same sense of restored pride. They feel the Democratic nominee is a Trojan horse liberal women and minorities are using to advance their own interests. Biden doesn’t present himself as a defender of white men, and they don’t see him that way. Hochschild sees her new work as an extension of the deep story she began probing in Strangers. In that book, her interview subjects found their guy in Trump. Now her interviewees are coming to realize their hero is surrounded by enemies. He’s battling evil forces such as the liberal media, the impeachment, the Democrats in Congress, and the lawyers who indicted his advisers. But Trump is fighting all of those enemies—the left, the deep state, the pandemic—and he’s fighting them for his constituents. The final chapter of this story, she said, is Trump becoming an almost Christlike figure to these men. “‘Look how I suffer,’” is how Trump presents himself, Hochschild told me. “‘I am suffering for you.’ And they say, ‘Thank you.’” 
I first met Kurtis in 2018, when I traveled to McKinney, my hometown, for research for my book about outsiders. I wanted to try to figure out why Californians were moving to the Dallas suburb. Before they relocated, Kurtis and Crystal had been living in Long Beach, paying $1,500 a month for an apartment the size of a bouncy castle. Kurtis found himself constantly at odds with his fellow Californians, who would yell at him for saying that he didn’t believe in global warming or that he was voting for Trump. “It’s like I couldn’t walk around with my ideas,” Kurtis told me for the book. Now that he’s in McKinney, Kurtis feels much more at home. Kurtis and Crystal bought a $325,000 house with a wraparound deck. They don’t get sneered at for their views, and they don’t have to recycle anymore. Their extended families have since moved out from California to join them there. And Kurtis wishes people would see the side of Trump that appeals to him: No apologies, what you see is what you get. Trump speaks the way people do at a barbecue, not at a dissertation defense. Sure, Kurtis reasons, the pandemic has killed a lot of people, but what was Trump supposed to do? Besides, the left called him a xenophobe for shutting down travel from China and for dubbing it the “China virus.” Kurtis’s father recently caught COVID-19 at church, which Kurtis saw as just another example of people knowing the risks but doing what they feel they need to do anyway. I asked Kurtis what he thought about Hochschild’s idea, that Trump supporters feel like white men are unfairly vilified these days. Kurtis deflected a little. “I don’t think it has to do with being white,” he said. He has other reasons, such as taxes and a possible repeal of the Affordable Care Act, for supporting Trump. At the same time, he was tired of “white men [being] looked at as the cause of everybody’s problems. I’m not gonna apologize that I’m white. I shouldn’t have to go around feeling like I have this great debt of reparations.” It’s been good to have a leader like Trump, he added, who takes no B.S. and is there to kick ass. “I’m proud to be an American again,” Kurtis said. Not all experts agree with Hochschild’s theory. Scott Winship, a sociologist and Director of Poverty Studies at the right-leaning American Enterprise Institute, says “it’s very questionable to explain overwhelming support among Republicans for Trump’s coronavirus response by pointing to whatever Hochschild’s white Kentuckians told her.” The income element, in particular, doesn’t hold up, he says: “Trump’s coalition in 2016 had higher incomes, on average, than the typical American.” But other experts’ research generally supports Hochschild’s thesis. “People look down on us, and now is our time to win,” says Jonathan Metzl, a professor of sociology and medicine at Vanderbilt University, summarizing what he has found is the attitude of some Trump voters. Given that the pandemic has disproportionately killed people of color, some white Trump supporters may write it off as a “them problem, not an us problem,” he says. Trump’s supposed heroism and sacrifice aren’t typically the reason his supporters offer when asked about his pandemic performance. Other explanations—the freedom to not wear a mask, the corporate tax rate, disdain for the leftward shift in the Democratic party—are more easily quotable. But the central wound remains: “Ban men” is a socially acceptable thing to say. And men who attend Trump’s rallies sometimes tell journalists that they’re willing to risk their lives to show up for Trump. “If I die, I die. We got to get this country moving,” these men tell reporters. Or: “If I catch COVID, that’s the consequences of my actions, so I’m willing to take that risk and have a good time today.” They’re bravely confronting COVID-19, just like the president. from https://ift.tt/3e7FDgb Check out http://natthash.tumblr.com Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. The president’s response to the pandemic should not have been a surprise. In December 2016, a month before Donald Trump was inaugurated, I asked how a pandemic would play out during his term. The question was not idly put: Every recent president before Trump had been challenged by epidemics, and Trump’s actions as both a citizen during the 2014 Ebola outbreak and a candidate on the campaign trail had been troubling. His record suggested that come a pandemic, he would lie, spread misinformation, opt for travel bans in lieu of more effective measures, and heed his own counsel over that of experts. Experience usually molds understanding, but Trump is still downplaying the pandemic, urging Americans not to “let it dominate your life” even after 210,000 had already lost theirs. One week ago, when asked if “there was anything that you think you could have done differently,” he said, “Not much.” As November nears, the coronavirus is surging again, with cases rising to record-breaking heights for the third time. To control the pandemic, changes are necessary, but Trump has proved that he does not learn from his mistakes—perhaps the most costly of his failings. If he is reelected, he will continue on the same path, and so will the coronavirus. More Americans will be sickened, disabled, and killed. Donald Trump is unchanging; the election offers an opportunity for the country to change instead. Read: The case against Donald Trump The near-term future is already set. Trump has repeated the lie that numbers are spiking because the U.S. tests extensively; in fact, the climbing cases have far outpaced the rise in testing, and are due instead to the rapidly spreading virus. Thanksgiving and Christmas are approaching. Several generations of family members will gather in indoor spaces for prolonged periods of close proximity and spirited conversation—the very conditions in which the coronavirus most readily spreads. Hospitalizations are rising in most states. Encouragingly, doctors and nurses have learned how to better care for COVID-19 patients, and the odds of dying from the disease, though still higher than for the flu, have fallen since the pandemic began. But health-care workers, physically exhausted and emotionally battered from a year of relentless work, are once again facing flooded emergency rooms and insufficient amounts of protective gear. The workforce of health-care providers is missing more than 1,000 colleagues who have died of COVID-19. And while the two previous surges were concentrated in specific parts of the U.S., allowing health-care workers from more tranquil regions to help colleagues in the hardest-hit ones, the current surge has lit up most of the country. Reinforcements will be scarce. Death rates always lag behind cases and hospitalizations. During the national death rate’s recent plateau, about 700 people were still dying every day, and that rate has risen by 15 percent in the past two weeks. It will climb further. This is not, as Trump baselessly suggested, because doctors and hospitals are overcounting COVID-19 deaths to “get more money”; in fact, deaths are undercounted. COVID-19 has already become the second leading cause of death in the U.S. this year after heart disease (or the third, if you lump all cancers together). It is likely the new leading cause of death among people ages 25 to 44. Every lost person leaves behind an average of nine grieving loved ones. Many thousands of survivors are struggling with long-term symptoms. [Read: Long-haulers are redefining COVID-19] As I wrote last month, there is a real risk that Americans will become habituated to this horror, and that COVID-19 will become another unacceptable thing that the U.S. learns to accept. That is all but inevitable if Trump wins a second term. His administration has given no indication that it will dramatically change its strategy. If anything, it has doubled down. It is allowing the virus to freely spread among younger people in the hopes of reaching herd immunity—an unfeasible strategy that has been widely panned by the scientific community. Such a strategy could leave millions dead, and many others with chronic illness. Vaccines will arrive, but not quickly enough to put a dent in the ongoing surge. Treatments are being developed, but so far, months of trials have provided strong, consistent evidence only for dexamethasone, which reduces mortality rates among the most severely ill patients from 26 percent to 23 percent. And yet, the pandemic is not impossible to control, contrary to what White House Chief of Staff Mark Meadows recently suggested. Many other nations have successfully controlled it, some more than once. Masks can stop people from transmitting the virus. Shutting down nonessential indoor venues and improving ventilation can limit the number of superspreading events. Rapid tests and contact tracing can identify clusters of infection, which can be contained if people have the space and financial security to isolate themselves. Social interventions such as paid sick leave can give vulnerable people the option of protecting their lives without risking their livelihoods. [Read: America is trapped in a pandemic spiral] The playbook is clear, but it demands something that has thus far been missing—federal coordination. Only the federal government can fund and orchestrate public-health measures at a scale necessary to corral the coronavirus. But Trump has abdicated responsibility, leaving states to fend for themselves. In May, I asked several health experts whether governors and mayors could hold the line on their own. Most were doubtful, and the ensuing months have substantiated their fears. There are three small mercies that Americans can be thankful for. First, COVID-19 is a starter pandemic, and SARS-CoV-2 is neither as contagious nor as lethal as other pathogens. Second, it is the only major epidemic that Trump has faced during his presidency. (By contrast, Barack Obama dealt with the H1N1 flu and MERS in his first term, and Ebola and Zika in his second.) Third, it occurred not during the dawn of his term but at its twilight, when Americans have an opportunity to avert further incompetence. Whatever the outcome of the election, the coming winter will be difficult. And whoever occupies the White House on January 21 will probably have to deal with another major epidemic before