|
The “abortion pill” is a bit of a misnomer. Known formally as medical or medication abortion, it is really two separate drugs—mifepristone, which stops the pregnancy from progressing, followed by misoprostol, which triggers uterus contractions—that together mimic what happens in a miscarriage. And so, in the early days of at-home medication abortion in the 1990s in the U.K. and Sweden, doctors looked to this parallel to establish a cutoff for its use: nine weeks, when a miscarriage is also typically managed safely at home. Over time, however, the line has slowly shifted later into pregnancy. When the U.S. finally approved medication abortion in 2000--much delayed because of political controversy—the FDA allowed only self-managed abortions up to seven weeks and did not extend to 10 weeks until 2016. Since then, though, international consensus has shifted with new data. The World Health Organization now recommends 12 weeks, or the end of the first trimester, as the cutoff for self-managing a medication abortion. “The FDA label is lagging behind what the science says,” Heidi Moseson, a researcher at Ibis Reproductive Health who has studied the issue internationally, told me. And in practice, women are using these pills even later in pregnancy. In countries where abortion is or until recently had been illegal, such as Mexico, Argentina, Ecuador, and Chile, activists have for years helped women self-manage medication abortions in the second trimester up to 24 weeks. Different stages in pregnancy just require different doses of the drugs. The odds of needing to see a doctor—say, because the placenta was not completely expelled—do tick up later in pregnancy. These complications are very treatable because they are treated exactly as doctors would an incomplete miscarriage. Clinically, the two are indistinguishable. But in U.S. states with restrictive abortion laws, women have been prosecuted when seeking follow-up care after ending pregnancies with pills ordered online. Outcomes will get worse if women are too afraid to go to the hospital for complications or if doctors refuse to treat them. At the same time, with more states banning abortion, the pills may be the one remaining option for women determined to end pregnancies. The U.S. is only going to see more self-managed medication abortions, and more later ones in the post-Roe era. To understand what medication abortion looks like in the second trimester, we have to look outside the U.S., to countries where records are kept and data carefully gathered. In Scandinavia, the same two drugs are routinely used for the second trimester abortions in the hospital. One hundred percent of abortions in the second trimester are performed with medication in Sweden, says Kristina Gemzell Danielsson, an ob-gyn at the Karolinska Institute. Historically, she explains, few doctors there were taught to perform second-trimester surgical abortions. Swedish researchers were on the forefront of developing medication abortions, though, and the mifepristone-plus-misoprostol protocol quickly became the default in hospitals once it was codifed. Medication abortion can be used in the second trimester in U.S. hospitals too, but it accounts for only a single-digit percentage of such abortions here. First-trimester medication abortions in Sweden can be managed at home; but second-trimester ones are managed in the hospital because they can take longer, can be more painful, and is more likely to require a surgical procedure to completely empty the uterus. In the second trimester, the fetus and placenta are simply bigger: A fetus at 10 weeks is the size of an olive, at 20 weeks the size of a banana. The placenta almost triples in weight. A small number of cases in the second trimester--less than 1 percent—might involve bleeding heavy enough to require a transfusion. On the whole, medication abortion in the second trimester is “extremely safe” with appropriate care, Gemzell Danielsson told me. It is much safer than techniques women have resorted to in the past, such as using coat hangers and bleach. Moseson, the researcher at Ibis, points out that it’s safer than childbirth. In countries where abortion was illegal, though, women have been self-managing second-trimester medication abortion for a long time, too. Moseson has worked closely with activist groups in Latin America to document outcomes. Due to the sensitivity, “in many cases, we were securely transferred photographs of records,” she told me. In some, they even did physical handoffs. Out of 318 self-managed medication abortions at 13 to 24 weeks in the study, 76 percent were completed without any further medical intervention. For pregnancies before 12 weeks, that proportion is closer to 95 percent. All of the patients in the study who needed care got it without legal repercussions, despite various abortion restrictions in the countries. Overall, 95 percent of patients were able to end their pregnancy as they wanted. (The other 5 percent needed another medication abortion, continued their pregnancies, or did not follow up.) Moseson reiterated that medication abortion is very safe with the right health care. But in the U.S., access to that care is not always a given. Not only is abortion being banned—with laws that punish doctors—but it is in some cases being criminalized, with law enforcement prosecuting women, especially for ending late second- and third-trimester pregnancies. Since 2000, more than 60 women have been prosecuted for self-managed abortions or miscarriage, according to Jill Adams, the executive director of If/When/How, a reproductive-rights group that is studying these cases. The charges have included murder, drug possession, and failure to report an abortion. And it’s not just pregnant women themselves who are at legal risk: In Pennsylvania, a mother went to jail after purchasing online abortion pills for her pregnant teenage daughter. In all the cases Adams could think of so far, the charges