|
Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. Americans’ social lifelines are beginning to fray. As the temperature drops and the gray twilight arrives earlier each day, comfortably mingling outside during the pandemic is getting more difficult across much of the country. For many people, it’s already impossible. To combat the loneliness of winter, some of us might be tempted to turn to pods, otherwise known as bubbles. The basic idea is that people who don’t live together can still spend time together indoors, as long as their pod stays small and exclusive. And pods aren’t just for the winter: Since March, parents have formed child-care bubbles. Third graders have been assigned to learning pods. Some NBA teams were in a bubble for months. A July survey of 1,000 Americans found that 47 percent said they were in a bubble. In theory, a bubble is meant to limit the spread of the coronavirus by trapping it in small groups of people and preventing it from jumping out. “The goal here with an infectious agent like SARS-CoV-2 is that you want to try and not give it hosts,” Keri Althoff, an epidemiologist at Johns Hopkins University, told me. “That’s the name of the game.” Earlier this year, researchers modeled the best ways to flatten the curve by limiting social interactions and found that having people interact with only the same few contacts over and over again was the most effective approach. But the details of how exactly to go about podding can be hard to pin down. The answers to some basic questions—how many people should be in a bubble? what’s okay for the members of a pod to do together?—are still unclear. For example, Beth McGraw, the director of the Center for Infectious Disease Dynamics at Penn State, suggests including 10 or fewer people who live in just a handful of households, but she and all of the experts I spoke with for this story emphasized that there’s no magic number that makes a group safe or unsafe. [Read: The difference between feeling safe and being safe] Bubbles might sound great—you can have your friends and your safety too!—but they don’t always work out the way they’re supposed to. Some pods are enormous. Some are open to an untold number of people’s germs through contacts of contacts (of contacts of contacts of contacts). “I think there’s leakage in a lot of people’s pods,” Whitney Robinson, an epidemiologist at the University of North Carolina, told me. Last week, a New York Times columnist examined the ties in his bubble and found that he was connected to more than 100 people—and that’s just whom he was able to trace. No public-health scheme is perfect, and we will need to layer as many of them as we can in order to survive the pandemic. But with pods, the country hasn’t even settled on a shared definition. If we do not reach a consensus on best bubbling practices soon, we risk blasting a hole in one layer of our armor and opening ourselves up as a nation to even more unnecessary sickness and death. This month, I spoke with five Americans about their pandemic pods. I reached out to them because they had talked in local media or on Twitter about their bubbles. Their strategies are by no means reflective of the entire country’s experience, but even within this small sample of middle-aged city dwellers and suburbanites, their behaviors were shockingly dissimilar. The deeper I probed, the more meaningless the terms pod and bubble seemed. Everyone was on more or less the same page as to the basics of the arrangement: Pod members interact with one another indoors without masks for extended periods of time, and do not do so with people outside the pod. But beyond that, they described practices that in some cases bore little resemblance to one another. Three of the bubbles I heard about are closed: No one on the inside has close contact with people on the outside, so with the exception of encounters in grocery stores and other public places, everyone knows exactly how many people they’re exposed to. John Skvasik, a 41-year-old librarian who lives in suburban Cleveland, is in a three-person pod with his 70-year-old mother and his uncle. (Skvasik spends 32 hours a week in the library, but he and his co-workers are all masked.) Stacy Selby, a 40-year-old who lives in Seattle and uses they/them pronouns, is in a 10-person bubble with the extended family of the children they nanny. Innosanto Nagara, a 50-year-old graphic designer and children’s-book author in Oakland, California, formed a “germ pod” of 16 with his wife and kids, his mother-in-law, and three other families who live on the same block. Other pods aren’t so self-contained. Jen Angel, a 45-year-old who lives in Oakland and owns a bakery (she was mixing vanilla-buttercream icing while we talked), has adopted a different strategy with her six housemates. Each of them is allowed to interact indoors and unmasked with a couple of their “most important people.” But there are no limits on the number of people those contacts see, or who those contacts’ contacts can mix with. Angel and her housemates meet weekly to go over the pod rules and map out everyone’s contacts and contacts’ contacts. As of last week, their most recent map included 35 people, and that didn’t include the unknown number of more distantly connected contacts. [Read: The most American COVID-19 failure yet] The podders I spoke with also had very different standards for rule making and communication. Angel’s house, for example, has a Google Doc of agreements (“wash your hands as soon as you enter the house,” “immediately report exposures or symptoms to the rest of the pod”). Selby’s nannying contract includes a list of permitted activities. But some groups don’t have formal agreements at all. Sue Loh, a 44-year-old programmer and software developer who lives outside Seattle, told me that she considers her children’s nanny to be part of her household (she prefers household to pod or bubble because her family and her nanny are interacting for practical, not social, reasons). But Loh hasn’t asked her nanny or her nanny’s family to “limit their behavior at all,” she said, because “we just know from her own behavior that it’s probably not any more risk than we’re already taking.” By any strict definition, Loh’s and Angel’s groups are not bubbles at all, because they’re not closed networks. Open pods aren’t useless, especially if everyone is good about wearing masks, but they’re still riskier than a self-contained pod, no matter how pandemic-conscious members are in the rest of their life. “As soon as you sort of break your bubble, the connections can be infinite. And this is how [the virus] spreads,” McGraw, of Penn State’s Center for Infectious Disease Dynamics, said. The leakiness might be even more dangerous when bubble buddies don’t realize it’s a problem. “We get into trouble when people maybe think they’re in a pod, but some recommendation is being violated,” Meghan Moran, an associate professor of health, behavior, and society at Johns Hopkins, told me. That could lead to “a false sense of security,” further endangering people in the group. In other words, not only do some pods keep their members safer than others, but the very premise of safety can also put pod members at risk. Why, then, aren’t we all keeping our pods closed tight? Some variation in how Americans form their pods is unavoidable and even healthy. Local transmission rates, for example, can be used to inform best practices, and people in different living and work situations will come up with different solutions to the problem of how to socialize in a pandemic. But inconsistent or nonexistent messaging is undeniably playing a role in the confusion. For a concept that’s so important and widespread, health experts and the government have given remarkably little direct advice to the public. When I checked the CDC’s website for official resources on how to safely form a pandemic pod, I came up empty. (The agency did not respond when I asked whether such resources existed.) There are no guidelines to be found on the White House’s website or President-elect Joe Biden’s. Compare the treatment of the pod concept in the United States with that in New Zealand, where Prime Minister Jacinda Ardern used the word bubble in a briefing on March 24, and where the government’s coronavirus alert system clearly delineates what Kiwis should do with their bubbles at different restriction levels. [Read: The simple rule that could keep COVID-19 deaths down] The timing of Americans’ pivot to bubbles could also be a factor in our general confusion. When Ardern started talking about the strategy, New Zealand was preparing for winter in the Southern Hemisphere and needed to deal with the imminent threat posed by the indoors. But, as the experts I spoke with explained, in the U.S., the public-health guidance since the spring has generally shifted from an abstinence mindset of shunning the company of anyone you don’t live with to a focus on keeping your distance outdoors. Bubble and pod have also run into the same communication pitfalls as social distancing, quarantine, and a host of other new and reappropriated terms this year. Inventing new words or phrases is always a gamble: Their creators have relative control over their meaning, but the verbiage might not catch on. (When I asked UNC’s Robinson to think of a new, alternative phrase to replace pod, she thought for a moment before answering, “Closed behavioral network is not catchy. This is why academics are not good at making things up.”) Pod and bubble “resonate because they conjure up some kind of image for us,” Moran said, “which causes us to maybe assume we know what it means. But without that deeper level of understanding, different folks may be using the same term in very different ways, which can lead to misunderstandings.” Such mistaken assumptions are why Robinson prefers bubble to pod: She said that bubble evokes a more concrete image of a closed object with a defined inside and outside, whereas pod is more ambiguous. [Read: The logic of pandemic restrictions is falling apart] Under ideal circumstances, anyone trying to teach the American public a new health concept would follow a long, iterative process of creation, testing, and review. This is generally easier to do if you’re trying to address chronic health conditions, rather than a virus that is killing 1,500 people a day. But the coronavirus has presented public-health experts with the worst of both worlds: They need pandemic-fatigued Americans to adopt lasting behaviors for the remaining months until a vaccine can be distributed, but they can’t test their catchphrases as thoroughly as they’d like. This tension could explain some of the communication failures around bubbles: Messages that aren’t as carefully planned and tested as their creators would like have less of a chance of reaching—and inspiring helpful behaviors in—their audience. With winter fast approaching, Americans need pods now more than ever. But pods have also never been more dangerous. As with so many efforts to rein in the pandemic, a bubble strategy would be much easier to implement if viral spread were at least relatively under control. Instead, new cases and hospitalizations in the U.S. are higher than they’ve ever been, and deaths are also poised to break this spring’s horrifying records. According to Althoff, the Johns Hopkins epidemiologist, the higher transmission rates are, the more likely people are to get infected, and the higher the chances that the virus sneaks its way into any given pod. Still, podding has its benefits, even when implemented less than perfectly and in less than perfect environments. Forming a pod can be an impetus for having conversations about what constitutes acceptable COVID-19 risk within a household or family. And those conversations can make the burden of navigating winter a bit lighter on everyone. “A hard thing about the pandemic is the feeling that you have to negotiate every interaction with someone, and that’s really exhausting mentally,” Robinson said. Talking about pod rules is a way to pre-negotiate, so that when you interact with people, you can focus more attention on the pleasure of their company. [Juliette Kayyem: The emotionally challenging next phase of the pandemic] Talking about pods and bubbles might seem like more trouble than it’s worth, but it is, at the very least, a starting point for considering the consequences of our behaviors. As Robinson said, it’s “a chance to acknowledge that our dependence on each other has changed.” None of us should be shamed for relying on people we don’t live with, or for wanting to maintain our emotional health. We need one another. But we also need one another to exercise caution and restraint so that thousands more will not die in the name of preserving the nation’s social well-being. from https://ift.tt/3fNTsks Check out http://natthash.tumblr.com
0 Comments
At 4:30 a.m. on the Monday before Thanksgiving, the dry-ice manufacturing floor at Noble Gas Solutions in Albany, New York, was hopping. The machine that compresses carbon-dioxide gas into dry ice was cranking out pellets of the stuff—1,500 pounds an hour—and Noble’s staff was racing to fill hundreds of bags so that a mission-critical product could be distributed on an unforgiving deadline. The product: cheesecake. The deadline: Thanksgiving dinner. “We have a business just 10 minutes down the road that distributes cheesecakes all over the country,” Noble’s vice president of operations, Robert Kohler, told me. After a burst of orders, the company needed more than a ton of dry ice, divided into six-pound bags that could be dropped into shipping boxes alongside the cheesecake, to keep it cold all the way to doorsteps across the country. “They wanted their first delivery at 6 a.m. on Monday. We normally don’t even open until 7 a.m.” Dry ice often helps save Thanksgiving, even if the beneficiaries of its special magic may not notice. But this winter, it will help save the world from the coronavirus pandemic. A senior salesperson for Noble, which routinely supplies the pharmaceutical industry, had just taken a call from an official with the state of New York, assessing how much dry ice Noble might be able to supply, on short notice, in order to get the first coronavirus vaccine out to every corner of the state once it is approved. That vaccine, the work of a partnership between Pfizer and BioNTech, is likely to be the first approved by the FDA. It is so delicate that it has to be kept at –70 degrees Celsius (–94 degrees Fahrenheit). That’s not just colder than most freezers; it’s colder than winter at the South Pole. But holding that temperature is not a problem for dry ice, which is a solid at –78 degrees Celsius (–109 degrees Fahrenheit). In fact, for shipping Pfizer’s coronavirus vaccine, nothing else is practical besides dry ice. “There’s really no other way to maintain that temperature stability in transit,” says Azra Behlim, a medical-supply-chain expert at Vizient, a health-care consultancy. The nation’s dry-ice makers aim to be ready. “We’re getting bombarded with inquiries by hospital districts and public-health departments,” says one employee at a dry-ice supplier, who requested anonymity because he isn’t authorized to speak to the press. Airgas—one of the nation’s largest dry ice companies, with 15 manufacturing sites and 60 distribution centers—is collaborating with the federal government’s vaccine-logistics effort, Operation Warp Speed. “We formed teams to evaluate everything that’s needed throughout the supply chain: How much dry ice might be needed, in different geographies, with different populations. Ensuring the logistics are in place,” says David Joyner, Airgas’s senior director for carbon dioxide. The dry ice planning, says Joyner, is similar to what Airgas did to keep hospitals supplied with medical oxygen during the peak demand in the spring, when the company set up a daily task force to monitor oxygen demand and make sure hospitals got what they needed. On the other end of the size spectrum are companies like Noble. “We’re currently a one-shift operation,” says Noble’s CEO and owner, Dave Mahoney. “But if the need is there, we can work around the clock if we have to. And if we need to be here around the clock—that’s a good problem to have. It’s just rewarding to know we can be part of the solution to the pandemic.” Dry ice has long been an indispensable, if mostly invisible, ingredient in the economy. Farmers clean out their wells with it. Cities blast graffiti off walls and statues with it. The nation’s largest meat companies mix it right into their products as they grind them, to keep the temperature safe and the fat from gumming up the grinding equipment. Factories of all kinds—from those that make shoes to those that make frozen waffles—have installed jets of dry ice pellets, right on the manufacturing line, to clean molds in real time. Dry ice helped remove radioactive debris from helicopters that were used during Japan’s Fukushima Daiichi nuclear disaster in 2011. A company in Utah, Cold Sweep, has perfected using it to lift dirt off the pages and bindings of fragile antique books and manuscripts without harming them. On Broadway, at Halloween parties, and in high-school auditoriums across the country, dry ice makes for convincing theatrical “smoke.” 