his term is over. With luck, that event won’t begin until the COVID-19 threat has subsided, but overlapping outbreaks are also possible. We do not know how Joe Biden would fare, and if he is elected, the U.S. will still be riddled with systemic weaknesses and inequities that another pathogen could also exploit. But we do know exactly how Trump will react to the next crisis. The U.S. is trapped in a pandemic spiral, and so is Donald Trump. Science values replication—repeated experiments that verify whether the same outcome occurs. But in this case, that work is unnecessary. The U.S. has now clearly seen what happens when a pandemic occurs under Trump. It is an experiment that no one should ever want to rerun. from https://ift.tt/35KvcuW Check out http://natthash.tumblr.com Many provisions of the CARES Act ran out in July. Soon, state unemployment insurance will start to run out for people who lost work at the beginning of the pandemic. Congress and the White House have failed to pass new support, and even if an agreement is reached, Senate Republicans have signaled that they’ll prioritize confirming Amy Coney Barrett to the Supreme Court before the election. On this episode of the podcast Social Distance, the executive producer Katherine Wells and the staff writer James Hamblin talk with Diane Whitmore Schanzenbach, an economist at Northwestern University who studies the social safety net. She describes a dire situation for poor Americans and a tremendous need for new relief funding. Listen here: Subscribe to Social Distance on Apple Podcasts, Spotify, or another podcast platform to receive new episodes as soon as they’re published. What follows is a selection of the conversation, edited and condensed for clarity: Katherine Wells: One thing I’ve had a hard time grasping is the scale of the problem we’re facing right now. How do you describe it in a way that people can understand how big it is? Diane Whitmore Schanzenbach: A way to think about it is through the access to food that families have. And we’ve got two broad measures of that. One is food insecurity. That’s the idea that families don’t have enough money to buy the foods that they want to eat. Sometimes it means hunger, and sometimes it means shifting to cheaper foods. And the rate of food insecurity—especially among families with kids—has skyrocketed during COVID-19. The best estimates are that the numbers have tripled. It used to be around 10 percent. Now it’s around 30 percent. Three out of 10 people with kids are food insecure right now. And that’s a broad measure. We can think about people reporting they don’t have enough to eat. And similarly, we’ve seen levels of people in the United States not having enough to eat that are unconscionable. They’re higher than anything we’ve seen on record. I just pulled the most recent numbers, and 14 percent of people report to the Census Bureau that, over the first half of October, they sometimes or often don’t have enough to eat in their house. That’s a lot of kids. Wells: As I’m listening to you, rage is welling up inside of me. Why is this happening? Schanzenbach: When it comes to kids, two big things have shifted. One is schools, and the other is family money that allows them to buy food. The question of schools is hard, right? We need to get the virus under control, and there’s all sorts of moving parts. That’s a hard problem to solve. What is not a hard problem to solve is feeding people. We can give them money. We can give them food stamps, what is now called the SNAP program. There’s a lot of very straightforward policy solutions that could be implemented. And I should be quick to say that we’ve done some of those. [The CARES Act created] the Pandemic EBT program, which provides families money for school meals that they missed. We’ve been able to study it and we can show that it reduces food hardship as experienced by kids. That’s a really good program. We were worried that Congress wasn’t going to reauthorize it, but in the nick of time, they decided that they would reauthorize it through this year. What’s staggering is these numbers would be even worse if it weren’t for what we’re already doing. Just fundamentally, this is not hard to solve. It just takes money. Wells: How much did the CARES Act help? Schanzenbach: That’s a hard question to answer because so much other stuff was going on with the economy. It’s hard to know how much worse things would be if it weren’t for the CARES Act, but we can say they made some really smart policy decisions. That initial boost to unemployment insurance, that extra $600 a week, really made a big difference. Another policy change that they made was they increased SNAP benefits to people who weren’t already getting the maximum benefit. And it also gave states—this is not very exciting, but, boy, it makes a difference on the ground—they gave states flexibility to concentrate only on enrolling new families who were newly eligible for SNAP and not processing renewals and things like that. I wrote a paper for the Brookings Institution that tried to understand, given how much we’ve spent, why is there still so much suffering? We came up with three reasons. The first is that aside from that unemployment-insurance bump, the rest of the benefits just weren’t all that generous. The second was, many of the benefits came with delays. At the beginning, people had to really wait to get their unemployment insurance. And the third is that there are a lot of holes in our safety net. A lot of families suffering food insecurity and hunger didn’t lose their jobs, but they lost income anyway. They lost shifts or they lost gigs. But because they didn’t lose their job, in most places, they’re not getting unemployment insurance. They’re just having to weather the shock without any additional public benefits. Wells: What’s the situation we’re in right now, given that many of the provisions of the CARES Act have expired, and the federal unemployment is out? What do we need now and what’s happening? Schanzenbach: We need something from Congress. And, of course, it’s been very frustrating as someone who studies the amount of hardship that the poor face, to see so much inaction. But I think we need a couple of things. We need more unemployment insurance. I’m not sure it needs to still be at $600, but it has to be something. A lot of people think $400 is maybe the right amount. I think it’s a no-brainer that we should be increasing SNAP benefits. During the Great Recession, we increased them by 15 percent. That was a very effective policy, both in terms of stimulating the economy and in terms of reducing hardship. We’re seeing so much hardship and we’re spending precious little relief aimed at the poor, which doesn’t make a lot of sense. And, of course, as someone who studies kids, I would argue that states really do need additional resources so they don’t have to cut school spending. As you may know, many states are under balanced-budget requirements. So when you get hit with an economic shock like this, the budget gets balanced on the backs of kids and other vulnerable populations. from https://ift.tt/3mpnFIH Check out http://natthash.tumblr.com On a normal day, the White House is one of the safest buildings in the world. Secret Service snipers stand guard on the roof, their aim tested monthly to ensure their accuracy up to 1,000 feet. Their heavily armed colleagues patrol the ground below and staff security checkpoints. Belgian Malinois guard dogs lie in wait for anyone who manages to jump the property’s massive iron fence. But safety means something different in a pandemic. Over the past few days, several aides to Vice President Mike Pence, including his chief of staff, have tested positive for the coronavirus. The outbreak is the second in the White House in a month, after dozens of people, including President Donald Trump himself, tested positive following the apparent super-spreader event hosted by the administration to celebrate the Supreme Court nominee Amy Coney Barrett. The outbreaks have been both utterly predictable and totally shocking. The Trump administration has consistently downplayed the severity of the coronavirus, encouraged Americans to resist safety measures, and promised that the pandemic is nearing its end. But the people orchestrating the country’s disastrous coronavirus response had no plausible deniability: The very best experts, information, and precautions were all available to them, even if they refused to pass that help on to others. People will write books on everything Donald Trump did wrong during the pandemic, with explanations both personal and ideological for his administration’s often willful failures. But for a group of people for whom self-preservation has long been an obvious goal, their willingness to put themselves in optional danger, given all the resources at their disposal, can’t be completely explained by Trump’s lack of empathy or his advisers’ policy goals. It suggests that on top of everything else, the administration fell prey to an error of intuition: Presumably, Trump and his coterie felt safe, despite the mortal danger nipping at their heels for all to see. Trumpworld’s infection fiasco is an especially bizarre case study of one of the pandemic’s defining features: how different feeling safe and being safe actually are. This misperception has played out in millions of homes and workplaces across the country as regular people make good-faith efforts to grapple with the swiftly changing circumstances of American life, absent the resources available to the federal government. Things that used to be safe, such as visiting grandparents and attending a friend’s wedding, are now potentially deadly. Things that used to be foreboding, such as the sight of many masked strangers in public, are now a source of comfort. This new sort of safety is difficult to adapt to, both practically and emotionally. Over the summer, previously innocuous private social gatherings, such as dinner parties and birthday celebrations, were cited as a primary driver of new infections all over the United States. In some instances, the people involved perhaps didn’t care about the risk or thought the pandemic was fake. But in others, they likely couldn’t imagine why they should be scared of time with loved ones. Many of these same people were wearing masks to the grocery store, using hand sanitizer, and otherwise doing what they understood to be asked of them. Safety is among the most powerful motivators of human behavior, which also makes the drive to feel safe a potent accelerant for confusion, disinformation, and panic. Staying safe requires an accurate, mutually agreed-upon understanding of reality on which to assess threats and base decisions. Since the pandemic arrived in the U.S., however, politicians have sparred over basic safety precautions and aggressive reopenings. The federal government and many of its allies at the state and local levels have actively undermined efforts to get people on the same page. These contradictions have sown confusion, even among those who disagree politically with the leaders encouraging people to flout masking and social distancing. When everyone is left to write their own version of Choose Your Own Pandemic Adventure, no one is safe. 