were eventually dropped, lessened, or overturned by a judge on appeal. “But by that point, someone’s life may have been upended,” she says. She pointed to the case of Purvi Patel, an Indiana woman sentenced to 20 years for feticide and child neglect after police uncovered text messages to a friend about abortion pills. Her conviction was overturned, but only after she spent three years in prison. Doctors may not be able be able distinguish between a medication abortion and miscarriage based on medical information, but law enforcement can try, casting a wide dragnet for clues about a person’s intent. In 2020, a 15-year-old girl and her mother came into the New York City health center where Miranda Loh, who specializes in adolescent medicine, was then working. The girl had taken abortion pills she bought online to end her 15-week pregnancy five days earlier. Now she was in pain, with an umbilical cord protruding from her vagina. She was one of the patients who needed a surgical abortion to complete her second-trimester medication abortion. The procedure was entirely routine at that hospital, and she went home with antibiotics within 24 hours. Without this care, though, it could have turned into “a serious infection that could absolutely be life-threatening,” Loh told me. “I think the biggest risk and threat that people face now that are seeking self-managed abortion, or abortion of any kind, is criminalization,” she added. In New York and in 2020, the girl and her mother could come to the hospital for care after an incomplete medication abortion. In much of the U.S. now in 2022, women may very well fear that’s no longer legally safe. from https://ift.tt/l4NtaFP Check out http://natthash.tumblr.com
0 Comments
In one sense, this is how it was always supposed to go: When viruses evolve, vaccines should follow, and sometimes try to leap ahead. The COVID-19 shots that the U.S. has used to inoculate hundreds of millions of people are simply so new that they’ve never had to undergo a metamorphosis; up until now, their original-recipe ingredients have stood up to SARS-CoV-2 well enough. But the virus they fight has changed quite radically, and this fall, the vaccines will finally, finally follow suit. Today, an advisory committee to the FDA recommended that our current slate of shots be updated to include a piece of an Omicron subvariant, with the aim of better tailoring the vaccine to the coronavirus variants that could trouble us this fall. Neither the agency nor its outside expert panel has yet reached consensus on which version of Omicron will be the best choice, and whether the next round of shots will still contain the original version of the virus as well. Regardless, a new formulation with any bit of Omicron will constitute a bet that these ingredients will better protect people than another dose of the original vaccine recipe, whose protective powers have been fading for many months. [Read: The U.S. is about to make a big gamble on our next COVID winter] The virus’s own mutational hijinks will determine, in part, how well that wager pays off. But for it to work at all, people have to actually get the shots. “A vaccine without vaccination is an exercise in futility,” says Stephen Thomas, the director of the University of Maryland’s Center for Health Equity. The protective power of COVID shots will depend heavily on their reach: The more people who get them as recommended, the better they’ll work. Here in the U.S., vaccine enthusiasm has a pretty dire prognosis. Fewer than half of the vaccinated Americans eligible for a first booster have opted for one; an even paltrier fraction of those who could get second and third boosters are currently up-to-date on their shots. Among high-income countries, the U.S. ranks embarrassingly low on the immunity scale—for a nation with the funds and means to holster shots in spades, far too many of its residents remain vulnerable to the variants sweeping the globe, and the others that will inevitably come. Those numbers are unlikely to budge in future inoculation rounds, unless “we do something very dramatically different,” says Kevin Schulman, a physician and economist at Stanford University. The next round of vaccines could start its roll out by early October, depending on its contents, making this autumn the first COVID-shot update of the rest of our lives—and marking one of the ways we’ll have to permanently incorporate SARS-CoV-2 into our thinking. The round of shots rolled out this fall, then, won’t just be a sequel to the injections of the past year and a half; it will be a chance for a true cultural reboot. By year’s end, America will likely set a vaccine precedent, either breaking its pattern of injection attrition or further solidifying it, and letting the virus once again lap us. From the beginning, the messaging on COVID boosters has been a bungled mess. Originally, it seemed possible that a duo of doses, perhaps even a single shot, would be enough to block all infections, and bring pandemic precautions to a screeching halt. That, of course, was not the case. With the virus still spreading last summer and fall, experts began heatedly debating what purpose extra doses might serve, and who should get them—and if they were needed at all. Caught in the cross fire, the FDA and CDC issued a series of seemingly contradictory communications about who should be signing up for extra shots and when. [Read: Vaccines are still mostly blocking severe disease] Then BA.1—the original Omicron subvariant—arrived. This variant was so mutated that it was tough to stave off with one or two original-recipe doses alone, and suddenly far more experts agreed that everyone would benefit from an immunity juice-up. By the end of 2021, the U.S. had a catchall booster recommendation for adults (and has since expanded it to kids as young as 5), but whatever the benefit of a booster might be, much of the public had disengaged. Many had been infected by then, and