Dry ice is made by taking purified CO2 gas, chilling it, and pressurizing it to the point that it’s a liquid, then releasing the pressure, which causes the liquid CO2 to take on a snowflake-like consistency. It is then turned into blocks, or into pellets that look like foam shipping peanuts. For cleaning, the dry ice is made into tiny beads the size of rice grains, or smaller. Companies use these like you would use sand-blasting pellets, but once you’ve “dry-ice blasted” a gas turbine, or a mold for making frozen waffles, or the graffiti off a wall, you have no mess to clean up—the dry ice does the cleaning, then simply disappears into the air. Most of the dry ice in the U.S. is made with waste from other kinds of manufacturing—ethanol plants, ammonia and fertilizer factories, and oil refineries produce CO2 as a byproduct, and many capture it to sell to other industrial users. Some of the nation’s biggest dry-ice makers, in fact, colocate their plants adjacent to those facilities, to make using the gas as easy as possible. “It’s kind of an amazing product,” says Buddy Collen, the general manager for Reliant Dry Ice, which has six dry-ice manufacturing plants across the southern and western U.S. Collen has been in the dry-ice business for 42 years. “It’s really very simple—it’s just carbon dioxide in solid form. That’s it. But there continue to be new applications for it that come along all the time.” Read: [Vaccine chaos is looming] The Pfizer/BioNTech vaccine is on track to win emergency approval around mid-December from the FDA, and if it does, Pfizer has estimated it could provide 25 million vaccine doses, distributed in tiny glass vials, to the U.S. by the end of the year. The vaccine will be distributed in specially designed shipping cases, each a little bigger than a carry-on suitcase, that hold up to 5,000 doses each. Just for the U.S., that’s more than 5,000 cases—and each case requires 50 pounds of dry ice to keep the vaccine inside frozen in transit. Once the cases reach the hospitals or medical centers that will administer the vaccine, they need to be “recharged” with 50 pounds of dry ice every five days, unless the hospital has an ultracold freezer that goes down to –70 degrees Celsius. The vaccine is itself the product of a taut, complicated supply chain. Raw materials are made in St. Louis. The crucial, and revolutionary, messenger-RNA components are made in Andover, Massachusetts. The elements come together for finishing and packaging at Pfizer’s factory in Kalamazoo, Michigan. All three sites have been working furiously for months making the vaccine, so they would be ready if trials proved it safe and effective. It’s one of the distinctive, and expensive, approaches pharmaceutical companies have taken to this pandemic: producing large quantities of vaccines whose value isn’t yet known, in case they turn out to work. That is why Pfizer (and Moderna, whose vaccine is stable at standard refrigerator temperature) will be able to deliver millions of vaccine doses before the end of the year, starting within days of any approval. But the dry ice that will make getting the Pfizer vaccine into people’s arms possible can’t be made in advance. Dry ice has many curious qualities, and one of them is that it is devilishly hard to store. As soon as you make it, it starts to disappear. “Every weekend, I always have one 1,500-pound bin full of dry ice, in stock, for an emergency,” Noble’s Kohler said. “When we come in on Monday, we’ve lost 200 pounds of that 1,500-pound bin.” Carbon dioxide is never liquid at room temperature and ordinary pressure. Which means dry ice doesn’t melt—it goes directly from being solid back to being a gas, in a process called sublimation. That’s precisely why it is so appealing as a source of “smoke.” It’s also why Kohler’s weekend emergency supply of dry ice, even when stored in an insulated bin, goes from 1,500 pounds to 1,300 pounds over two days. The sublimation is, to some degree, dangerous—CO2 is heavier than oxygen, to the degree that it carries with it a suffocation hazard. Another node in the great logistical web of America’s vaccine rollout: Shipping companies have to take extra care in flying large loads of Pfizer’s dry-ice-packed vaccine boxes, so the CO2 doesn’t escape and overcome flight crews. The Federal Aviation Administration has had to give FedEx special guidance to increase their capacity. Operation Warp Speed has, in the past two weeks, promised to deliver the initial 50 pounds of dry ice to resupply Pfzier’s vaccine cartons to every location that receives the vaccine and doesn’t have a freezer, at the same time as the vaccine itself arrives, via FedEx or UPS. The vaccine supplies can be stored in Pfizer’s shipping container for another 15 days, if the dry ice is replaced every five days. But if it is to stay frozen, Pfizer says, the box can only be opened twice a day to remove supplies, and then for no more than three minutes each time. The vaccine can be thawed and held at an ordinary refrigerator temperature—2 to 8 degrees Celsius (36 to 46 degrees Fahrenheit)—for five additional days. So the people who get a container of vaccine will have to plan their need for the vaccine carefully. And because of dry ice’s perishability, once Pfizer’s vaccine is approved, it will set off a furious race to make enough dry ice to ensure the vaccine stays cold as long as it needs to. Margaret Mary Health is going to need dry ice. Consisting of a hospital and outlying clinics in four different towns, the system serves a rural area of southeastern Indiana between Cincinnati and Indianapolis, centered in Batesville. The hospital is small, but busy. Last year the ER saw 19,000 patients, and the hospital delivered 500 babies. Before the pandemic, the hospital was licensed for 25 beds, but it’s now allowed to exceed that capacity; earlier this week, it had admitted 30 patients, 13 with COVID-19. Margaret Mary is one of around 50 hospitals that Indiana has chosen to administer the first round of coronavirus vaccines, which will go to health-care workers. So if the Pfizer vaccine is approved, it will have responsibility for vaccinating hundreds of health-care workers across a five-county region covering 1,400 square miles. Margaret Mary doesn’t have an ultracold freezer. It also doesn’t have easy access to dry ice—it not only doesn’t use it routinely, it has never bought any. And there isn’t any nearby. In fact, “there are no dry-ice suppliers in the whole five-county region,” Margaret Mary Health CEO Tim Putnam says. So members of the hospital’s vaccine-planning “strike team,” led by Geralyn Litzinger, the director of community health, have lined up three dry-ice vendors farther afield: two in Indianapolis, 65 miles west, and one in Louisville, Kentucky, 90 miles south. “We’ve tried to calculate how much vaccine we might get,” Litzinger says, “and how much dry ice we’ll need … We’re making sure we’re set up as customers with those vendors, so we can quickly place orders.” The dry ice is just one of dozens of details for a small health-care system getting ready to administer the vaccine. Litzinger and her staff are planning to administer the vaccine to health-care workers at two locations across their wide service area, one of which will be a drive-through. Last week, a team from Margaret Mary was at a fire station, testing the Wi-Fi connectivity for the computers the hospital will use to record information about every person who gets the vaccine as they roll through. Read: [‘No one is listening to us’] In terms of the dry ice and the Pfizer box, Litzinger says, “We won’t open it very often. By scheduling appointments for people to get the vaccine, we should know how many people per day—so when we do access the box, we can pull out only what we need.” Putnam says the planning at the state level has been as good as could be expected under the circumstances, though the details are always changing. The state has told rural hospitals to ask for help if they can’t secure their own dry-ice supplies. Meanwhile, America’s dry ice makers will be working overtime to make sure there’s enough dry ice for the first wave of distribution. There was, in fact, a shortage of dry ice in the spring and early summer—Americans were driving less, so ethanol plants were producing less ethanol, and thus less CO2. But the shortage has eased in most places, and many dry-ice suppliers are confident they’ll be able to support the vaccine rollout. Buddy Collen says that Reliant Dry Ice is keeping a list of health-care outlets that will need dry ice—and waiting for the moment when the vaccine is approved. “We tell them, ‘Call us back when you know what you need,’” he says. Reliant’s philosophy, Collen says, is that “we have a moral obligation to do everything we can to help make sure these vaccines get to the right places. And we will do everything we can to do that. We also have a responsibility to our existing customers, of course—for some of them, if they don’t get dry ice, they may have to shut down.” The volumes that most hospitals need—a few hundred pounds a week at most—shouldn’t strain even local dry-ice makers. The greater challenge may be getting dry ice to all those new customers, like Margaret Mary Health, who are far outside the normal distribution channels—either by setting up priority deliveries, or arranging to have hospitals and health departments come collect the dry ice themselves, with all the care transporting it requires. For a man with 42 years in the business like Collen, the sudden stardom for dry ice is bemusing. “It’s amazing that no one could care less about the dry-ice business until this year,” he says. “It’s always been a quiet business. Now everyone is talking about dry ice.” from https://ift.tt/3fHOsOd Check out http://natthash.tumblr.com Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. Recently, over the course of just one week, the Houston Health Department received more than 110,000 lab reports of COVID-19 test results. In a city of 2.3 million people, “it’s quite a high volume,” says Beau J. Mitts, the department’s bureau chief. Less than two-thirds of those lab reports flow automatically into the health department’s electronic system, according to Mitts. Another 35 percent arrive in digital form but must be imported into the city’s database, and the remainder arrive via fax. All over the country, health departments are facing such influxes, and many are struggling to keep pace. The latest surge has earned the terrible distinction of having the highest number of daily cases and hospitalizations since the pandemic began. Now data-reporting delays caused by the Thanksgiving holiday and long weekend may provide a veneer of comfort—a seeming dip in cases—when the actual course of the pandemic in the coming days will almost certainly be much bleaker than the reported numbers show. Our colleagues at the COVID Tracking Project have monitored how holidays and weekends can affect the daily reporting of tests, cases, hospitalizations, and deaths to public-health departments. As the project’s managing editor, Erin Kissane, wrote this week, the number of new COVID-19 cases reported on a Sunday or Monday—data that are actually collected on Saturday and Sunday—is typically several percentage points below the weekly average. These delays have several causes: Doctors’ offices may be closed or public-health departments may be short-staffed during the weekend, resulting in fewer tests being conducted, fewer positive cases being identified, and less data making their way onto the internet. But though the reporting infrastructure slows over weekends, the virus does not. Later in the week, the data “catch up,” with higher-than-average numbers on Thursday, Friday, and Saturday. [Read: The final pandemic surge is crashing over America] Holidays tend to bring the same delays as weekends, and Thanksgiving combines a long weekend with a holiday at the pandemic’s worst point yet. If the patterns that the COVID Tracking Project has documented over other holidays hold, in the next week, reporting