To understand how humans think about safety, you have to understand how they think about fear. To be safe, people need to be free from the threat of physical or mental harm. But to feel safe, people need to be free from the perception of potential harm, confident that they understand what the likeliest threats are and that they are capable of avoiding them. Whether their perception is accurate is often incidental, at best, to the feeling itself. “Fear reactions are very primitive,” Arash Javanbakht, a psychiatry researcher at Wayne State University, told me. “We don’t react so well or so accurately to conceptual threats.” People learn what or whom to fear in a few different ways, according to Javanbakht. The things we have experienced or observed ourselves, such as car accidents or the kinds of violence frequently depicted on the news, have a significant impact. So do the warnings of peers and authority figures. This assemblage of influences—family members, friends, co-workers, religious or cultural leaders—is as much a tribe now as it was when these instincts evolved, and the security and support that it can provide creates a profound psychological incentive to remain a member in good standing of one’s group. People’s dependence on group affiliation for safety and support can be so strong, in fact, that it sometimes overrides more logical assessments of fear and safety, Javanbakht said. Even in situations where the actions of the tribe’s leaders contribute to the group’s collective misery, many members will find it difficult to reject that leadership. Instead, studies have shown, people dig in their heels when confronted with evidence that challenges their beliefs or identity: They redouble their support for trusted authority figures and reject outside criticism, which they’ll often paint as proof that the group is under threat. Javanbakht compared this dynamic to softer forms of American tribalism, such as being a fan of the Cleveland Browns. The team’s leadership has been antagonizing its fanbase for decades, but some people cannot be mistreated into retracting their emotional and monetary support. Many Americans have come to understand their political affiliations in much the same way they do their affinity for particular sports teams or movie franchises, but with much darker implications than, say, getting your hopes up about an Atlanta Braves postseason run. On a basic level, you could see tribalist fear in how people scrambled for clarity early in the pandemic. The methods humans use to understand and pursue safety aren’t really built for quick, competent responses to novel threats. Fear abounds as people realize they don’t have a script to follow. (Buy six cases of bottled water.) Panic sets in. (Lysol the groceries.) They wait for guidance from existing leaders and search for previously overlooked ones. (Nice to meet you, Dr. Fauci.) They monitor the behavior of their peers. (Wear a mask.) In a country with a dwindling consensus on the basic experience of reality, though, tribal affiliation can be especially fraught. Trump and other leaders have conscripted supporters into cultural warfare, recasting safety measures as political attacks from the opposition and tools of social control. Some people have duly followed, rejecting simple precautions recommended by scientific experts, such as masks and open windows, and promoting some of the more extreme reactions to the pandemic: The virus is a hoax; it’s a bioweapon meant to hurt Trump’s reelection chances; it really is just the flu. Tribal affiliations have been exploited in American politics for centuries; influential people stoke fear against those outside their constituencies, such as ethnic and religious minorities, immigrants, and the poor, which intensifies supporters’ belief that loyalty to the group itself is their best bet for safety. But Trump, from whom this narrative radiates, has been especially adept at fomenting and wielding fear as a source of power in his brief political career. People who have built a significant portion of their identity around Trump fandom by attending rallies, joining Facebook groups, and buying merchandise likely have a psychological investment in his version of reality that’s too high to consider abandoning; for some of them, losing those beliefs might feel like a fate worse than the coronavirus. When the spell is that strong, according to Javanbakht, it generally requires a more immediate measure of danger to break it, such as the COVID-19 death of a loved one. Intuitive failures of safety extend beyond Trump and his acolytes. Ultra-strict adherence to pandemic precautions can itself be a display of tribal identity, especially as scientific understanding of the virus evolves and some safety measures, such as wiping down groceries with sanitizing wipes, can be dispensed with. No matter where their beliefs fall on the country’s political spectrum, people whose identity is more weakly tied to a political group have an advantage when it comes to adapting in response to new information. A relatively small proportion of conservatives are virulently anti-mask, and most liberals are not fully sequestered in their homes, Lysol-soaking their mail-in ballots. While these sets of behaviors share an underlying psychological mechanism, they are not equivalent. To belong to one tribe, people accept an outsize and sometimes irrational portion of responsibility for their own safety and that of others through self-abnegation and personal fastidiousness. To belong to the second tribe, people must refuse to care about others at all. 
Over time, theoretically, the country’s collective understanding of safety should both improve and normalize, as the definition of safety is expanded to account for the pandemic, and the group—in this case, Americans as a whole—forms new norms to achieve it. In most of America, that hasn’t necessarily been the case so far, and any progress has been hard-won over sometimes-violent opposition. But the tribalist fear that causes those big variations often doesn’t account for smaller ones among families and social circles, which tend to be politically similar. Anyone who’s been holed up in their home for months, watching friends and family proceed with indoor weddings or spend their weekends inside bars—or anyone who’s invited a buddy to a day at the beach only to be rejected over amorphous safety concerns—knows that something more complicated is going on. Even among people with similar beliefs, a smooth, uniform pivot to a new understanding of safety requires diligent, competent, well-intentioned leadership. According to Eric Scott Geller, a psychologist at Virginia Tech who has studied safety for more than 40 years, the best way to get lots of people to adopt new safety precautions is to be explicit and consistent about what they are and why they’re important, and then demonstrate examples of people adhering to them repeatedly over time. As a whole, American leadership continues to do the opposite. “I’ve been in the business for a long time, and I’ve never seen anything quite like this,” Geller told me. “The biggest problem we have right now is mixed messages.” Left to their own devices, people chart their paths based on their personality, how they see the world, and how they relate to risk. According to Geller, many people presented with a barrage of contradictory instructions just grow tired and give up. Others become hypervigilant, their behavior calcifying against new information that might let them ease up and enjoy life a little more. Still others simply choose optimism, no matter how dangerously misguided—such as the belief that “herd immunity” is near, or the assumption that catching the virus will have no long-term consequences for them. “People will gravitate to the positive message because it’s convenient, and it’s not scary, it’s not fearful,” Geller said. And so the chaos of a country becomes the chaos within its families and communities. People spar over their assumptions and hastily made decisions based on half-understandings of scientific evidence. They’re forced to conduct their own awkward, fraught behavioral micro-negotiations before visiting relatives, celebrating a birthday, or going out for a beer on a bar’s patio. Americans have no common conception of the pandemic, which means you can’t assume that someone you’ve trusted for years isn’t about to expose you to a deadly disease, or even that you live on the same plane of reality. People feel bad about enforcing their boundaries, or they simply grow tired of constant vigilance. Occasionally, they just forget. In some ways, these tragic errors in intuition are convenient for leaders, both within and outside the government. Birthday parties and vacations and nights out on the town are easily framed as personal choices free from government influence, even though other countries have gone much further in giving their citizens tools to keep themselves safe and make good decisions—nationally coordinated testing programs, extensive government aid for businesses, a clear and consistent message about safety. You can see the same finger-pointing dynamic in how some college presidents set their charges up to fail, and then punished them for becoming infected. This approach reflects how, in America, blame for large-scale destruction and death is often shunted onto those with the least power to change policy or protect themselves. “Think about all the accidents on oil platforms, or drilling rigs,” Susan Silbey, a sociologist who studies safety at MIT, told me. “It's the same few companies over and over again. They always blame the workers.” 