even people who had gladly gotten doses one and two couldn’t muster the same urgency or enthusiasm again. “The feeling was, I’ve already gotten one series of shots—I’m not just going to keep getting more,” especially with no obvious end to the injection rigamarole in sight, says Stacy Wood, a marketing expert at North Carolina State University who, with Schulman, has written about the challenges of promoting COVID-19 vaccines. The shots have also become much harder to get. Mass vaccination sites have closed, especially affecting low-income and rural regions, where there’s a dearth of medical centers and pharmacies. Pandemic funds have dried up, imperiling shot supply. Ever-changing recommendations have also created an impossible-to-navigate matrix of eligibility. Since the booster rollout began, recommendations on when to boost and how many times have shifted so often that many people haven’t realized the shots were actually available to them, or were mistakenly turned away from vaccination sites that couldn’t parse the complex criteria dictating who was allowed an extra dose. Pile onto that the persistent problems that have stymied initial vaccinations—a lack of paid sick leave, fears of side effects, the hassles and costs of scheduling and traveling to a shot—and it sends a message: The shots can’t be so necessary if they’re this cumbersome to get. The country’s loosened stance on the pandemic as of late has reinforced the shots’ optional status. With COVID death rates near their all-time low—thanks largely to vaccines—infections, which have now hit a majority of Americans, continue to be dismissed as manageably “mild.” Mask mandates, testing programs, and gathering restrictions have evaporated. And so have what vaccination requirements existed. [Read: America created its own booster problems] “People just aren’t as concerned,” says Mysheika Roberts, the health commissioner of Columbus, Ohio. “The fear of the virus has changed a lot.” Of the 230,000 vaccines Roberts’s team has delivered to her community since December 2020, only 16,000 have been boosters. In an atmosphere of mass relaxation, the urgency of more vaccines—a reminder of the pandemic’s persistent toll—simply doesn’t register. Compared with the pandemic’s early days, we’re now “fighting complacency and fatigue” that wasn’t bogging us down before, says Angela Shen, a vaccine expert at Children’s Hospital of Philadelphia. Immunization ennui has created cracks into which anti-vaccine misinformation has quickly seeped. “It allowed the dominance of the negative messages,” Schulman told me, with a fervor that pro-vaccine messages have yet to match. With any vaccine, “there’s going to be a certain percentage drop-off each time you ask people to come back in,” says Elaine Hernandez, a sociologist and health demographer at Indiana University Bloomington. But America’s approach to boosters took that natural chasm and stretched it further out. This year, well-timed boosters, delivered in advance of winter, could blunt the wave that many experts forecast will begin to crash over the nation by year’s end. Recent modeling suggests that SARS-CoV-2 could kill up to 211,000 people from March 2022 to March 2023—making new vaccines essential to stem the tide. As things stand, the U.S. has little planned from now until the fall to make this booster push more successful than the last, and communicating the shots’ benefits will be far more difficult than it was in 2021, when the vaccines were fresh. If anything, the next rollout threatens to be one of the most constrained distribution efforts yet: COVID funding remains in congressional limbo, and federal officials have fretted that “we’re not going to have enough vaccines for every adult who wants one” this fall. If the current trends continue, “I don’t think we’re going to do any better” than the boosting rates the country has already clocked, Shen told me. That doesn’t have to be the case. With our first several vaccine rollouts, “we messed up,” Thomas, of the University of Maryland’s Center for Health Equity, told me, because the nation’s priorities were misaligned. Although billions of dollars were funneled to pharmaceutical companies so they could develop COVID vaccines in record time, no proportionate allocation of resources went to ensuring that those shots actually found their way into arms. And so, too many of them did not. The fall boosters will reignite those communication challenges, and add some of their own. The new formulation, selected months ahead of schedule, remains an inherent gamble. “We need an updated shot,” Shen told me. That decision has to happen now, in order for boosters to be manufactured by fall. But there’s no telling what Greek-letter threat will be ping-ponging around the globe by the time winter sets in, or how good a match the shots will be. Whatever Omicron variant is slotted in may no longer be pertinent by the time October begins. If BA.1 is the agency’s choice, that’s already the case. A BA.4- or BA.5-inspired shot might feel more current—but such a selection could push the entire timeline back: Some vaccine makers have already said they might need more time to cook up those shots en masse. Still, introducing (or reintroducing) vaccinated people’s bodies to any Omicron spike should broaden their defenses, even if the variant isn’t a perfect match for the version of the virus they see next. Should the FDA select a two-spike shot that includes the original variant as well, it will also offer immune systems a reminder of the SARS-CoV-2 morphs they’ve encountered before. The new message has to be that “the virus has changed, and now the vaccines have changed,” says Elizabeth Wrigley-Field, a sociologist at the University of Minnesota. The shots’ selling points, though, won’t be the same across the country. From the beginning, people have gotten vaccines for different reasons, on different schedules; attempting to collapse that diversity now may