will slow for a few days, then spike. While no one can say exactly how long labs will take to work through the holiday backlog, the current picture, of rapidly rising testing, cases, and deaths, could be blurred for days at a critical point in this third surge. On top of the holiday-related data delays, the offices that report coronavirus data could be dealing with a larger volume of paperwork simply because of the size of this surge—which means more people getting tests, more people going into the hospital, and more people dying. While testing has grown appreciably—in the past week, the U.S. reported an average of 1.8 million tests a day, more than double the figure from three months ago—those tests can be slow to process. That’s especially true now, as new cases exceed 170,000 a day and Americans have flocked to testing centers under the misguided notion that a negative test would magically render large Thanksgiving dinners safe. This week Quest Diagnostics, which operates labs and makes COVID-19 testing equipment, said that higher demand is resulting in delays in processing results, to two to three days for most patients. Jessica Guernsey, the public-health director for Multnomah County, Oregon, says her county began to see changes in the data before Thanksgiving. “It has more to do with the health department being overwhelmed because of sheer volume,” Guernsey says. “The system we’ve set up could be more nimble—to have the data processed and make its way into the statewide system is a fairly laborious process.” Even with bumps in the data, Guernsey warns, the numbers are going up. “I don’t think most people looking at the data would think we’re in the clear, and none of our messaging reflects that,” she says. “We’re in each other’s care right now, and we need to make decisions that are sacrificial. We’ll have to hunker down for a while to protect other people.” [Read: ‘No one is listening to us’] Because COVID-19 data can vary significantly from day to day, averages over the longer term paint a clearer picture of the disease’s trajectory. Decreases in the numbers of cases or deaths in the days surrounding Thanksgiving won’t be particularly meaningful until we have a wider view of the data, in the form of weekly averages. As Kissane notes, hospitals don’t get days off, so data about hospitalized patients are less volatile than other metrics. Nearly 90,000 people are hospitalized with COVID-19 in the United States, and that number has grown 89 percent since November 1. Any immediate post-holiday spike, driven by data delays, should not be conflated with the rise in cases that could follow still later, driven by new infections incubated by holiday travel and gatherings. Public-health officials have mostly implored Americans to stay home for the holiday, but for those who do visit Grandma, a COVID-19 infection acquired this weekend could take more than a week to appear in a public-health dashboard, says Angela Rasmussen, a virologist at the Georgetown Center for Global Health Science and Security. “The median time that people test positive is five days after exposure, but it could take up to two weeks.” A person who gets infected late this week might not display symptoms for several days (if at all); scheduling a test, and getting results back, could take several more days. “I would expect to see increases in cases one to two weeks after Thanksgiving. I would expect to see a two-to-three-week lag for hospitalizations, and then another two to three weeks for mortality to increase,” Rasmussen says. After Halloween, it took about a week to see an increase in cases, says Olivia Kasirye, the public-health officer in Sacramento County, California. “A week from this Thursday is when we’ll see an impact from the Thanksgiving holiday.” In Canada, where fewer than 12,000 people have died of COVID-19, cases rose 33 percent in the three weeks after the country celebrated Thanksgiving in mid-October. Rasmussen cautions that the current stress on the medical-care system now makes any hospital trip more dangerous. “When facilities and people are put under this amount of strain, it’s not just COVID that is a risk; it’s a heart attack, pancreatitis that requires emergency surgery, a car accident,” Rasmussen says. “You may find yourself in a situation where you are not able to access the kind of care that you usually would. It’s really scary.” If there is a rise in deaths following Thanksgiving, the evidence of it could be delayed even further, because of the grim math of the disease at this time of year. “Reporting of death is even more challenging,” says Ellie Murray, a Boston University epidemiologist. The bulk of Thanksgiving-related COVID-19 deaths will likely come around Christmas, she says. Confirming and reporting a death takes time, and, Murray points out, the people working in the systems that track these numbers may step back for rest and reprieve during the holiday season. “That could potentially delay the reporting even more,” she says. “We may not really have a full picture of what happened post-Thanksgiving until sometime in January.” from https://ift.tt/3nZIA61 Check out http://natthash.tumblr.com Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. In the week before Thanksgiving brings thousands of Americans through airports and travel stations and into multigenerational indoor gatherings, U.S. states have reported more than 1.2 million cases of COVID-19. The seven-day average for new cases has more than doubled since the beginning of November. The number of people currently hospitalized with the virus in the United States hit nearly 90,000 on Wednesday, breaking the national record for the 16th day in a row. As hospitals fill up across the country, deaths are also spiking. For the first time since May 7, daily reported deaths exceed 2,000 this week, first on Tuesday and again on Wednesday. In better news, growth in the number of new tests this week outpaced the number of new cases for the first time in two months. The increase in the number of reported tests may have been driven in part by people getting a COVID-19 test before traveling for the holiday. (In related news, Quest Diagnostics this week said turnaround time for lab results was rising because of the latest surge. The company also said that because so many tests are coming back positive, it is relying less on pooled testing, the practice of combining several test specimens into a batch and testing the resulting sample.) A warning to data-watchers: Over the past eight months, we have observed that the data coming from states and territories during and after weekends and holidays tend to be erratic. We expect to see this trend in full force over the holiday weekend and for several days afterward. As our managing editor, Erin Kissane, explained on Tuesday, “Holidays, like weekends, cause testing and reporting to go down and then, a few days later, to ‘catch up.’ So the data we see early next week will reflect not only actual increases in cases, tests, and deaths, but also the potentially very large backlog from the holiday.” On Wednesday, California reported 18,350 new cases, the highest single-day count for any U.S. state during the pandemic. The western state’s single-day case record is followed by Texas’s—15,609—set on the same day. California and Texas are the country’s most populous states; on a per capita basis, California’s and Texas’s case rates are unremarkable compared with the midwestern states we discuss below. Nevertheless, these are large numbers. As of yesterday afternoon, 45 of California’s 58 counties were in the state’s “purple tier,” which indicates that infections are widespread, many nonessential activities are restricted, and nonessential businesses may be closed. Los Angeles County’s director of public health this week called the region’s current case and death numbers “the most alarming metrics we’ve ever seen,” according to the Los Angeles Times. City health officials on Wednesday released a report estimating that one in 145 people in Los Angeles County--population 10 million—are infected with the coronavirus. A week ago, the report says, that metric was 1 in 250 people. In California, our COVID Racial Data Tracker shows that the Latino and Native Hawaiian/Pacific Islander communities have more than three times the cases per capita as the white population. To date, nearly 60 percent of all cases reported by California are for Latino people, who make up slightly less than 40 percent of the state’s population. More than 100,000 new cases among Latino people have been reported in the last month, and 1 in 32 Latino people in California have tested positive for COVID-19 since the pandemic began. Native Hawaiians and Pacific Islanders make up less than 1 percent of California’s population, and are similarly affected, with 1 in 33 having tested positive for COVID-19. For comparison, 1 in 99 white people have tested positive for COVID-19. (All of these figures are based on California’s confirmed case count and therefore exclude antigen testing.) In the national picture, many of the Midwest and Mountain West states we’ve been tracking closely posted very high per capita case numbers this week, with Minnesota, Montana, Nebraska, North Dakota, South Dakota, and Wyoming all exceeding 1,000 new cases per day on the seven-day average this week, along with Southwest outlier New Mexico. North Dakota has had the highest per capita number of cases of any state for 10 of the past 12 weeks. What the case map doesn’t show is a small but important change in U.S. COVID-19 data patterns this week: After three months of a consistent rise in the seven-day average of new daily cases, North Dakota’s cases began to fall. The state’s current hospitalizations, too, are declining, which means that more COVID-19 patients are leaving North Dakota’s hospitals than are entering them. We’re also seeing convincing case drops, backed by clear decreases in hospitalized patients, in Iowa, Montana, South Dakota, and Wisconsin. This change in state numbers is reflected in the regional view of new cases per capita, which shows that across the Midwest, daily new cases are declining. In the other three major regions, however, daily cases are still rising—a sign that we should expect to see hospitalizations continue to rise in much of the country for the immediate future. Hospitalizations are now 50 percent higher than they were during either the spring or summer case surges. Nearly 90,000 Americans are in the hospital with COVID-19 today. Hospitals across the country continue to experience extraordinary levels of strain. Cases have been rising in Alaska; in Anchorage, the state’s biggest city, hospitals are filling up, and one facility has opened an overflow unit, according to the Anchorage Daily News. Hospitals in Utah are approaching capacity, according to The Salt Lake Tribune; a Mayo Clinic facility in Wisconsin is placing hospital beds in an ambulance garage; and Arizona’s hospitals are running out of beds. As our long-term-care team reported in its weekly update, cases in U.S. congregate-care facilities grew enormously: States reported a 50 percent increase in new long-term-care cases—46,153 new COVID-19 cases this week alone. Long-term-care facilities recorded about 3,000 new deaths in one week. The Midwest remains the epicenter of long-term-care-facility outbreaks, accounting for 39 percent of new cases reported in the U.S. But the crisis stretches beyond the Midwest, too. This week each region of the U.S. reported its largest increase in long-term-care cases in the past four months. So far this month, long-term-care residents represent 39 percent of all U.S. COVID-19 deaths. This week, 20 percent of long-term-care-facility cases and deaths in the Midwest were reported in Illinois—the highest increase in cases in the past six months. This weekly update covers the number of tests reported, but it’s worth reminding readers that the U.S. health system administers multiple kinds of COVID-19 tests—polymerase chain reaction, or PCR, and antigen tests are the most commonly used—and our testing data do not, as a whole, distinguish among these tests. We have previously written about which states break out antigen tests from PCR tests; this week, we published a deep dive in which contributor Whet Moser explains how the two test types play different roles in an effective public-health response to the pandemic. Although we expect the holiday weekend to bring data disruptions to much of the country, we’ll be here doing our regular daily updates throughout. We wish you all a healthy and happy holiday. from https://ift.tt/3l8UKHZ Check out http://natthash.tumblr.com