Even with mixed messages from above, pandemic-era safety would be a little bit clearer to negotiate if talking about your behavior and asking questions about others’ wasn’t so excruciatingly awkward. Ensuring pandemic safety requires interrogating loved ones about whom they’ve been with and what they’ve been doing, and if they’ve been tested recently. If that sounds familiar, it’s because health educators ask people to go over the same topics anytime they have a new sexual partner. As it turns out, it wasn’t just the sex that made those conversations notoriously difficult to have, but the same strategies that public-health experts have developed to talk about sex might be just as useful in these new types of negotiations. As masks became both more common and more controversial in the United States during the spring, Logan Levkoff, a sex-and-relationship educator, found herself having the same conversation over and over again with her peers. The dynamics of pandemic health and sexual health make people anxious and cagey in very similar ways, about very similar types of precautions. Should you refuse to attend your cousin’s wedding unless she moves it outside? Should you tell your maskless friend to mask up? These situations are “still fraught with shame and stigma and assumptions about people’s politics,” Levkoff told me. “Often, if we don’t want to have someone make assumptions about us, and we don’t want them to feel we’re making assumptions about them, we just don’t say anything at all.” That avoidance can put people in riskier situations than they’d choose for themselves if they felt free to be picky. Even so, the desire not to anger loved ones in an already anxious and fearful time can be strong. “That’s where we get tripped up a bit,” Levkoff said. “We think that in those intimate relationships, it would be a violation of trust to ask.” She said that the politicization of public-health measures has likely exacerbated this dynamic. Conversations about safety can quickly devolve into arguments about political differences; less than two weeks out from the election, many people are probably happy to avoid poking that bear if they can avoid it. These conversations can even be hard among political peers, which in theory seems silly. We’re in a pandemic, after all. Isn’t transparency just reasonable? “We have this belief that our health is a measure of our character,” Levkoff explained. In America, being disease- and disability-free is often assumed to be an indicator of a person’s moral righteousness and good priorities. To you, asking a friend if she’s been to a house party recently might feel like checking a box on a to-do list. For her, it might feel like being told she’s some kind of degenerate. These dynamics rear their ugly head in less intimate interactions, too. After the University of Notre Dame’s president, John I. Jenkins, became one of the many people who tested positive for the coronavirus after attending the apparent White House super-spreader event celebrating Barrett, an unnamed member of the Notre Dame delegation told The New York Times that the group’s decision to go maskless was politeness, not politics—an attempt to blend in and adhere to the conventions set by the event’s powerful hosts. There are many ways in which people are expected not to rock the boat in American social culture. Those niceties can set people up to spread a deadly disease in an environment where the circumstances of safety have changed swiftly and confusingly. Looking for ways to have these conversations—or even just thinking about their implications at all—is half the battle. Broaching an uncomfortable issue or figuring out a new way to understand our friends and loved ones is awkward, but it’s certainly doable. Tread lightly. Reassure friends and family that you’re just trying to help everyone have fun. Volunteer information about your own behavior. Starting these conversations is often the hardest part, especially among people whose goals are the same, even if their methods differ. They’ve already made the most difficult concession: banishing the idea that the way we understood one another seven months ago is enough to get us through the months ahead. “We think we share the same values and norms,” Sibley, the sociologist, told me. “We think we know each other.” from https://ift.tt/3dW4BPt Check out http://natthash.tumblr.com Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. The United States is sleepwalking into what could become the largest coronavirus outbreak of the pandemic so far. In the past week alone, as voters prepare to go to the ballot box, about one in every 1,000 Americans has tested positive for the virus, and about two in every 100,000 Americans have died of it. This third surge is far more geographically dispersed than what the country saw in the spring or summer: The coronavirus is at risk of careening out of control, and it can be found in every kind of American community, from tiny farm towns to affluent suburbs to bustling border cities. This is the first of the American surges with no clear epicenter: From North Carolina to North Dakota, and Colorado to Connecticut, more Americans are contracting COVID-19. The United States now reports nearly 60,000 new cases every day, numbers previously seen only during the peak in July and early August, according to the COVID Tracking Project at The Atlantic. Since the middle of September, the number of new cases diagnosed each day has swelled by 73 percent. The number of Americans hospitalized has increased by at least 40 percent. 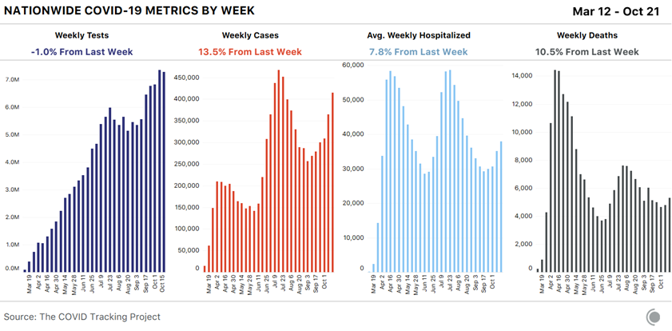
True to its pandemic response so far, the White House has not mounted an effort to stop this spike. Donald Trump has not spoken to the nation or pushed forward a strategy to address a third surge. And both the president and Vice President Mike Pence are holding crowded in-person rallies in some of the same states—such as Iowa, Pennsylvania, and Indiana—now seeing surges. In the next two weeks, yet more Americans will fall ill, in numbers that are certain to make this an Election Day unlike any other. If the country’s medical and political crises were ever separate, they are not now. The third surge has belied some of Trump’s predictions about the pandemic. The president has repeatedly said that only states led by Democrats have struggled with the virus. “If you take the blue states out, we’re at a level that I don’t think anybody in the world would be at,” he said at a press conference last month. Since then, coronavirus infections have skyrocketed in rural America. The number of people hospitalized with COVID-19 has more than tripled in North Dakota, Montana, and Wisconsin. It has roughly doubled in South Dakota, Utah, Indiana, and Ohio. [Read: The vaccine news that really matters] But describing what’s happening now as simply a red-state surge would be too pat. Cases are now rising in all but nine states—meaning this surge is more widespread, and harder to explain, than either of the earlier waves. It may end up being less deadly, however: The United States now runs many more tests than it could in March and April, and people who are hospitalized with the virus are less likely to die. At the same time, the virus’s long-term complications, which might range from respiratory disability to cognitive decline, now seem more ominous. What’s happening now might be best understood as three smaller types of outbreaks. You could call them the rural explosion, the swing-state surge, and the fatigue creep. The rural explosion The first phenomenon: After months when viral transmission seemed to dominate cities, the coronavirus has now wheedled its way into rural America. That’s a large part of what’s happening in North and South Dakota, which stand out even in a country of hot spots. Earlier in this article, I mentioned that one in 1,000 Americans has tested positive for COVID-19 in the past week. But on Tuesday alone, one in every 1,000 residents of North and South Dakota was diagnosed with COVID-19. That’s a per-capita rate of infection nearly double New York State’s during the spring. In North Dakota, the harder hit of the two, the number of people hospitalized with COVID-19 has tripled in the past month. The state is so deluged that it has asked residents to do their own contact tracing. 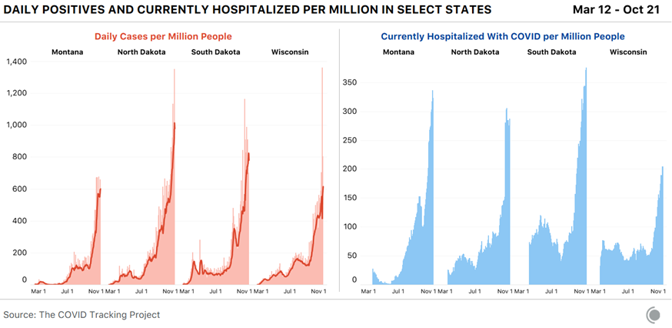
The state’s cases are not limited to its largest cities, such as Fargo and Bismarck. Look at Ward County, for instance, which is home to about 68,000 people and, according to the state health department, reports nearly 646 active cases—one case for every 105 residents. Or Williams County, with a population of about 38,000, which reports 203 active cases—one case for every 187 residents. The state of Maine has 43 times more residents than tiny Stark County, North Dakota, but they reported the same number of new COVID-19 cases on Tuesday. To some degree, the rural explosion is playing out across the conservative Mountain West. The western U.S. now reports as many cases per capita as it did in late June—but spread over the country in a very different way. In the early summer, California and the Pacific Northwest dominated the region’s numbers; today, the interior states lead. Wyoming, Idaho, and Montana, where Democratic Governor Steve Bullock has fought incumbent Senator Steve Daines in a close congressional race, now each report at least 400 cases each day per 1 million residents. Utah is reporting more than 1,200 new cases a day, its worst-ever outbreak, but most cases remain concentrated in Salt Lake City and the surrounding area, according to state data. The swing-state surge Cases and hospitalizations are also rising across some of the Great Lakes and upper-Midwest states that could prove most crucial in the presidential election. The Midwest now has more COVID-19 cases per capita than any other region in the country, and is reaching rates of infection that come close to matching the worst of the Northeast’s during the spring and the worst of the South’s during the summer.