fail to actually bring people together. “The local variation is just remarkable,” Hernandez told me. Policies specific to one location just can’t be expected “to work the same way somewhere else.” For enthusiasts—people who can’t wait to dose up again—health officials might do well to play up the novelty of the autumn vaccine recipe, the hottest new model to hit the shelves. “The upgrade mentality is compelling,” Wood, of North Carolina State University, told me. “People like to have the most cutting-edge thing.” That won’t fly with everyone, however. Newness was the very thing some people feared about the COVID vaccines to begin with, Wood pointed out; highlighting an unfamiliar version of an already foreign-seeming product could exacerbate those concerns. To revamp communications around the new recipe, experts might even consider moving away from the term booster, a word people have come to link with the peak of pandemic crisis, and simply refer to regularly reformulated COVID vaccines as “another annual shot,” Schulman told me. A term like that might help soften “the emotional tone,” he said. People are already used to getting shots in the fall, thanks to the flu—a COVID vaccine could piggyback on that routine. [Read: America’s flu-shot problem is also its next COVID-shot problem] And in many of the communities that Thomas has worked with, people aren’t hinging their vaccination decisions heavily on the shots’ exact formulation, he said. Far more important is “who’s delivering it.” Any successful vaccination effort, he said, survives on maintaining trust long-term. “Once you have trust, everything flows from there.” His own efforts to increase vaccination have built on that principle—which has meant shifting the venues in which people expect to receive their shots. For more than a year, he and his colleagues have been been partnering with Black barbers and stylists across the country to turn hair salons into COVID immunization sites, where regulars can stop in for a trim, a shave, and a jab, all while getting their questions answered in a space that feels familiar and safe. The experts talking up the shots are often shop owners—“people they know from the community,” Thomas told me. “It’s about wrapping the message in a way that’s nonthreatening.” The same goes, he told me, for just about any vaccination drive. Many people are just eager to keep their loved ones safe, he told me, and want to hear that that’s possible to achieve from a nonjudgmental source. Messages like “Don’t let COVID come to your family reunion” and “Are your kids max-boosted?” partnered with images of grandmothers and children strongly resonate. Whatever the scale, the more infrastructure that’s around to support continued immunizations, the better. Reopening vaccination venues, with the help of renewed federal funds, this fall would help; so would reigniting outreach that brings shots to low-resource communities. Wrigley-Field notes that another crucial priority is maintaining access to vaccines, including first doses—the foundation on which boosters build. “There is this assumption that people have had their chance, and that mass vaccination sites and outreach campaigns are no longer needed,” she told me. “And I think that is just so wrong.” In Minnesota, she’s been working to deliver vaccines with the help of leaders from local mosques and pharmacies; a year and a half in, “we still find people who want to get their first shots when we talk with them,” she told me. “And there are people who know they want boosters, but haven’t had the opportunity, and people who are on the fence, but can decide to get it pretty quickly in a conversation where they can ask their questions.” For all the discussions that people have been having about what to put into our next vaccines, Thomas told me, “I’ve not heard anything about how that’s going to be communicated and rolled out.” Those conversations, he said, need to launch now, or risk never getting off the ground at all. from https://ift.tt/P2Nbqia Check out http://natthash.tumblr.com In 2018, while reporting on pandemic preparedness in the Democratic Republic of Congo, I heard many people joking about the fictional 15th article of the country’s constitution: Débrouillez-vous, or “Figure it out yourself.” It was a droll and weary acknowledgment that the government won’t save you, and you must make do with the resources you’ve got. The United States is now firmly in the débrouillez-vous era of the COVID-19 pandemic. Across the country, almost all government efforts to curtail the coronavirus have evaporated. Mask mandates have been lifted on public transit. Conservative lawmakers have hamstrung what public-health departments can do in emergencies. COVID funding remains stalled in Congress, jeopardizing supplies of tests, treatments, and vaccines. The White House and the CDC have framed COVID as a problem for individuals to act upon—but action is hard when cases and hospitalizations are underestimated, many testing sites have closed, and rose-tinted CDC guidelines downplay the coronavirus’s unchecked spread. Many policy makers have moved on: “We’re heading into the midterms, and I think there’s a real desire to show confidence that they’ve solved this,” Céline Gounder, an infectious-disease specialist and the editor at large for public health at Kaiser Health News, told me. But COVID is far from solved. The coronavirus is still mutating. Even at one of the lowest death rates of the pandemic, it still claims the lives of hundreds of Americans daily, killing more than twice as many people as die, on average, in car accidents. Its costs are still disproportionately borne by millions of long-haulers; immunocompromised people; workers who still face unsafe working conditions; and Black, Latino, and Indigenous Americans, who are still dying at higher rates than white Americans. When Kirsten Bibbins-Domingo, an epidemiologist and physician at UC San Francisco, works with