Dear Dr. Hamblin, I need to see my therapist, but she isn’t doing teletherapy due to her hearing. She says she’s opening windows on both sides of her office, leaving one hour between appointments, requiring masks, and swapping the nylon cover on the couch between clients. I still don’t feel comfortable. Plus, she herself is elderly. Am I overreacting? Anonymous San Francisco, California San Francisco, You are overreacting. Because I’m not a therapist, I’ll tell you that directly, even though I understand it would be more effective to let you discover it yourself. It’s good to be cautious. About 1,700 Americans are dying from COVID-19 every day. The number is climbing quickly. Our collective problem is that most people aren’t being cautious enough. At the same time, it remains possible to be too cautious. At a certain point, caution becomes self-defeating, especially if it means missing things like important medical appointments. When in-person visits can reasonably be delayed until vaccination is widespread, that may be the safest choice, especially in places where health-care systems are overwhelmed. Many people who are young and healthy, for example, could be fine without an annual primary-care check-up this year. But keeping up with therapy is extremely important, more like a root canal than a wart removal, and even more so at a moment when the United States is seeing a surge in mental-health issues. In your case, it sounds like your therapist is doing almost everything right. She’s set up good airflow (assuming these are big windows, seriously open) and required people to wear masks (assuming these are good masks, worn well). Clinicians around the world have managed to see patients safely under similar circumstances, and even to treat people who have COVID-19 (which neither of you should knowingly have). I’m not sure about the necessity of changing the couch cover or waiting a full hour between appointments, but the measures she’s taking suggest meticulousness, which itself is a reassuring sign. The basic principle to keep in mind—for this sort of appointment and others like it—is that you want to make sure you’re in a space where the coronavirus can’t accumulate in the air. If one person is infected and talking in an enclosed space, the air in the room can gradually fill with virus. Masks help this happen more slowly, and airflow helps dilute the buildup of virus (though neither totally prevents it). Taken together, effective masks and high airflow make it extremely unlikely that you’ll be exposed to enough virus to infect you (or that you’ll infect your therapist). If her office is enormous, like an airplane hangar, then the risk is essentially zero. In a small office, a similar effect can be achieved with an air purifier that has a HEPA filter, which can clean the air of any virus every few minutes. All of that said, I know the futility of telling someone who’s nervous not to be nervous. Anxiety isn’t mitigated by a barrage of facts about airflow and viral doses. If you feel uncomfortable in the office, your sessions will be less effective. The whole process requires you to feel at ease in the setting and to focus on your thoughts and emotions. “Paging Dr. Hamblin” is for informational purposes only, does not constitute medical advice, and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. By submitting a letter, you are agreeing to let The Atlantic use it—in part or in full—and we may edit it for length and/or clarity. from https://ift.tt/3m0Y9d7 Check out http://natthash.tumblr.com Two weeks ago, I staged a reluctant intervention via Instagram direct message. The subject was a longtime friend, Josh, who had been sharing photos of himself and his fiancé occasionally dining indoors at restaurants since New York City, where we both live, had reopened them in late September. At first, I hadn’t said anything. Preliminary research suggests that when people congregate indoors, an infected person is almost 20 times more likely to transmit the virus than if they were outside. But restaurants are open legally in New York, and I am not the COVID police. Josh and I had chatted several times in the early months of the pandemic about safety, and I felt sure that he was making an informed decision, even if it weren’t the one I’d make. As weeks passed, my confidence began to slip. The number of daily new cases in NYC started to balloon, heightening the risk of transmission in any closed space, but Josh kept going to restaurants. Maybe he was misunderstanding something about the risk. Maybe he’d want to know. The next time he posted about COVID-19, I told him, as gently as I could, that if he was trying to stay safe, it would be a good idea to stop dining indoors. My suspicions were correct. Because the state and city had reopened restaurants, Josh, who asked to be identified only by his first name to protect his privacy, assumed that local health officials had figured out a patchwork of precautions that would make indoor dining safe. He and his fiancé had even gone one extra step, making a Google Map of places they knew were being particularly strict with temperature checks. They were listening to the people they were told to listen to—New York Governor Andrew Cuomo recently released a book about how to control the pandemic—and following all the rules. Josh was irritated, but not because of me. If indoor dining couldn’t be made safe, he wondered, why were people being encouraged to do it? Why were temperature checks being required if they actually weren’t useful? Why make rules that don’t keep people safe? Across America, this type of honest confusion abounds. While a misinformation-gorged segment of the population rejects the expert consensus on virus safety outright, so many other people, like Josh, are trying to do everything right, but run afoul of science without realizing it. Often, safety protocols, of all things, are what’s misleading them. In the country’s new devastating wave of infections, a perilous gap exists between the realities of transmission and the rules implemented to prevent it. “When health authorities present one rule after another without clear, science-based substantiation, their advice ends up seeming arbitrary and capricious,” the science journalist Roxanne Khamsi recently wrote in Wired. “That erodes public trust and makes it harder to implement rules that do make sense.” Experts know what has to be done to keep people safe, but confusing policies and tangled messages from some of the country’s most celebrated local leaders are setting people up to die. Since my conversation with Josh, the internal logic of New York’s coronavirus protocols has deteriorated further. As more and more New Yorkers have become sick, officials have urged people to skip Thanksgiving, because of the danger of eating indoors with people you don’t live with. Rather than closing indoor dining, however, Cuomo has ordered all restaurants and bars simply to close by 10 p.m. This curfew also applies to gyms, which are not exactly hotbeds of late-night activity even in normal times. Meanwhile, case counts have risen enough to trigger the closure of New York City public schools, but businesses still have full discretion to require employees to come into work. (Cuomo’s office did not respond to a request for comment.) [Read: Answers to every possible pandemic-Thanksgiving question] It isn’t just New York; in states across the country, local officials have urged caution and fastidiousness. But those words can seem tenuously connected, at best, to the types of safety measures they’ve put in place. In Rhode Island, for example, residents are prohibited from gathering with even one person outside their household, even in the open air of a public park. But inside a restaurant? Well, 25 people is fine. Hire a caterer? You’re legally cleared to have up to 75 outdoors. The governor’s executive order merely notes: “The lower attendance at such events, the lower the risk.” (The Rhode Island governor’s office did not respond to a request for comment.) Before you can dig into how cities and states are handling their coronavirus response, you have to deal with the elephant in the hospital room: Almost all of this would be simpler if the Trump administration and its allies had, at any point since January, behaved responsibly. Early federal financial-aid programs could have been renewed and expanded as the pandemic worsened. Centrally coordinated testing and contact-tracing strategies could have been implemented. Reliable, data-based federal guidelines for what kinds of local restrictions to implement and when could have been developed. The country could have had a national mask mandate. Donald Trump and his congressional allies could have governed instead of spending most of the year urging people to violate emergency orders and “liberate” their states from basic safety protocols. But that’s not the country Americans live in. Responding to this national disaster has been left to governors, mayors, and city councils, basically since day one. “You've got a lot of problems if every state has to develop everything from scratch,” Tara Kirk Sell, a researcher at the Johns Hopkins Center for Health Security, told me. “First of all, it’s a lot of wasted time and money.” Instead of centralizing the development of infrastructure and methods to deal with the pandemic, states with significantly different financial resources and political climates have all built their own information environments and have total freedom to interpret their data as they please. In the worst-case scenarios, that interpretation has privileged politics over the health of the population. Vociferously Trump-allied governors in hard-hit states such as Georgia, Florida, and South Dakota have declined to so much as implement a public mask mandate while local caseloads have soared. Sometimes, they have sparred with municipal leaders trying to do more. In hard-hit El Paso, Texas, for example, a local stay-at-home order was recently overturned by a state court, even as local officials have had to call in refrigerated trucks to serve as makeshift morgues. [Read: Georgia’s experiment in human sacrifice] Even in cities and states that have had some success controlling the pandemic, a discrepancy between rules and reality has become its own kind of problem. When places including New York, California, and Massachusetts first faced surging outbreaks, they implemented stringent safety restrictions—shelter-in-place orders, mask mandates, indoor-dining and bar closures. The strategy worked: Transmission decreased, and businesses reopened. But as people ventured out and cases began to rise again, many of those same local governments have warned residents of the need to hunker down and avoid holiday gatherings, yet haven’t reinstated the safety mandates that saved lives six months ago. The pandemic is surging virtually everywhere in America; last week alone, it infected more than 1 million people and killed more than 8,000. And yet indoor dining largely remains open, even as leaders warn of the very real perils of Thanksgiving dinner. As time goes by, you'd think that local governments would get better at setting restrictions fine-tuned to protect people’s safety, not worse. But beneath this contradiction lies a fundamental conflict that state and local leaders have been forced to navigate for the better part of a year. Amid the pandemic, the people they govern would generally be better served if