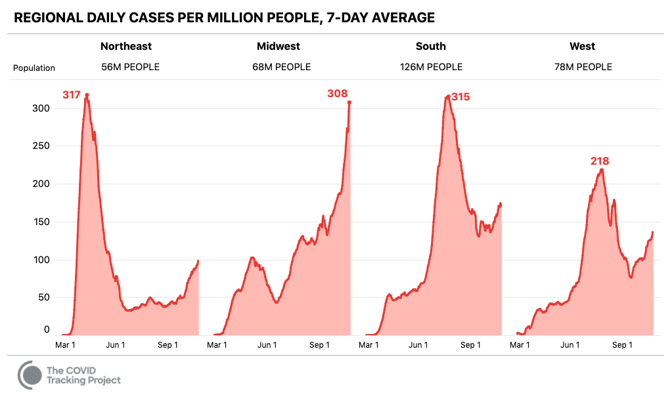
I wrote last month that Wisconsin looked like a growing hot spot. That warning has come true: New cases in Wisconsin have more than quintupled since dipping in late August, and hospitalizations have reached an all-time high. More than 3,500 Wisconsinites now test positive for the virus every day. The state’s pandemic response has been politically polarized: While its Democratic governor, Tony Evers, has defended a mask mandate against criticism from Republican leaders and conservative legal groups, mask wearing has been spotty in some areas and many people have refused to reduce their travel to stop the spread of the disease, according to Wisconsin Public Radio. In Ohio, cases and hospitalizations have more than doubled in the past month and now exceed the previous all-time peak. More than 2,000 Ohioans, on average, are now diagnosed with the virus each day. In Iowa, the home of a close congressional race that could determine whether Democrats retake the Senate, a large outbreak continues to grow. More than 950 Iowans, on average, are diagnosed with the virus each day; and more than 500 are currently in the hospital, an all-time high. [Read: Why Trump’s rapid-testing plan worries scientists] The most ominous state may be Pennsylvania, whose 20 electoral votes could determine the election’s winner. The Keystone State saw a huge coronavirus outbreak in the spring, but this appears not to have protected it from another surge: Its numbers have deteriorated in the past month. On Saturday, the state reported more than 1,800 new cases, its third-highest single-day total of the pandemic. While many fewer people are hospitalized now than were in the spring, the state’s outbreak is still growing: There are now at least 1,400 new cases a day, as many as in late April. Voting in Pennsylvania has already become contentious, and Republicans and Democrats have fought over rules for voters who want to avoid going to polling places. Earlier this week, the Supreme Court ruled that the state could count mail-in ballots received up to three days after Election Day, blocking a Republican challenge to the policy. While voting in person is relatively safe, registered Democrats have requested absentee ballots at two to three times the rate of Republicans, according to the Pennsylvania Department of State. If a surge in COVID-19 cases limits turnout on Election Day, it could depress the GOP vote more significantly. A pandemic-fatigue-induced creep of cases The fact that Pennsylvania’s cases are rising despite its earlier outbreak raises a third specter, which seems to be happening in New Jersey, where new cases have quadrupled since their low in mid-August. More than 1,000 residents of the Garden State now test positive for the virus every day, a return to late-May levels. Hospitalizations have remained at much lower levels, though about 300 more people are hospitalized than were last month. Deaths have not increased at all. In the Northeast, cases have also recently increased in Massachusetts and Connecticut. They have also modestly risen in New York—every day, about 400 more people now test positive for the virus than did in the middle of last month—but numbers still pale in comparison with springtime levels. [Read: This overlooked variable is the key to the pandemic] Many of these states, Pennsylvania among them, saw large spikes in the country’s first two waves. They successfully kept cases low throughout the summer. If they cannot now keep viral levels low as they enter the winter, it bodes ill for the hopes that any region can depress transmission indefinitely. (Surging caseloads in Europe offer the same warning.) Since March, the United States has failed to keep the virus from spreading widely. In the past few weeks, that failure has again become acute, and now the most important date on the American political calendar will be defined by sickness. Trump has chosen Americans’ fate during the coronavirus pandemic. Now the disease will define the day that the country chooses his.