low-income, Black, and Latino communities in the Bay Area, their concerns are less about returning to normal and more about “how to keep themselves safe,” she told me. “Take it from a tuberculosis activist that you can lose political will, public attention, and scientific momentum and still have a disease that kills over a million people each year,” Mike Frick of the Treatment Action Group told me. “We’re seeing the TB-ification of COVID start.” For any disease, there is a moral case against neglecting those who are most vulnerable; for COVID, there’s also still a self-interested case for even the privileged and powerful to resist the pull of neglect. For more than a year, the U.S. has focused on using vaccines and drugs to avert severe disease and death, while deprioritizing other means of preventing infections, such as masks and ventilation. To a degree, this strategy is working: Cases and hospitalizations recently spiked again, while ICU admissions rose gently and deaths have remained stable. And yet, infections still matter, and are affecting all of American society, including the vaxxed-and-done. The coronavirus periodically takes waves of educators and health-care workers out of action; the entire health-care system is now perpetually overburdened and unable to provide its former standard of care. People are still being disabled by long COVID, often without ever landing in the hospital. And uncontrolled infections are a gift to the virus, which keeps birthing new variants that could prolong the current level of crisis or send it spiraling back into a greater level of disruption. Many sensible policies—say, mask mandates that toggle on in grocery stores, public transport, and other essential spaces when community transmission is high—seem unlikely in this political climate. What, then, is still on the table? Right now, “I feel like I’m screaming into the wind,” Matifadza Hlatshwayo Davis, the health director for St. Louis, told me. But while others get to simply say “We’re screwed” and move on, she said, “I have to drive into work and figure it out.” Débrouillez-vous, indeed. I have interviewed dozens of other local officials, community organizers, and grassroots groups who are also swimming furiously against the tide of governmental apathy to push some pandemic response forward, even if incrementally. This is an endeavor that all of American society would benefit from; it is currently concentrated among a network of exhausted individuals who are trying to figure out this pandemic, while living up to public health’s central tenet: Protect the health of all people, and the most vulnerable especially. The late Paul Farmer, who devoted his life to providing health care to the world’s poorest people, understood that when doing such work, victories would be hard-won, if ever won at all. Referencing a line from The Lord of the Rings, he once said, “I have fought the long defeat.” In the third year of the COVID pandemic, that fight will determine how America fares against the variants and viruses still to come. In a study of 177 countries, people’s level of trust—in the government and especially in one another—predicted COVID infection rates and vaccine uptake. In America, trust is in short supply, and accordingly, the country has underperformed throughout the pandemic despite its considerable resources. This problem is getting worse: A poll from January found that only 44 percent of respondents trusted the CDC’s statements on COVID, down from 55 percent in 2020—a decline that spanned the political spectrum. As the pandemic has revealed, even powerful biomedical tools such as vaccines sputter in practice if disadvantaged people can’t access them, or if distrusting people refuse to use them. America’s recurring mistake is to create such technofixes at warp speed, while neglecting the systems that actually deploy those tools. Those systems—the country’s social infrastructure—are so porous that a multitude of smaller projects are necessary to patch each and every hole. Once lost, trust is hard to regain at scale. But it can slowly be rebuilt. America actually has an entire workforce that specializes in earning trust: community health workers. They’re hired for their empathy, their strong local ties, and their personal experience with hardship. Breanna Burke, a community health worker in Bristol, Tennessee, where she has lived since she was 3, told me that her job is to “get to the root cause of ongoing health issues,” with the understanding that a person’s circumstances constrain their choices. For example, she helped one of her diabetic clients plan a budget to keep their power on so they could keep their insulin cold; another time, she figured out that a patient whose pain wouldn’t stop had been sleeping on a hardwood floor for nine months, and contacted a local women’s club to raise money for a mattress. When COVID hit, Burke provided people with emergency food supplies so they could weather quarantine in safety, and talked others through their hesitancy over getting vaccinated. She can do that because her nonjudgmental approach and shared life experience make her trustworthy—the secret to community health workers’ extraordinary effectiveness. In three randomized trials involving people living in poor parts of Philadelphia, Shreya Kangovi, a physician at the University of Pennsylvania, showed that people who see community health workers spend 66 percent fewer days in the hospital than those who receive usual care. In her research, Kangovi also found that every dollar invested in said workers returns $2.47 to the average Medicaid payer. If their work on COVID prevention fulfills even part of that promise, it could be a crucial lifeline for the badly stretched health-care system. Such efforts are part of a long-standing tradition. In the early 20th century, public health was a broader enterprise than it is now. It included not just physicians and scientists, but also labor-union