they got to stay home, stay safe, and not worry about their bills. To govern, though, leaders also need to placate the other centers of power in American communities: local business associations, real-estate developers, and industry interest groups. These groups, whose businesses have cratered, have been vocal about their desire to see people go back to their jobs and pay their rent on time and in full. Just as these kinds of groups have developed an outsize influence on how policies are made on a national level, they also have significant sway in state and local politics. The best way to resolve this conflict would probably be to bail out workers and business owners. But to do that at a state level, governors need cash on hand; currently, most of them don’t have much. The federal government, which could help states in numerous ways, has done little to fill state coffers, and has let many of its most effective direct-aid programs expire without renewal. Those programs, such as expanded unemployment benefits and lump-sum relief checks, were so successful that they briefly prevented the poverty rate from rising at a time when more people than ever were suddenly out of work. However effective these kinds of robust monetary programs may be at keeping people fed, housed, and safe, they are generally not in line with the larger project of the American political establishment, which favors bolstering “job creators” instead of directly helping those who might end up working those jobs. If you make people safe and comfortable at home, it might be harder to make them risk their lives for minimum wage at McDonald’s during a pandemic. [Annie Lowrey: States need federal money to do the right thing.] With people out of work and small businesses set up to fail en masse, America has landed on its current contradiction: Tell people it’s safe to return to bars and restaurants and spend money inside while following some often useless restrictions, but also tell them it’s unsafe to gather in their home, where nothing is for sale. It’s a woefully inadequate stimulus plan, funded by money extracted little by little from the pockets of people who are mostly just confused about what they’re being compelled to do. Service workers—the people at highest risk of contracting the virus in restaurants, bars, and gyms—are rarely part of a union, which would make it easier for them to take collective action to protect themselves. If they were, their situations might be closer to that of teachers in some cities, whose unions have won them strict protections, including the cancellation of in-person classes once local caseloads rise past predetermined rates. Transparency, Kirk Sell told me, would go a long way toward helping people evaluate new restrictions and the quality and intentions of their local leadership. “People aren’t sheep,” she said. “People act rationally with the facts that they have, but you have to provide an understanding of why these decisions are being made, and what kind of factors are being considered.” With that in mind, I asked Kirk Sell the question that’s been bothering me since I broke the news to my friend about the ineffectiveness of temperature checks and indoor partitions. Why can’t a governor or mayor just be honest? There’s no help coming from the Trump administration, the local coffers are bare, and as a result, concessions are being made to business owners who want workers in restaurants and employees in offices in order to white-knuckle it for as long as possible and with as many jobs intact as possible, even if hospitals start to fill up again. Saying so wouldn’t change the truth, but it would better equip people to evaluate their own safety in their daily life, and make better choices because of it. Kirk Sell stopped me short. “Do you think it might be the end of their career, though?” she asked. “Probably.” from https://ift.tt/3fA8evd Check out http://natthash.tumblr.com Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. Most years, in the anxious days before Thanksgiving, I write a health-related FAQ. It’s meant to be fun, reminding us of the timeless risks that spike every year around this day, such as Salmonella poisoning and fires from exploding turkeys. This year is different. On Thursday, the CDC advised Americans not to congregate with people outside their immediate household. If anything, the advisory understated the risk at hand, saying that “travel may increase your chance of getting and spreading COVID-19.” Travel does increase your risk. It should have read: Do not travel. Do not gather. Effectively, Thanksgiving is canceled. Just wait one year, and then have a basically normal holiday. If everyone in the United States did this, we’d likely save thousands of lives. Many people have changed or pared down their holiday plans, but many others have purchased tickets, their hearts and minds made up. At this point, since millions of people are likely to attempt some form of intermediate-risk Thanksgiving, we should consider a harm-reduction approach. Just as sex-education classes for teens are not meant to encourage those activities, this FAQ is not an endorsement of Thanksgiving gatherings. It is only an attempt to respond to reality. If you’re going to travel to see family, how should you rank the modes of transport? Purely from the standpoint of coronavirus transmission (not carbon emissions, cost, time, or other safety concerns), here’s a very rough hierarchy from safest to riskiest:
Does the risk of air travel change during Thanksgiving if tons of people fly? Yes. Up until now, flying itself has proved to be low risk: The ventilation is good, and people wear masks and are mostly quiet. Airports with large crowds are likely more hazardous than time spent on the plane, and that risk will increase as more people travel. Still, the act of flying in a plane is less of an issue than close, prolonged contact in a home where people are eating and socializing. Traveling vigilantly, only to arrive at someone’s home and act as though there is no pandemic is a serious misallocation of anxiety. I’m not feeling well, but I think it’s just a cold, because I tested negative for the virus. Should I go to an outdoor gathering? No. A negative test isn’t enough to reassure you that you don’t have the virus, especially if you have symptoms. The most common coronavirus test, a PCR test, can confirm only that you do have the virus, but it can’t ensure that you definitely don’t. If you’re not feeling sick, is it morally defensible to get a coronavirus test in order to see family, given testing shortages? In many cases, no. Sick people need those tests, and so do essential workers. They don’t need to be waiting in a three-hour-long line between shifts to get tested. That said, there are situations in which people may have an urgent need to see one another this winter. The most obvious example is when someone is terminally ill or unable to care for themselves, or they are especially isolated and depressed. If you’re fortunate to not fall in any of those categories, and seeing family can wait until the spring or summer, do that. Leave the tests for those who need them. Should my family do temperature checks at the door? No. This is an even less effective mode of screening than PCR tests. By the time a fever develops—if it does at all—you’ve likely been contagious for days. So temperature checks give a false sense of security. The fact that someone doesn’t have a fever isn’t meaningful information that should change how they behave, or how anyone else behaves around them. How much safer is an outdoor meal than an indoor meal? Much, much safer. Almost all transmission of this virus happens indoors. Even if people are close together? Eating outdoors doesn’t mean you’re invincible. Still try to stay six feet apart. If you huddle together around a cramped table and have close, face-to-face conversations with the people next to you, you could absolutely infect them. What if Uncle Al won’t pull his mask up over his nose? If you insist on having a family gathering, at least make clear ground rules. Ask everyone to agree to them beforehand, and to help correct people who seem to be forgetting. Even if Uncle Al believes some bizarre chain email he read about how masks are communist propaganda, he agreed to the rules for the day. Once he has made the choice to attend, he has made the choice to wear a mask, and to wear it properly. If he doesn’t go along with the rules, the whole group should ask him to leave. Why is everyone freaking out? I’ve gotten together with my family several times since the start of the pandemic and no one has gotten sick. Most cases of COVID-19 are mild. I think that’s exactly the challenge. Warning people about this virus isn’t like warning them not to touch a hot stove. In that case, the outcome is predictable every single time. With COVID-19, a Thanksgiving dinner may leave everyone unscathed—or it may lead to serious illness and death for multiple people around the table, and countless more who contract the virus from them. But, taken together, it’s practically inevitable that lots of individual “it’s probably fine” choices accumulate into one enormous, very bad decision. Anthony Fauci said this weekend that we all need to do a “risk-benefit assessment” before traveling. I think the benefit of Thanksgiving is so great that I’m willing to take the risk. Assessing the risk of any single gathering is impossible. Even if you’re ready to die, and you’d sooner die than do a virtual Thanksgiving, you could infect other people and set off a chain of infections. Any assessment of personal risk that you’re willing to take would have to factor in how much harm you’re willing to cause. My 95-year-old mother is staying with my sister in Vermont, and my wife and I were planning to drive and see them for Thanksgiving. Both my wife and I have had very little contact with other people. We practice social distancing, and dinner will be no different. Can this be done safely? Nothing is perfectly safe. But your number of merged bubbles is only two, and they are small bubbles. And the fact that your mother is 95 is significant. If it’s very important for her to see you on the holiday, and she understands her particularly high risk, the time with her may be justifiable. If you all decide to do this, remember that just as you’ve been careful before this dinner, your family should be equally or more vigilant for two weeks after. I’m alone this Thanksgiving. What should I do? Lots of people are alone for Thanksgiving every year. Fortunately, this year has produced tons of guides for cooking for one. There are also new ways to interact with family and friends that didn’t exist in the past. Suddenly, eating in front of your computer has gone from sad to virtuous, and potentially even fun. Since coronavirus cases are rising in some places more than others, should people evaluate their Thanksgiving risk differently depending on where they live? Technically, risk increases as the disease becomes more ubiquitous. That is, a 20-person gathering in a part of the world with little or no virus, such as New Zealand, is very unlikely to lead to infections. The same 20-person gathering in the U.S. is more likely to lead to infections. And at a practical level, though, no part is free of the virus to a degree that should allow people to gather outside their bubbles without extreme precautions. Because some hospitals are overloaded, should we stop doing things that are unrelated to the pandemic? Like shoveling snow? Speeding? Opening a champagne bottle with a sword? The sword openings are fine. But never speed. Keep a regular exercise routine to lower the chance of having a heart attack when you shovel snow. This winter is going to be a bad one to find yourself in a hospital. If you’re seriously injured, you’ll likely get medical care that’s similar to what you would receive in another year. But minor injuries and mild symptoms of conditions such as heart disease will be triaged, delayed, and missed. The health effects will play out in