from https://ift.tt/34lLOtN Check out http://natthash.tumblr.com
Dear Dr. Hamblin, I’m perfectly healthy. I’m 42 and I exercise routinely, eat a whole-food, plant-based diet, and have excellent biomarkers. If I get the flu, chances are it will be mild and run its course. So why risk any potential negative side effects of a vaccine? To protect me against something that I might still get even with the shot? Even though I’m sure the risk is low, why should I potentially jeopardize my health? I guess I see only downsides and no upside. Todd Kelly Philadelphia, Pa. Your concerns are widely shared, and your question is important. The answer is especially worth considering because the same logic that guides your decision will apply to the coronavirus vaccines in coming years. Let’s start with the downsides. Any moral decision starts with accurately assessing the risk of taking an action. In this case, it’s as close to zero as anything modern medicine has to offer. If I were going to focus on risks, I’d be more worried about you getting hit by a car on your way to the pharmacy or doctor’s office than anything that might happen because of the shot. Influenza vaccines come in a few types. For healthy American adults like you, the most commonly used variety is the shot. It contains an inactivated form of the virus—either segments of an actual influenza virus’s genetic material or synthetic mimics of those segments. In any case, it can’t cause the flu. Getting the flu from a segment of the virus’s genetic material is impossible. It’s like the difference between inhaling a bee’s wing and inhaling an actual bee. The only type of flu vaccine that contains a living virus is the nasal spray. But even that can’t cause the flu. The nasal vaccine contains a “live attenuated” virus, meaning it can’t invade human cells and replicate, so it’s like inhaling a bee without its stinger and genitals. Why inhale a whole bee at all, you ask? Well, compared with shots, these live-virus vaccines can more reliably induce a broader immune response. Generating a sufficient immune response is, of course, the goal. It’s also the source of any symptoms that might arise after the shot. Most people will have some mild soreness or redness at the injection site. A significant minority will have some fatigue or a headache. These symptoms are a result of your immune system reacting to the proteins that have just been injected into your muscle. Unpleasant as they may be, you could think of them as a sign of your immune system getting stronger, like being sore after one of your workouts. Even if you feel a little uncomfortable, none of these symptoms is comparable in scale or severity to having the flu itself. Like COVID-19, influenza is not a disease that completely spares healthy young adults. Some years it largely does, but other years see thousands of hospitalizations and even deaths. In 1918, to take the worst example, influenza killed millions of young, healthy people. Vaccination carries nothing close to that level of risk. The one scary-sounding, longer-term complication that has been associated with the flu shot, if not definitively linked to it, is something called Guillain-Barré syndrome, an autoimmune condition that results when the immune system misfires and attacks parts of the nervous system, causing muscle weakness. In some cases it leads to temporary paralysis of certain muscles. It can happen in the days and weeks after all sorts of viral or bacterial infections (including COVID-19)—any of a menagerie of things that trigger the immune system to go into attack mode. The Centers for Disease Control and Prevention and global-health agencies suggest that the odds of developing Guillain-Barré syndrome after receiving the flu shot are about one or two in a million. And if that sounds too risky to countenance, consider that you’re much more likely to get Guillain-Barré after an actual case of the flu than after getting a vaccine. [Read: Why the government pays billions to people who claim injury by vaccines] So, really, this is sort of like talking about how seat belts may cause redness or irritation on bare skin and, in rare cases, can cause internal bleeding and organ damage during a serious car accident. If you focus on those risks, wearing a seat belt sounds like a bad idea. Why take a chance? But the value of seat belts becomes obvious when you shift your focus to the danger of going without a device that saves tens of thousands of lives every year. Likewise, when weighing the risks of getting a flu shot, you have to consider the much more relevant risks of not getting vaccinated. We get used to health risks—such as deaths from car accidents, heart disease, gun violence, and influenza—as they lose their novelty and start to take them for granted, but that doesn’t make them any less dangerous. Somewhere between 10,000 and 60,000 Americans die of the flu each year. Combine that with the effects of so much illness and missed work, and the virus’s annual impact on the U.S. economy is about $90 billion. This brings us to the upside: If everyone got a flu shot, we could bring those numbers down to about zero. Vaccination is a measure that we undertake to remove ourselves from the pool of susceptible people who can become vectors of disease. You have a great opportunity to do an essentially risk-free thing to play your part in saving thousands of lives. And there’s really no opting out. Whatever you choose, it affects everyone. It’s a personal decision in the same way that driving on the sidewalk is a personal decision. [Read: America should prepare for a double pandemic] This is true of getting any vaccine, but especially flu shots, because of the nature of the virus. Influenza mutates so rapidly that each year’s vaccines are based on modeling predictions about which strains will spread most widely. Some years those models work pretty well, and other years they don’t. Even in a good modeling year, a flu shot offers only partial immunity: Some people who get the shot will still be susceptible to the flu. The imperfection means it’s especially important that everyone gets vaccinated to achieve some degree of herd immunity. When you have a more reliably effective vaccine, you can get to herd immunity with a smaller percentage of the population being vaccinated. But with the flu vaccine, we always need to aim for 100 percent participation. Each year, about half of Americans get vaccinated. A partially effective vaccine has one other important effect: It can make the disease milder even if it doesn’t prevent an infection. That means a lower likelihood of going to the hospital and fewer days of being sick. Even if that doesn’t matter to you personally—maybe you have unlimited sick days, or maybe you like being sick (I don’t know)—a shorter course of disease means you’re less likely to infect other people. That’s ultimately what vaccination is about. [Paging Dr. Hamblin: What if the vaccine works only half the time?] The flu is a global disease that kills more than 500,000 people every year. Someday it will again become a pandemic that kills millions. The rates of death are much higher in countries with less developed health-care systems. The currently available influenza vaccines are difficult to use in low- and middle-income countries without the systems required to vaccinate everyone every year. You and I are lucky to live in a wealthy country and have easy access to a free vaccine. For people like us to forego it is morally unconscionable. from https://ift.tt/3jifNXF Check out http://natthash.tumblr.com 
When I finally met Sanjiv “Sam” Gambhir in person—last November, after months of planning—I knew he was dying. Gambhir knew it, too. Seated in his small, bland office at the end of a warren of hospital hallways in Palo Alto, he was visibly depleted from the cocktail of treatments, some highly experimental, that were being deployed to save him from cancer. But Gambhir, a titan in the field of diagnostic medicine, wasn’t interested in dwelling on his own fate. Instead, he wanted to reimagine reality. Well known among his colleagues for his “What if?” thought experiments, Gambhir took the occasion of my writing about the end of his life to reflect on the limits of writing itself. “I see writing as a primitive form of communication,” he declared in his commanding nasal voice. If Homo sapiens had evolved from the beginning with modern-day video and audio technologies, he surmised, there would have been little need to perfect written communication—and we’d be all the better for it today. The moment was classic Gambhir. His riff was admittedly absurd, but it was meant as provocative speculation. He had made a career out of spinning outlandish visions into realities. Working at the nexus of medicine, physics, and engineering, he had spent nearly 40 years masterminding ways to see and study the infinitesimal biochemical and cellular events in living people—something that had never been done before. The goal of his research: cancer detection. Over some 700 scientific papers and 40 patents, Gambhir, a physician-scientist at the Stanford University School of Medicine and a principal investigator in the massive health-monitoring research endeavor Project Baseline, had pioneered steps toward finding the earliest, currently unfindable, cancer cells before they had a chance to spread. Then, in the spring of 2019, his pursuit took on unanticipated urgency. His own bone marrow was seeded with a metastasis that had migrated from an unknown site somewhere in his body. Gambhir convened a scientific all-star team from around the globe, but even they couldn’t figure out the source. Medicine calls this rare malignancy “carcinoma of unknown primary”—a sad, darkly poetic, and, in Gambhir’s case, tragically apt name. The median survival time after diagnosis is three to four months. Gambhir made it 16 months. On July 18, he died at the age of 57. It was a staggering blow to the field. Gambhir’s “research and innovations have, with no uncertainty, founded modern medicine’s approach to early disease diagnostics,” said Lloyd Minor, the dean of the Stanford University School of Medicine, in a statement after Gambhir’s death. Last month, the Journal of Nuclear Medicine, a highly influential publication that has always featured on its covers spectral images of human scans or incomprehensible graphs from scientific papers, ran a tender, full-page photo of Gambhir, his dark eyes full of curiosity, his expression serene—the journal’s first cover with a flesh-and-blood human being. Over the last year of his life, I had four probing interviews with Gambhir about his