leaders, housing reformers, and social activists, who attempted to right big societal problems such as unsafe workplaces and dilapidated neighborhoods. Even as the field professionalized, pockets of people with no official qualifications repeatedly stepped up to protect their communities’ health. Alongside their more radical activities, the Black Panther Party and the Young Lords provided vital health services for Black and Puerto Rican communities in the 1970s. In the ’80s and ’90s, ACT UP—the AIDS Coalition to Unleash Power—fought for the creation of HIV treatments, and changed the legal definition of AIDS and the way the FDA approved new drugs. More recently, Stephen B. Thomas, a health-policy professor at the University of Maryland who has turned Black barbers and stylists into health-care advocates, worked with those shops and salons to provide COVID vaccines. And in early 2021, the sociologist Elizabeth Wrigley-Field and a small group of volunteers began setting up their own vaccination events at local mosques, for the many East African refugee and immigrant families in their neighborhood of Seward, Minnesota. The community had been heavily targeted with vaccine misinformation for more than a decade, but the group, the Seward Vaccine Equity Project, included trusted local figures—Inari Mohammed, an Oromo epidemiology student and long-standing member of a neighborhood mosque; Saida Mohamed, a gregarious Somali pharmacy owner whose store doubles as a social hub; and Ramla Bile, an experienced Somali civil-rights organizer. They identified local leaders, including a soccer coach and a local union staffer, and recruited attendees through conversations at Section 8 house towers and immigrant-owned small businesses. Ultimately, they delivered more than 500 vaccine doses. That might seem insignificant when 73 million Americans remain unvaccinated, but several hundred Seward residents are now substantially safer, which Wrigley-Field counts as a win. The impact of community work can feel small in the face of a pandemic’s scale, as if people are merely mopping up the stragglers left behind by national initiatives. In fact, such work is foundational. It creates a bedrock of trust and solidarity, without which public health cannot operate. The problem isn’t that community work is trivial; it’s that there hasn’t been enough of it. And for many of the people I spoke with, such work acts as a vaccine against nihilism. The pandemic has fostered beliefs that people are inherently selfish or permanently polarized. Neither is true, Wrigley-Field told me: Despite the persistent myth that unvaccinated people today are all unreachable holdouts, “every time we organize an event, people come,” she said. She and her team were still giving people their first doses this January. Her goal is now simple: “Do something that helps, even when it’s very small,” she said. “I believe that doing the small stuff now is setting us up for bigger things.” Going bigger means ultimately compelling state or federal governments to commit to some kind of sustained COVID response. Over the past two years, tranches of concerned Americans have begun to coalesce into new interest groups, for whom public health is a top priority, to push for better pandemic protections. Public-health professionals often lament that the field has been consistently underfunded because it lacks a vocal constituency. But as the historian Amy Fairchild of Ohio State University and her colleagues have noted, public health had more political power in the early 20th century partly because it allied itself with a broader coalition of organizations. It now has a rare chance to rebuild those alliances. After Kristin Urquiza’s father died of COVID in June 2020, she founded the nonprofit Marked by COVID—a group of activists united in their grief and their desire to permanently memorialize America’s 1-million-plus COVID deaths. The group now has about 100,000 members, Urquiza told me. In 2017, when the longtime activist Paul Davis helped coordinate a nationwide campaign to save the Affordable Care Act, he thought his database of 7,000 people was “huge,” he told me. Now he is the policy director of Right to Health Action, an advocacy group that formed in the spring of 2020, and his database of COVID activists “is about 150,000,” he said. Other groups represent the millions of long-haulers who have been wrestling with the debilitating symptoms of long COVID, or communities that have been disproportionately harmed by the pandemic. A mixed team of public-health practitioners, health-care workers, educators, and others created the People’s CDC to “push back on harmful narratives that we don’t need COVID protections,” such as testing and masks, Lucky Tran, an activist and a science communicator, told me. Though disparate, these groups share many qualities. Many feel abandoned by their government. Many feel that they cannot return to “normal,” and that a better normal can be fashioned instead. Many aren’t interested in shaming people over individual choices, but want structural changes that will make society safer for everyone. And most, to be blunt, are really pissed. In this, they could be successors to ACT UP, which was immensely effective despite staying relatively small: “A few thousand people were able to win lifesaving AIDS treatments for millions,” Davis, who is an ACT UP alumnus, told me. The pandemic activists he now works with dwarf that old community in numbers, and to his mind are just as motivated. Long-haulers have already won important victories, including pressing institutions such as the World Health Organization and the CDC to formally recognize long COVID, and so securing substantial research dollars for long-COVID research from the National Institutes of Health and private philanthropists. Their symptoms often keep them depleted physically and mentally, but although this work only adds to their strain, they feel they have no choice but