years to come. Those who do get treated in a hospital will add to the strain on an already overwhelmed health-care system. About one in five American hospitals is already short on staff, and hospitalizations continue to rise. There are some regional variations to this answer, but overall this is not a good time to need elective care. Be especially careful. I feel restless. I can’t just sit at home and do nothing. I’m worried about everyone having Thanksgiving. I’m not a medical professional, but I want to help. The U.S. is seeing a surge in food insecurity. If you can volunteer any time, money, or nonperishable foods, now is a great time to do that. You don’t need a medical degree to help address the effects of the pandemic. A sense of purpose can go a long way to staving off the darkness of winter in any year, but especially this one. If I put a frozen turkey into a deep fryer this year, will it still explode? Yes, thaw your turkey. Dropping a frozen turkey into boiling grease will send flames 20 feet into the air. Yet people do it every year. There are some truths about humanity that even a pandemic cannot change. from https://ift.tt/3703lrj Check out http://natthash.tumblr.com Inside the headquarters of the Department of Commerce in downtown Washington, D.C., just around the corner from the White House, sits an expansive suite of offices reserved for the American government-in-waiting. The space, managed by the General Services Administration, can accommodate more than 500 people, and in the weeks before a new president is inaugurated, it would ordinarily be a whirl of activity—hosting dozens of daily policy briefings, outreach meetings, and job interviews for the 4,000 positions that come open in the federal government every four or eight years. Today, however, that transition office sits nearly empty; just a handful of people from the incoming Biden administration have even stepped inside. That the offices have gone unused is not, as one might assume, a consequence of President Donald Trump’s refusal to concede his election defeat to President-elect Joe Biden, or of his directive that his administration not cooperate with Biden’s transition team. The Biden campaign, under federal law, has had access to the transition space since September. But the former vice president has chosen not to use it—a decision made in deference to the coronavirus pandemic and his commitment to prioritizing the safety of his staff during a public-health crisis. Biden won the presidency with a largely virtual campaign, forgoing most in-person canvassing and traditional rallies. But building a new administration in the span of 11 weeks is a far taller order. Imagine a start-up company that must hire 4,000 people, including 1,200 who must be shepherded through the gantlet of Senate confirmation. It’s a project that, even in normal times, no modern presidential transition team has come close to finishing by Inauguration Day. By former President Barack Obama’s 200th day in office in 2009, he had filled just over one-quarter of those positions—and his transition to the White House is widely considered to be the smoothest transfer of power from one administration to the next in decades. [Read: ‘The most important takeover of any organization in history’] Four years ago, Obama symbolically launched his own transition out of office by welcoming Trump to the White House days after the Republican’s surprising election win. The two men spoke for an hour and a half—much longer than planned—before sitting awkwardly for a photo op with reporters. The outgoing president pledged his full cooperation with Trump’s team, but his assistance did not prevent a much bumpier beginning for the new president, who had thrown out the carefully written plans his own transition team had prepared before the election. No such meeting has taken place between Trump and Biden this year, and one isn’t likely anytime soon. Biden’s team will have to contend with not only an uncooperative outgoing administration but an ongoing economic and public-health crisis that is complicating an already Herculean challenge. The thought that the Biden team will be tackling the bulk of that endeavor on Zoom is unthinkable to Obama-administration veterans such as Patrick Gaspard, who helped lead that transition’s hiring efforts before joining the White House staff. A dozen years ago, Gaspard arrived in Washington the day after Obama’s election victory to begin staffing his government at the Commerce Department’s headquarters. “There were constant streams of people coming in, both for interviews but also for briefings, for prep sessions, to give advice and counsel,” recalled Gaspard, who would go on to lead Obama’s Office of Political Affairs before serving as the ambassador to South Africa. “It was a constant hive of incessant activity.” When I asked him to contemplate managing a presidential transition during a pandemic, he just laughed. “There are extraordinarily brilliant folks who are leading all of this, but man, I can’t imagine it,” Gaspard told me. “I just can’t.” The Biden team does have certain advantages that the Obama transition lacked. In 2008, Democrats had been out of power for eight years, and the president-elect had served in Washington for less than four. Biden, by contrast, has been out of office for just four years and brings nearly half a century in government experience to the White House. The man he’s chosen to lead the transition, former Senator Ted Kaufman of Delaware, is a co-author of the federal law governing the modern transition process. “This is a team that is filled with people who understand government, who have been there before,” said Max Stier, the CEO of the nonpartisan Partnership for Public Service, who has advised transition teams of both parties over the years, including Biden’s. Led by Kaufman, the Biden transition began working behind the scenes months before the election. “It's a very challenging thing to do this right, but they’ve started better than anybody so far,” Stier told me. The pandemic, of course, isn’t new by now, and the Biden campaign, like businesses across the country, is used to interviewing job applicants remotely. Many of the people who will likely form the White House staff, for example, have already been working together remotely for months. (The transition team uses Google software for video meetings, rather than Zoom.) And in some cases, incoming members of the Biden administration might be able to start their jobs virtually too. The increase in telework throughout the government this year meant that many new employees took their oaths and completed their onboarding paperwork remotely. But many jobs are too important to fill without an in-person meeting. “I would want to sit across the room from the president-elect before I'm going to take a job in his Cabinet,” a person close to the transition told me on the condition of anonymity because Biden’s team is under strict orders not to speak with the media. “So a lot could be done on Zoom, but some can’t.” (The former vice president reportedly conducted his search for a vice-presidential running mate this summer through a mix of in-person and virtual interviews.) Nor can many other aspects of the transition proceed entirely remotely. Transition teams will need to physically enter government buildings to review classified documents at the Pentagon, the Department of Homeland Security, and other federal agencies. Biden officials have set up strict COVID-19 protocols—and says it reviews those requirements every two weeks—for when those teams begin meeting in person with their counterparts in the Trump administration. And the president-elect’s staff has named larger agency review teams than usual to account for the possibility that members could become infected or need to quarantine during the transition. “Like many organizations around the country, the Biden transition team will continue to do our work remotely,” the team said in a statement. “While we have access to GSA space, the number of staff needed inside the office will be limited.” Conducting so much sensitive planning remotely could also raise cybersecurity concerns, especially because the Biden team is not yet using government networks, and commercial platforms such as Zoom were plagued by security issues over the summer. The Biden transition team said it has “invested in best-in-class IT systems and processes,” including briefing staff members on using security keys and other best practices. Beyond the pandemic, the bigger threat to a successful transition, according to the people I interviewed, is the Trump administration’s continued refusal to cooperate with the incoming Biden team. Federal agencies are waiting for the General Services Administration to formally “ascertain” that Biden has won the election, a move that will release millions in federal funds and allow transition landing teams to meet with outgoing Trump administration officials. Biden advisers have warned that the delay could prove deadly during the pandemic, since it will hamper the new administration’s ability to swiftly distribute vaccines that appear poised for federal approval. “As knowledgeable as they are, they're still on the outside,” Stier said. “It’s a real limitation.” The delay has other national-security implications: The FBI cannot begin processing permanent security clearances for incoming Biden officials, which could result in crucial agencies being understaffed in the event of a terrorist attack. It was the 9/11 attacks during the eighth month of President George W. Bush’s first term that helped prompt an overhaul of the presidential-transition process so that new administrations would be better prepared in the future. The combined effects of the delayed transition and the pandemic could be less obvious but felt more widely throughout the new administration. One of the most important but often overlooked aspects of a presidential transition, Stier told me, is the integration of a new administration’s many political appointees into a career federal workforce that must carry out its policies. “They are the engine room of the government. They are ultimately the ones that know the most and get the stuff done,” he said. “There’s been a lot of turmoil, and turmoil is not good for organizational performance.” The fact that many federal employees won’t get to meet their new overseers in person only adds to the challenge. “It's much easier to maintain existing relationships than to create new ones, especially relationships of trust,” Stier said. The Biden team might find some advantages to a pandemic transition. It likely won’t have to devote as much time or money to planning an enormous presidential inauguration, as that will almost certainly be much smaller in scope than usual. And it could choose to preserve or even expand teleworking across the federal government, which has led, in some cases, to higher productivity as employees forgo long commutes to and from work. One former Obama-administration official who no longer lives in the Washington area told me they are eager to see whether they can rejoin the government from afar. Gaspard told me he wasn’t worried about the long-term effects of a remote transition on the workings of government in the Biden administration. But he said a certain “dynamism” would be lost. It’s a missing ingredient undoubtedly familiar to millions of people who haven’t seen their office in months, but one whose absence is only magnified when the task at hand is building a new presidential administration. “There’s an ad-hocracy in a transition,” Gaspard said, chuckling at coining a new word, “that’s not possible in the virtual world.” from https://ift.tt/2J5wx7T Check out http://natthash.tumblr.com The United States has passed a terrible milestone: 250,000 Americans have died of COVID-19. But with the holidays approaching and the spread worse than ever, the situation could become even more dire. Now is the time to have hard conversations about Thanksgiving, even though it will be awkward. On this episode of