work and his life; I also spoke with his colleagues and with his wife, Aruna Gambhir, a biotech executive. These were the last formal interviews that Gambhir granted. What he gave me was an intimate portrait of a vast mind coming to terms with the limits of his own place in his grand perspective. Gambhir’s discoveries opened radically new directions in cancer medicine. But, like so many visionaries, Gambhir carried the burden of knowing that he would not live to see his full aspirations become reality. Right up to the end, his cancer remained a medical mystery. In cancer treatment, timing is everything. With many tumors, there is a lag of 20 years or more between the first cancer cell and the onset of end-stage disease. Most cancer therapies ultimately fail for a simple reason: They aren’t applied until after a cancer is discoverable by conventional diagnostics—which is usually too late. When cancer cells emerge, they are confined to a single small site and are homogeneous, making them good targets for drug treatments. But as the cells proliferate and spread, they mutate. Standard chemotherapy kills the most vulnerable cells, leaving those that have evolved genetic defenses to survive and multiply. Cutting-edge treatments such as immunotherapies, which have been celebrated in mainstream-news reports for miraculously melting away advanced cancers revealed by conventional diagnostics, are undeniably valuable when they succeed, but they vary widely in their outcomes and can cause life-threatening side effects. Gambhir’s revolutionary ambition was to erase the long, silent, lethal interval between the first deviant cell and a grim lab report. Rather than curing cancer once it had already spread, he wanted to stop the first abnormal cells from ever gaining ground. To achieve this almost inconceivable goal, he proposed developing ways to monitor people while they are still healthy, in order to catch the earliest, subtle transition to disease. If surgeons could pinpoint a tiny mass of aberrant cells, smaller than the tip of a ballpoint pen, he explained, they could easily remove it before it had a chance to spread and cause irreversible harm. In our first conversation, in June 2019, Gambhir likened cancer progression to a movie that we glimpse in only a few scattered frames—or “snapshots,” as he called them—near the end. “We need the whole cancer movie,” he said, including footage of the very first rogue cells. In his lab, he searched for telltale biomarkers from cells that have started to careen out of control—faint biological signals deep in the body such as proteins, DNA or RNA, circulating tumor cells, or immune cells. He called this signal capturing “remote sensing,” invoking astrophysicists’ use of the term when trying to understand what’s going on in a star millions of light years away. As recently as the 1990s, when less was known about cancer biology and when radiological techniques were less sensitive, the notion of intercepting nascent tumors would have struck most scientists as outrageous. Gambhir was repeatedly rejected for research grants early in his career. But at UCLA, where he started out, and then more extensively at Stanford, Gambhir and his team built instruments to record an individual’s cancer movie. Among his lab’s fantastical creations: a slender magnetic wire that can sample the body’s entire blood supply and snag stray cells sloughed off by otherwise elusive tumors, and a “smart toilet” that analyzes urine and stool to detect biomarkers of colorectal cancer, a potential alternative to colonoscopies. In the works: a photo-acoustic smart bra that enables doctors to “hear light” reflected by newly forming blood vessels around a microscopic breast tumor. These devices were just the beginning. Gambhir foresaw a time when a patient would swallow a pill, the contents of which would enter all of the body’s cells and, should they encounter a cancer cell, send up the equivalent of a biological flare. He predicted that within 40 or 50 years, the annual physical will be a quaint relic, because we will instead be surrounded by passive health trackers in our homes and cars and wearable devices, including bedsheets that gauge heart and lung function, mirrors that measure vital signs using radar, toothbrushes that biochemically probe saliva, and even sensors that can register “smellprints” of lung and ovarian cancer. Gambhir’s ultimate vision was a bioinformatician’s dream—though perhaps a dystopia to anyone troubled by the prospect of being surveilled by their bedsheets. He conjured up always-on technology that monitors the entire body, just as jet engines’ hundreds of sensors continually generate real-time data during flight. “Imagine a cockpit where … you can see the status of each and every cell of our trillions of cells,” he told me. “To me, that’s not impossible.” Prevention can be a hard sell. Unlike cures, which are dramatic and definable—and, therefore, attractive investments—staving off disease in the first place is uneventful and vague, because nothing happens. Even for much of the scientific community, preempting diseases like cancer through continuous passive surveillance is a risky bet. How can the results—essentially, nonevents—be measured? How much evidence would it take to prove the concept? As scientists scramble to compete for federal grants doled out at ever-shrinking pay lines, who would bet their careers on such an untested path? In fiscal year 2018, the most recent period for which information is available, only 5.7 percent of the National Cancer Institute budget was allotted to prevention and control, even though cancer is poised to be the leading cause of death in the United States (surpassing heart disease) and, later in this century, around the world. That dilemma has led many scientists to seek deep-pocketed private investment, and Gambhir was no exception. As a leader of Project Baseline, he helmed what is likely to be the most expensive collaborative study (estimated to be upward of $100 million) ever undertaken by the academy and industry, with participating institutions that include Stanford University and Duke University, as well as Verily, the life-science division of Google’s parent company, Alphabet. Launched in 2017, Project Baseline will eventually follow 10,000 volunteers across the U.S. for four years, monitoring scores of biological functions through an extensive battery of tests, home sensors, and wearables. The study’s aim: to describe in minute detail each individual’s healthy “baseline” or threshold, and how it imperceptibly shifts to disease. Privacy experts have raised issues around the use of medical data for commercial purposes. Earlier this year, for instance, Verily sparked concerns about data collection when it used the Project Baseline platform to roll out a much-discussed coronavirus-screening website. Gambhir was acutely aware of the danger. According to his colleagues, he stipulated that Project Baseline data be stored under the strongest possible security. He also recognized that standards and regulations for data sharing, confidentiality, and privacy would take years to come to fruition. This was a common tension throughout Gambhir’s career: a crystal-clear sense of where he was going, with an agonizingly complete understanding of the obstacles that would need to be overcome to get there. Cyriac Roeding, the CEO of the cancer-detection biotech company Earli Inc., told the hundreds of mourners at Gambhir’s memorial service that Gambhir once warned him, “The world of biology will always find a way to screw you over. It will be harder than you want, and it will take longer than you want.” Yet Gambhir always seemed content to wait. Naive or not, he had faith that society would catch up with technology. One of his mantras was “We’re in the field of research, not search. The prefix ‘re-’ is extremely important.” As he told me, “The secret is not to give up, to take those decades and not look for short-term gratification, because most of the time, you won’t get lucky.” In the last months of his life, Gambhir acknowledged that his own luck had run out. “I tell my wife, ‘If I just had more time, I know I could solve this,’” he told me last fall. I asked him how much time he would need to solve his own cancer case. His answer, fittingly, was “decades.” This was not the first time for Gambhir that the gap between his futuristic vision and the present came with tragic personal consequences. When he and I met in November, he wore a thin, red, braided cloth bracelet: the kalava, a symbol of protection in Hinduism. “I’m not a religious person at all,” he said, gazing down at his wrist. “It’s a connection to my son.” In 2015, Sam and Aruna Gambhir lost their only child, 16-year-old Milan, to an aggressive and highly lethal brain tumor called glioblastoma multiforme, one of the many cancers that Gambhir had been studying at the time in his lab. As the Gambhir family learned afterward, Milan’s cancer was likely tied to Li-Fraumeni syndrome, a rare, inherited condition caused by a genetic mutation that dramatically raises the risk of many types of cancer. The mutation was passed down from Aruna, who has twice battled breast cancer as a result of the DNA defect. “If [Milan] had been born 100 years from now,” Gambhir said in a 2018 talk, “the tools of precision health would possibly have allowed him to live much, much longer.” In the final months of Milan’s life, Gambhir confided to family members and close friends that he felt as if his mind had “opened.” His scientific imagination, already expansive, seemed to stretch even further, with an invigorated sense of purpose. Unlike Milan, Gambhir carried no family history of cancer, so he had no reason to expect that the many productive years he had left in his career would be cut short. “I thought we had had enough random bullets with our son,” he told me. Still, he said, it had been easier to come to terms with his own untimely diagnosis than with his child’s. “When your son’s life is at stake, it’s even more than your own life.” Just before Thanksgiving last year, Gambhir learned that the cancer that had been confined to his bone marrow had spread. He was in severe pain. “I’m back to square one,” he told me by phone in December. “Just have to bear through it.” By January, it was obvious that his cancer had metastasized. As the coronavirus pandemic seeded itself around the world, Gambhir entered his own medical lockdown, sequestered at home as he cycled over the subsequent months through different chemo regimens, suffering toxic reactions to almost all of them. “With Sanjiv, the problem was that he knew