to do it. “Our pain, grief, and disability isn’t going away,” Lisa McCorkell, a long-COVID advocate and co-founder of the Patient-Led Research Collaborative, told me. Groups of impassioned but inexperienced activists can often struggle to do little beyond merely existing. Achieving power in the U.S. requires more than angry individuals, Jane McAlevey, an organizer and the author of A Collective Bargain, told me; it needs “a well-built organization that can actually channel people’s rage effectively,” she said. ACT UP did that by drawing wisdom from its predecessors, and becoming “involved with basically every community that was vulnerable at the time,” as the historian Sarah Schulman once said. Similarly, several of the newly formed pandemic groups have already started working with one another, veterans of ACT UP, organizations advocating for chronic illnesses like myalgic encephalomyelitis, and health-care workers’, teachers’, and labor unions. These groups vary considerably in their goals, which include permanent COVID memorials, better funding for long COVID, global vaccine equity, and more. These goals aren’t mutually exclusive, but the protoplasmic coalition still “needs a skeleton, an organizing principle to tie it together,” Gregg Gonsalves, a Yale epidemiologist and ACT UP alumnus, told me. That could be as simple as a push for a robust public-health system that centers the needs of the most vulnerable people. ACT UP achieved its many concrete victories without insisting that its members conform to specific messages, uniting instead around the idea that HIV deserved more public attention. Building a stronger public-health system demands an unfettering of the moral imagination: Americans need to believe that their government should invest in systems that keep everyone safer from disease—and to trust that such systems are even possible. But throughout his decades-long career, Gonsalves has witnessed social safety nets being repeatedly shredded, leading to “a collapse of any faith in the state to do good,” he told me. That faith eroded further when public institutions buckled during the pandemic, and when two successive administrations failed to control the coronavirus. The resulting “pandemic fatigue” is not just a craving for the status quo, but a deep cynicism over the possibility of something better. In one study, most Americans preferred a better, fairer post-pandemic future, but mistakenly thought a “back-to-normal” one was more popular—and so more likely. “People can imagine a world with crypto-banking and the metaverse, so why is it so hard to imagine a world with less disease and death?” Céline Gounder of Kaiser Health News said. Even in the débrouillez-vous era, the nascent COVID constituency can still push for big policies that would prevent disadvantaged groups from suffering a disproportionate burden of disease and death. In December 2021, as Omicron swept the U.S., then–White House Press Secretary Jen Psaki replied sarcastically when a reporter asked why rapid tests weren’t widely available. “Should we just send one to every American?” Psaki said. But after two weeks of public outcry, the administration announced plans to do just that. To date, every household has been able to order up to 16 free tests—still insufficient, months too late, but invaluable nonetheless for families that can’t afford these expensive products. Several people I talked with mentioned the rapid-test turnaround as a rare and recent example of a positive, nationwide pandemic policy—and a sign that such policies are still achievable. Similarly, the government could still promote the use of masks even if it won’t mandate them when the risk of transmission is high. In the 2000s, as HIV faded from public concern, health departments responded by making condoms as accessible as possible; New York City alone distributes tens of millions every year to bars and nightclubs. As Jay Varma, a physician at Weill Cornell Medicine who advised the New York City mayor’s office during the pandemic’s first year, has suggested, states and cities could follow the same playbook now, flooding public indoor spaces with free, high-quality masks, such as KF94s, KN95s, or N95s. Doron Dorfman, a disability-law expert at Syracuse University College of Law, is also leveraging the court system in favor of masking. He argues that requiring people to wear masks around immunocompromised students or employees—who may still have higher risks of infection and illness despite being vaccinated—counts as a reasonable accommodation under the Americans With Disabilities Act; the Eighth Circuit Court of Appeals accepted this argument, as did a federal district court in Virginia. “Even if you get crumbs from the federal government, the scale is such that even crumbs save a lot of lives,” Matthew Cortland, a disabled policy analyst and lawyer at Data for Progress, told me. Cortland and others see the greatest potential in improving the air we breathe. The coronavirus spreads primarily through shared air, making indoor spaces riskier than outdoor ones. After misguidedly focusing on surface-cleaning hygiene theater, both the government and industry leaders are now starting to grasp the importance of ventilation and filtration. The White House has launched a Clean Air in Buildings Challenge (but falls short of actually mandating businesses to take action or providing dedicated funding). Varma and Cortland have both pitched officials the idea of assigning public buildings letter grades for air quality, just as there are grades for food safety in restaurants; that would tell immunocompromised people which essential spaces are safer in the absence of mask mandates. “People really like being able to breathe! Across the political spectrum!” Cortland told me, dryly. What’s missing, Cortland said, are detailed checklists of the kind that tell businesses how to make physical spaces accessible to disabled people; nothing similar exists for