the Social Distance podcast, James Hamblin and Katherine Wells answer listener questions about the holidays and give advice on how to cancel plans. Listen to their conversation here: Subscribe to Social Distance on Apple Podcasts, Spotify, or another podcast platform to receive new episodes as soon as they’re published. Below is a transcript of listener questions and responses, edited for length and clarity. Katherine Wells: Here’s a general question from a listener: “How do I decide whether I celebrate the holidays with family if everyone in our family is being safe and masking and we live in a lower-risk area, but the holidays are inside? Is it still a giant mistake to celebrate with our family for the holidays? Thanksgiving is my favorite.” James Hamblin: It’s really hard to imagine a gathering inside where people are also masked, because usually Thanksgiving involves eating. If you have a small family and you can do things outside and everyone tries to really quarantine for two weeks before and after this gathering, there are ways that it could be done. But there’s a sort of cultural dynamic, especially when you’re among friends and family, that people let their guard down. So I think it would be safest—unless you really know your whole family to be really vigilant about this ... Wells: This is the thing ... there is a wide variation in how people interpret “being safe and masking.” Everyone may say they’re being safe and masking, because they’re being more safe and wearing masks more often than they did before the pandemic. But it doesn’t mean they’re 100 percent careful. So the answer to the question is yes, it is a big, giant mistake, right? Hamblin: Yeah. Because traveling, bringing people together as multigenerational families, gatherings like this ... remember there was this wedding in Maine over the summer that they’ve traced to seven deaths now among people who weren’t even at the wedding. And so even if everyone in your family were ready to become seriously ill and possibly die, it’s not just about you. So yeah, just don’t do it. But the hard thing is talking to your family about that—friends, family, whoever you might spend Thanksgiving with. Wells: Here’s another question about that: “How do I convince my parents, who have been living very carefully to avoid the virus, that they shouldn’t travel home for Christmas to stay with the rest of my extended family? I understand it’s tough and sad to miss a family holiday, but my extended family has not been living in a similarly careful way. I’m very nervous.” Hamblin: Yeah, I’m sure that stuff is going to happen. Part of it depends on your families. What is their thinking? If they’ve been in a Fox News bubble and think the whole thing is a hoax, that’s different than if they have made some internal calculation and think they can do it safely. But in any case, a heartfelt conversation where you’re expressing concern for them, and probably a series of conversations. Wells: I tell you, I’ve done it with my parents: “I don’t want you to die!” Almost a quarter of all hospitals in the U.S. right now don’t have enough staffing to deal with all the patients they have right now. This isn’t really a time for gentle, hopeful prodding. Hamblin: I think it’s a time for being evidence-based in your approach. We have a tendency to think the more forceful or emotional or angry we sound, and the more scolding we get, the more effective it’ll be. For some people, it may work. For others, it requires a kind of Socratic path. And I think those are the kinds of conversations that are actually going to turn the tide at this point. My writing and others’ writing are probably pretty futile at this point. I don’t know what more I can do to talk to audiences of national magazines if people haven’t already gotten the picture. But there’s a lot that can be done person-to-person. Wells: What we’re talking about is this in-between where people definitely know it’s a problem, they know what they’re supposed to do, but the strictness is just hard. It’s genuinely hard to keep up. I think a lot of people are just feeling tired right now. We’ve been doing this for six months. Can I just have one single meal with my family? But the answer is you can’t, not the way you did before. Hamblin: Yeah. Don’t do it. Wells: Here's another scenario. This is a tough one. A listener wants to visit her 91-year-old mother. It’s not an emergency, but her cognition is declining. If she quarantines and travels by plane wearing a mask, can she see her mother? Hamblin: This is the one big caveat to Thanksgiving gatherings: people with terminally ill relatives. You might not see them again. Honoring people’s wishes if they want to see you and they don’t care if you infect them, and they are homebound, not seeing other people, that’s a situation where I think the right thing to do is honor their wishes and go see them. If you can do that safely. It doesn’t mean bringing your whole family together to see them simultaneously. But if it’s a one-on-one situation with a family bubble going to see an elderly relative who desperately wants to see them, that’s something that I wouldn’t categorically say we should not do. And that’s what makes it so hard to say simply: Don’t go at all. But that’s a different situation than just having Thanksgiving in May. Postpone it and do it outside. Everything will be pretty similar then, except we can actually enjoy it. Wells: Okay, we’ve also gotten some plane questions. If you’re going to break this recommendation because you have some extenuating circumstances and [have to] travel, how are people supposed to think about travel by plane versus car versus train? Hamblin: Planes are not what I’m worried about. We are not seeing significant transmission on planes. Planes have good ventilation. They have good airflow and filters. People mostly wear masks. You pretty much kind of sit quietly not facing other people. You’re not having loud, boisterous conversations and you’re not eating. That’s a much safer scenario than a prolonged period of having a loud conversation, eating with a big group. It’s really about once you arrive. Wells: So it’s not getting to Thanksgiving that is the riskiest, necessarily; it’s Thanksgiving? Hamblin: Yeah, that’s the unfortunate thing. On other forms of travel: riding in a car with strangers is not a good situation. Taking a ride-share or a taxi to an airport is not a good situation. Wells: A car alone or with people in your household, not a problem. Train: bad? Hamblin: I don’t know how they’re doing trains right now, but I believe trains have ventilation systems that are similar to subways and planes and are generally pretty safe. And once again, most people on the train are sitting quietly, keeping to themselves. Wells: But again, don’t do it. Hamblin: People will have a need to travel occasionally, so we’re just being pragmatic, but yeah, elective travel right now is not a good idea. This is the worst of the pandemic. Wells: So to reiterate, don’t go to Thanksgiving. Just don’t do it. Okay, one last question; this one is from Kevin Townsend, producer of the show. Kevin Townsend: My family is spread all across the country and every holiday season is a negotiation of who’s going where when. Canceling Thanksgiving probably means shifting around Christmas. I have to call my dad right after taping. Am I canceling Christmas, too? Hamblin: Oh gosh. You know, if people have Thanksgiving in traditional ways on anywhere near the scale that Americans normally do, it’s going to be a nightmare around Christmas. Any hope of gathering at that point will be in doubt. There will be serious travel advisories; many cities will have extreme lockdowns. We’re going to be in a much worse shape. There’s that three- or four-week lag between spreader events like Thanksgiving and when you actually see the big uptick in hospitalizations. We’d be seeing it right around Christmas. So without regard to any particular religious holiday, which is going to be especially fraught, any negotiation about how to handle the December holidays is going to be much worse if we are overloaded from people having gotten together on Thanksgiving. Wells: So what’s Kevin supposed to say to his dad? I think the breakup “It’s not you; it’s me” tactic works well. I’m just not ready to have a Thanksgiving ... I’m not in a place where I can really have a Thanksgiving right now. Hamblin: If you really feel like you can’t have an honest conversation with someone, then do that. But if you see an opportunity to actually talk directly about the concerns about the virus, you can at least make other people question if it’s really smart to be getting the family together. Wells: Yeah, if you feel uncomfortable with it, don’t push through it and go. And not just for you but for everyone, because hospitals are already overwhelmed in so many places. You don’t know if you’re even going to be able to get care in the hospitals in a couple of weeks. Hamblin: It’s honestly a great opportunity to just take the holiday off, too. Just go with an excuse. I have to work. I need to save money. I’m not feeling well. Those are going to be ways to avoid it if you know that you have family members who just really couldn’t honestly talk to you. Townsend: The dog ate my plane tickets. Wells: Exactly. This is genuinely very difficult. I hope we’ve given a range of options for how to say no, but the answer is no. And I think the vaccine news is, at least for me, making this a little bit easier, because we’re not going to be locked down forever. There is an end in sight. It’s not going to be immediate, but there is an end in sight. So all the more reason to really tighten up right now. from https://ift.tt/2UNwBvY Check out http://natthash.tumblr.com Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. Updated at 11:51 a.m. ET on November 20, 2020. Understanding the pandemic this week requires grasping two thoughts at once. First, the United States has never been closer to defeating the pandemic. Second, some of the country’s most agonizing days still lie ahead. Long term, the view has never looked brighter. This week, confirmation came that scientists have developed two vaccines against the coronavirus, each at least 90 percent effective, and more shots are likely on the way. Some health-care workers could be vaccinated by New Year’s. Most Americans can expect to receive a shot in the spring, according to Anthony Fauci, the country’s top infectious-disease expert. Yet in the short term, the outlook is unavoidable: The country faces several weeks of mass suffering and death. Almost every major metric of the pandemic stands at or near record levels, according to data collected by the COVID Tracking Project at The Atlantic. 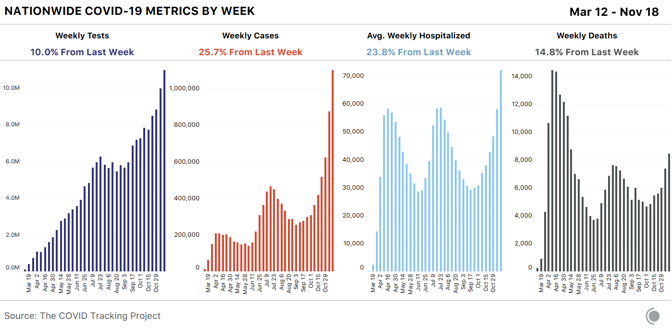