too much … But he still had hope,” Aruna told me in August. “He was fighting until the very end.” Early in our conversations, Gambhir admitted that living in the present moment—that earnest cultural cliché—was “a foreign concept” to him. Later in our talks, I mentioned that the idea of time, in all of its dimensions, seemed to course through his work. He agreed. “The part that humans can’t comprehend—and I myself have a difficult time comprehending it—is time. We are a tiny speck in this massive universal clock.” That enormity, he added, worked against him. “It’s frustrating, because from the pure scientific-discovery part, you would like to be able to … [go] back to that full movie.” “Do you mean the cancer movie or another movie?” I asked. “The cancer movie, the life movie, the universal-clock movie,” he said. He was skipping across temporal scales, as if to say that great science requires a kind of God’s-eye view of existence, intimate and infinite—though, empiricist that he was, he didn’t believe in God. “Boy, what I’d do to have a peek into what things’ll be like hundreds, if not thousands, of years out,” he said. Gambhir called the medical revolution that he inspired “inevitable.” And though the revolution came too late to save his own life, it will, by the end of this century, save countless others from premature death—the time horizon on which he had always set his sights. from https://ift.tt/3o2NrUO Check out http://natthash.tumblr.com Before COVID-19 upended our lives, clinical vaccine trials typically made news only when they were done—when scientists could definitively say Yes, this one works or No, it doesn’t. These days, every step of the COVID-19 vaccine-development process comes under intense public scrutiny: This vaccine works in monkeys! It’s safe in the 45 people who have gotten it! The entire trial is on pause because one participant got sick, but we don’t know yet whether the person got a vaccine or a placebo! “Never before have there been vaccine trials that have been followed so closely from inception to onset to conduct,” Dan Barouch, a vaccine researcher at Harvard and collaborator on Johnson & Johnson’s vaccine, says. Over the next few months, the companies behind the leading vaccine candidates will start releasing the first data from large clinical trials. Most likely, they will not be unalloyed good news or bad news. Keeping expectations measured will require understanding when a vaccine clears just one of many hurdles—it doesn't have to be perfect, but it must be good enough. Clinical trials usually follow three phases, with the first two focused on questions of safety and dosing. By Phase III, a vaccine should already be proven safe for most people, which leads to the key question: How well does it actually work? Five vaccines—from Pfizer, Moderna, AstraZeneca, Johnson & Johnson, and Novavax—have already begun or are beginning Phase III trials that seek to recruit tens of thousands of volunteers in the U.S. Phase III trials are always large, but the ones for COVID-19 vaccines are especially so, Ruth Karron, the director of the Johns Hopkins Center for Immunization Research, says. Vaccine trials depend on volunteers getting exposed to COVID-19 as they live their life: The incidence of illness in the treatment group compared with the placebo group shows how effective the vaccine is. A normal vaccine trial might recruit 3,000 to 6,000 volunteers, but could run for years. We don’t have that kind of time with COVID-19. Each trial plans for a certain number of COVID-19 infections, and to hit that number, companies can either wait a long time for fewer volunteers to get naturally infected or they can recruit lots and lots of volunteers, which is what they’ve done. “We want to be able to detect an efficacy signal as quickly as possible,” Karron says. The public now knows exactly how many infections these COVID-19 trials are planning for—and how many would trigger an interim analysis of early data. In an unprecedented but much-applauded move, the leading vaccine companies have released detailed trial protocols. Moderna, for example, will conduct two interim analyses at around 53 and 106 infections. AstraZeneca is doing one at around 75 cases. Pfizer is doing four at 32, 62, 92, and 120 cases. “Pfizer’s, from what I can see, is the most aggressive,” Derek Lowe, a chemist who writes about drug discovery for his blog, In the Pipeline, says. Companies are not required to release interim analyses, but they might in this case, given the extraordinary public interest in a COVID-19 vaccine; promising results could also be the basis for applying for an emergency use authorization from the Food and Drug Administration. This is why Pfizer was the only company to once suggest that its vaccine might be authorized before the election--though it has since said it will wait until at least mid-November to finish collecting safety data. Pfizer is still likely to be the first out of the gate with interim results on efficacy. “I very much hope that Pfizer does their first interim, and it kicks ass. But who knows?” Lowe says. “They also then have a better chance of doing an interim readout and having it not quite come out as strong as they want it, because they’re doing it earlier.” With such small numbers—the first interim analysis will occur after only 32 infections—it may still be unclear how well the vaccine actually protects against disease. If most of the infections are in the placebo group—say 26 out of 32—that would suggest the vaccine is at least 76 percent effective. That’d be pretty good. But scientists have cautioned that a COVID-19 vaccine might be less effective than we’d like, based on how vaccines against respiratory viruses tend to work. The FDA has set a minimum bar of at least 50 percent efficacy for a COVID-19 vaccine. It’ll take longer and more cases for trials to reach a conclusion if vaccine efficacy is on the lower side. So if the first interim results are a little disappointing, that “doesn’t mean this is a failed vaccine,” Lowe says. “We’re just going to keep on rolling.” We’ll have a better idea of efficacy once we’ve seen how the vaccine performs in more people. Conversely, it shouldn’t come as a shock if some of these vaccine candidates do turn out to be ineffective. The development process from Phase I to II to III has gone very smoothly so far. But, in general, more than 90 percent of drugs and treatments fail, and close to 50 percent of them fail in Phase III. Lowe says he expects COVID-19 vaccine candidates to do much better because scientists are building on research into MERS and SARS, two related coronaviruses. But the whole point of conducting clinical trials is to find out if a vaccine works, so we shouldn’t expect them all to succeed. With 46 vaccine candidates already in clinical trials around the world, scientists are optimistic that at least some will be effective. The other big question, of course, is one of safety. The smaller Phase I and Phase II vaccine trials have so far found adverse events including fatigue, chills, headache, and pain at the injection site. But the big Phase III trials are meant to find rarer adverse events that might turn up in only, say, one in 10,000 people. That’s one advantage of these unusually large Phase III studies. Then again, volunteers might get sick for unrelated reasons, too, and any connection to the vaccine can be tricky to determine. With all the Phase III trials going on, “you're talking about hundreds of thousands of people, some of whom are elderly, over a prolonged period of time,” Barouch says. “So there will be heart attacks. There will be strokes. There will be cancers. There will be neurological events.” A serious adverse event—like a neurological disorder—triggers a study pause and a review by an independent data and safety monitoring board. This board is made up of scientists who do not work for the vaccine company and are not investigators for the trial itself. First, they would “unblind,” to figure out whether the person got a vaccine or a placebo. And if the participant got the vaccine, the board might seek additional medical records and data to look for any possible link between the vaccine and adverse event. The AstraZeneca and Johnson & Johnson vaccine trials are currently halted for this reason in the U.S., though AstraZeneca’s has since resumed in other parts of the world. These pauses are relatively common with vaccines, which have a very high safety bar because they, unlike drugs, are given to healthy people. Normally, a pause doesn’t become public if the trial is resumed, but COVID-19 vaccines are under special scrutiny. “Hearing there is a pause means the system is working,” Karron says, because it means safety concerns are being investigated. Recruiting large numbers of volunteers speeds up the trials significantly, but investigators will still have to wait to understand a vaccine’s long-term safety. While normal vaccine trials might run for years before going to the FDA, the agency says it will require at least two months’ worth of follow-up data before authorizing a COVID-19 vaccine for emergency use. (Emergency use authorization or EUA is a lower bar than formal approval.) Peter Marks, the director of the FDA division responsible for vaccines, has said that this time frame was chosen because most adverse events show up by the two-month mark. Experts agree that this is reasonable, given the pandemic, but regulators will continue monitoring the vaccine’s safety after emergency authorization and approval. When COVID-19 vaccines are eventually given to millions of Americans, some number of extremely rare—literally one-in-a-million—events will occur. The flu vaccine, for example, is linked to one or two additional cases of a rare neurological disorder called Guillain-Barré syndrome for every 1 million doses administered. But public-health officials weigh that risk against the 12,000 to 61,000 people who die of seasonal flu every year in the U.S. With the FDA’s two months of required safety data, mid-November is the earliest companies might seek emergency approval for a COVID-19 vaccine, assuming the required number of infections is met. The interim data in a small number of people may or may not offer clear results, but the bigger picture is worth keeping in mind: Many, many candidates are in the pipeline. The first vaccine will make news, but it might not be the most effective, the easiest to deploy, or ultimately even the most widely used. from https://ift.tt/37jRAOb Check out http://natthash.tumblr.com |
Authorhttp://natthash.tumblr.com Archives
April 2023
Categories |
 RSS Feed
RSS Feed