More Americans are getting sick: The U.S. has recorded more than 1 million cases of COVID-19 in the past seven days, the highest level ever. More Americans are in need of urgent medical care: Nearly 80,000 Americans are in the hospital with COVID-19 right now, smashing the old record of 59,924. And more Americans are dying: At least 8,461 people have died of COVID-19 since last Thursday, the highest seven-day total since May. More older Americans, and residents of nursing homes, are also getting sick. This week, nursing homes and similar facilities reported 29,606 new virus cases among residents and staff, the largest increase in six months. This surge is especially foreboding because the virus is deadliest in these places; about 40 percent of all U.S. coronavirus deaths have happened in long-term-care facilities. For weeks, White House officials have argued that the virus should be allowed to spread freely as long as nursing-home residents are protected. The new data make clear that this approach is failing. The virus continues to hammer every region of the country. Fifteen states hit all-time records for new cases this week. Five of those record-breaking states are in the Northeast; no state in that region had set a new case record since May 31. In short, the United States is plunging into what may be the darkest period of the pandemic so far, even as it lacks the public-health orders or congressional assistance that buffered it in the spring. Because the virus is so widespread, America’s medical system is facing a greater test now than it did then; one in five hospitals nationwide reported a staffing shortage this week, according to federal data. A vaccine is at hand. But for tens of thousands of Americans, it will come too late. Here are five big lessons from the data we collected this week at the COVID Tracking Project. First: Cases are increasing exponentially nationwide, and it may be months before they fall in some states. For the past few weeks, outbreaks have been worsening rapidly in more densely populated midwestern states like Illinois and Michigan. At the same time, cases have been steadily rising in every region of the country. Nationally, the seven-day average for daily reported cases has almost doubled since November 1. But what does it mean to see the country report 1 million cases in a single week? Leaving aside that this number accounts only for detected cases—true infections are almost certainly higher—we know this wave of newly diagnosed cases will crash into hospital systems that are, in many areas, already over capacity. And we know that three or four weeks behind each jump in cases, we expect to see a spike in reported deaths. Ominously, this effect might be hitting multiple regions at once. Cases in the South have grown closer to that region’s summer peak, while the Midwest continues to post enormous increases and the West and Northeast creep upward. 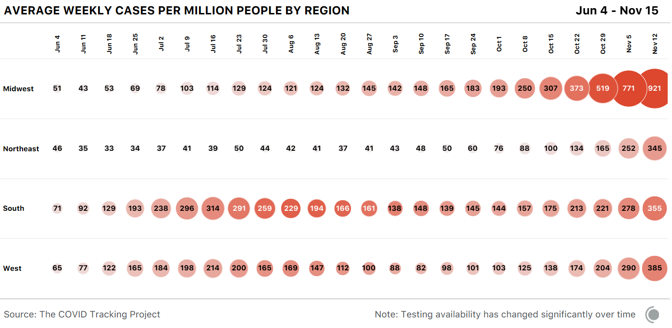
This increase in cases can’t be chalked up to testing. While our national expansion in testing has seen the number of tests rise linearly, cases are now growing exponentially. In fact, the testing infrastructure may be coming under strain again, as it did during earlier outbreaks. News organizations are once again reporting long lines at drive-through COVID-19 testing sites, and Quest Diagnostics, which makes both PCR and antigen tests, this week said high demand and limited supplies are delaying the delivery of some results. Data reporting, too, is increasingly difficult as case numbers soar, case investigations and contact tracing even more so. And at the moment, we don’t see any indications that cases have reached a peak nationwide. Nationally, cases have already been rising for 10 weeks. Yet based on what we’re seeing in the data, the outbreaks in many states, even in the hard-hit Midwest, may have plenty of room to grow. Look to North Dakota, for instance, where cases started taking off almost exactly three months ago. (For our purposes, we define the beginning of a surge as the moment when a state sees an average of more than 200 new cases a day per million residents.) North Dakota passed that line and began to surge on August 18. But another 67 days elapsed before every other state in the Midwest had followed it. As of today, North Dakota is a canary in the coal mine for our current outbreak: It has reported more new cases per capita than any other state or territory for nine of the past 11 weeks. But it’s not clear that North Dakota’s outbreak has even peaked yet. Some states in the region have taken more aggressive public-health measures than North Dakota, and they may see declines soon. But among those that have adopted a similar approach to the virus as North Dakota, we could be looking at many more weeks of rising cases. 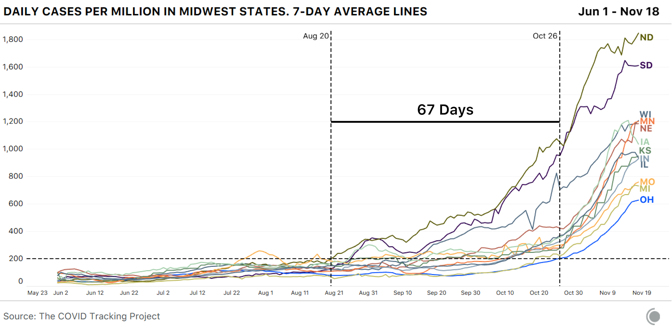
A similar story is unfolding across the country. Only three states have kept their average case totals below that “surge” threshold of 200 daily new cases per million residents. Yet many states just crossed that threshold and are steadily rising now. If those states follow the same path as the Midwest, they could more than triple their case counts in the coming weeks. 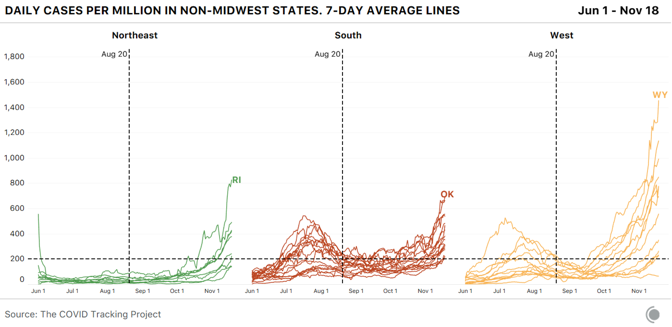
Where race and ethnicity data are available, we are seeing cases rise most quickly for Indigenous and white populations in many states. Not all states report data for Indigenous people; of those that do, 18 now report more than 1.5 times the number of cases reported a month ago. In eight states, the number of reported cases for white people has more than doubled over the same time, while cases have grown more slowly in other racial and ethnic groups. Second: Hospitalizations are also smashing records nationwide, and the national medical system is under the greatest strain it’s faced in the pandemic so far. As we have written many times before, it’s clear that increases in COVID-19 cases mean more reported hospitalizations about 12 days later, and more reported deaths within a few weeks. In human terms, some of the people being diagnosed now will end up sick enough to be admitted to a hospital. Some of those people—though far fewer than in the spring—will die. The gains we’ve made since the spring in keeping people alive with severe cases of COVID-19 are at risk if our hospital systems are overtaxed. And our hospital systems are already overtaxed, even before the huge case spikes we saw this week and last week have converted into rising hospitalizations. This week states reported a 21 percent increase in the number of patients hospitalized with COVID-19; that figure has risen 67 percent since November 1. The number of people hospitalized per capita in the Midwest has hit a level not seen since the spring surge in the Northeast. 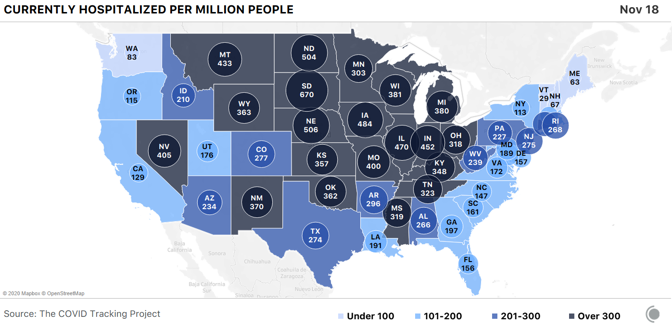
Our colleague, Alexis C. Madrigal, wrote at The Atlantic this week about the dire straits facing American hospitals; 22 percent of facilities told the U.S. Department of Health and Human Services they expect staffing shortages. The examples are everywhere: More than 900 staff at the Mayo Clinic in Minnesota and Wisconsin have been diagnosed with COVID-19 in the past two weeks; El Paso’s convention center has been converted to a field hospital, and some hospital patients are being sent as far as Austin, nearly 600 miles away, for treatment. [Read: Hospitals can’t go on like this] Using the data we compile from state and territorial health departments, we have been able to track total current COVID-19 hospitalizations, but not newly admitted COVID-19 patients—a more precise measure of where outbreaks are worsening. A newly released dataset from the Department of Health and Human Services allows us to look at daily COVID-19 admissions of new patients, and they are rising sharply in every U.S. region. 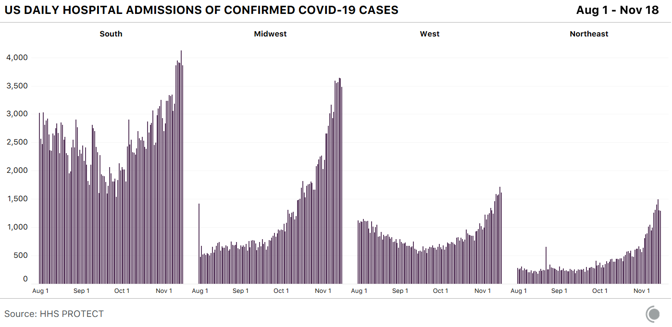
A per-capita view of hospital admissions data also allows us to pinpoint states both inside and outside the Midwest that are seeing spikes in new hospitalizations. It’s clear that Wisconsin is still in serious trouble and that Montana’s new admissions are rising sharply, while South Dakota’s may have peaked. Iowa, Kentucky, and Oklahoma are all showing the signs of dangerous increases in new patient admissions as well. 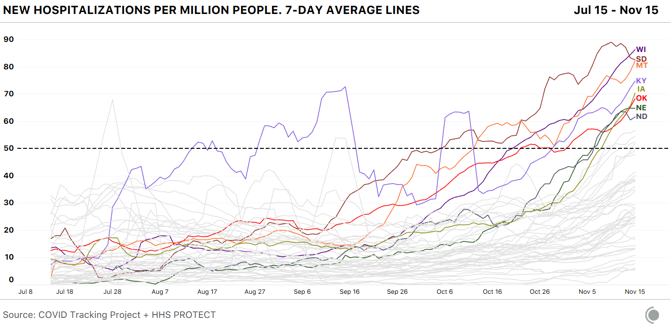
Third: Deaths may soon exceed their levels from the spring. States reported more deaths from COVID-19 this week than we’ve seen since May. Yesterday, The New York Times reported that the COVID-19 pandemic has claimed 250,000 lives. As we wrote the last time a similar record loomed, our current figures run behind those of several other sources because we compile data at the state level, rather than from counties or cities. As of November 18, the COVID Tracking Project recorded 241,704 fatalities from COVID-19. 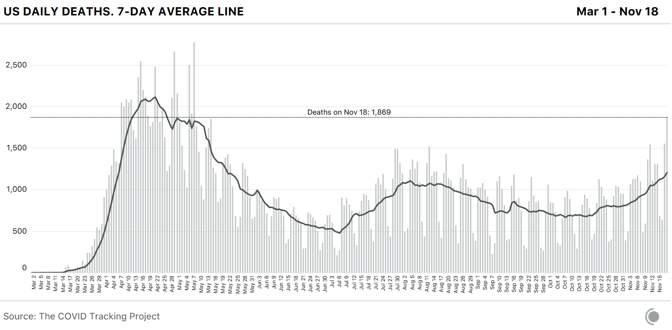
Our understanding of who is dying is hampered by states not reporting demographic categories consistently. Reported deaths for white people are still proportionately lower than for most other demographic groups, but the trend is shifting. In many states, deaths are rising most quickly among white residents. Six states are reporting more than 1.5 times the deaths among white residents as in mid-October, while deaths have generally risen more slowly in other racial and ethnic groups. [Read: How many Americans are about to die?] Fourth: The virus has continued to ravage long-term-care facilities. As our long-term-care update detailed earlier this week, nursing homes and other congregate care facilities reported their largest increase in cases in the past six months—29,606 cases. New COVID-19 cases in nursing homes, assisted-living facilities, and other long-term-care facilities rose 20 percent across the nation. 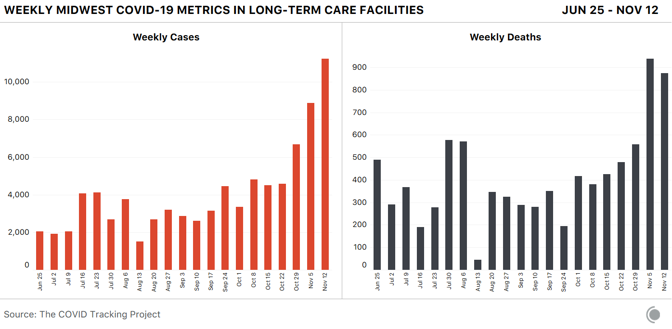
From the 37 states that report residents and staff separately, we know that residents account for twice as many cases as staff. Yet, from the same batch of states, we know that less than 1 percent of deaths in long-term-care facilities occur among staff. There are still 13 states that don’t split resident and staff cases and deaths, obscuring any additional analysis. After three weeks without releasing cumulative long-term-care case data, North Dakota’s health department sent us a spreadsheet on November 17 that shows substantial increases in cases. Resident cases have increased by 70 percent and staff cases by 61 percent since October 29. With a three-week gap in the data, we are unable to determine at what rate cases are increasing.* Finally, the country’s public-health response remains scattered and patchwork. But some Republican leaders have urged mask use in recent days. Facing rising cases and hospitalizations, many states and metropolitan areas recently mandated new or more stringent measures in an effort to contain the virus. California Governor Gavin Newsom said he was pulling an “emergency brake” for the state, eliminating indoor dining, closing indoor gyms, and banning indoor worship services in 41 counties, among other efforts. Iowa, a state whose governor had long resisted a mask mandate, announced it would require residents to wear masks. Minnesota’s governor banned indoor dining and in-person get-togethers until mid-December. New York City this week said it would shut down schools as cases have risen. Governor Mike DeWine of Ohio, who was one of seven Democratic and Republican governors to co-author an opinion piece in The Washington Post this week urging Americans to cancel Thanksgiving, advised residents to wear masks and instituted a curfew. Costco, one of the nation’s largest retailers, said customers would be required to wear a mask while inside its stores, regardless of local and state regulations. This week, West Virginia Governor Jim Justice tightened the state’s mask mandate and held an 80-minute press conference in which he implored West Virginians to get on board. “I love all of our kids, and I want them to be able to play ball and go to school, but more than anything I want us to get more control over this terrible virus that’s just eating us alive,” said Justice, a Republican. “I want us to absolutely wear a mask. I will not allow people to just decide they’re not going to wear a mask. I mean, what right do they have to infect others or possibly infect others? … Ninety-six percent of the people in West Virginia believe we ought to be wearing masks. I strongly urge—strongly urge—us all to wear a mask. That’s all we’ve got to go on right now.” Artis Curiskis, Alice Goldfarb, Erin Kissane, Jessica Malaty Rivera, Kara Oehler, Joanna Pearlstein, and Peter Walker contributed to this analysis. *This article originally reported that in West Virginia, cases related to long-term care facilities more than doubled over the past two weeks, with deaths increasing at nearly the same rate. In fact, COVID Tracking Project researchers misinterpreted the state’s newly reformatted long-term care data. In the past two weeks, within long-term care facilities in the state, resident cases actually increased by 9 percent, staff cases increased by 18 percent, and deaths increased 16 percent. from https://ift.tt/32WSayj Check out http://natthash.tumblr.com |
Authorhttp://natthash.tumblr.com Archives
April 2023
Categories |







 RSS Feed
RSS Feed