indoor air. “Businesses are telling me they need granular guidance, and it’s not there,” Cortland said. “But it could be.” Cities and counties can also act in the face of sluggish national policy. The antiviral Paxlovid is effective only when taken shortly after symptoms first appear, so New York City created a free, same-day home-delivery system for the drug, and the city’s hotline also works for people who don’t have a regular doctor. Manhattan Borough President Mark Levine has been working on COVID safety bags—tests, high-quality masks, and Paxlovid information—that can be sent to every home or distributed via community groups. Alameda County, in California, recently reinstated an indoor mask mandate because of growing hospitalizations, and other left-leaning areas could follow suit: Polling by Data for Progress found that 80 percent of Democratic voters support mask mandates on public transportation, for instance. “Maybe that’s a place where local public-health activism can make an impact,” Cortland told me. Activist groups can also push for grander upgrades to the U.S. public-health system, and longer-term funding to safeguard them. During the pandemic, the U.S. plastered over the wounds of its bleeding institutions with “taped-together systems of volunteers” and temporary scale-ups of important services such as testing and contact tracing, Amy Kapczynski, a global-health expert at Yale Law School, told me. When these Band-Aids fall off, the wounds beneath them reopen. What the U.S. needs, instead, is to rebuild its “infrastructure of care,” Kapczynski said, so that its epidemic responses aren’t subject to boom-and-bust cycles of emergency funding, and so that vulnerable populations aren’t left in the lurch whenever attention and resources wane. It could, for example, massively expand its corps of community health workers, who are often overlooked because they “tend to be rural people, people of color, and women, without a lot of letters behind their name,” Kangovi, the UPenn physician, told me. In the U.S. there are just 61,000 of them, in contrast to roughly 1 million physicians—a ratio indicative of a health-care system that “waits for people to get sick and feeds them to us to make a livelihood off of,” Kangovi said. For years, doctors and nurses have been called frontline workers, and therein lies the problem: If emergency rooms are the front lines of a nation’s pandemic response, that response has already failed. The real front lines are in people’s homes—the places where community health workers operate. The Biden administration has committed $226.5 million to training another 13,000 community health workers, which still feels insufficient for a country that spent $4.1 trillion on health care in 2020. Had a bigger system been in place before COVID arrived, “it would have made a real difference,” Kapczynski said, echoing many others I interviewed. Several of America’s biggest pandemic problems—plateauing vaccination rates, the mental-health toll, the erosion of trust—are exactly the problems that community health workers are good at solving. Scaling up their numbers could effectively be an Operation Warp Speed for trust—a way of making face-to-face solutions work at a national scale. The débrouillez-vous phase of the pandemic will be as patchwork as those that preceded it. And there are limits to what local officials can do in the absence of “anything even remotely resembling a national coordinated response,” Lindsay Wiley, a health law expert at UCLA, told me. Philadelphia, for example, reinstated an indoor mask mandate in April as local case numbers rose, only to rescind it four days later. There used to be “a clear understanding that locals would implement the CDC’s guidance in a way that worked best in their community,” Theresa Chapple, a local public-health official in the Chicagoland area, told me. “Now, if you’re doing anything different, it’s seen as going against the CDC.” Matifadza Davis, the St. Louis health director, told me the city has the authority to reinstate a mask mandate, but that it’s hard to use that power when surrounding counties won’t—or risk being sued by the state’s attorney general if they try. “Getting sued like that is exhausting, and we have a country full of health officials who’ve spent years dealing with lawyers and judges,” Wiley said. “There’s a chilling effect.” States also can’t spend at a deficit; only the federal government can. Only federal leaders have the power and pockets to approve new vaccines and buy them at scale; to distribute vaccines to poorer countries that still desperately need them; to force a systematic improvement in indoor air; to push for universal paid sick leave and other measures that would allow vulnerable workers to protect their health without risking their income; and to truly create what the U.S. so sorely needs—a sustainable infrastructure that can keep more people from getting COVID, regardless of their social circumstances. Such a world is always possible. The 1960s and ’70s saw a bloom of bold public-health initiatives—the passage of the Clean Air Act, the Clean Water Act, Medicare, and Medicaid, and the creation of the Environmental Protection Agency, the Occupational Health and Safety Administration, and what are now called federally qualified health centers. Upcoming decades could still witness a similar blooming. “What’s standing in the way? It’s our political will—the way we think about our society and ourselves,” Beatrice Adler-Bolton, who co-hosts Death Panel, a podcast about the political economy of health, told me. “As we’ve gone through the pandemic, and our hope for policies has been ratcheted down, there still needs to be room for big ideas.” As a disabled person who studies disability, she has had to repeatedly renew her own sense of worth in the face of social structures that dismiss her value. That has made her practiced at hoping and calling for transformative policies. She echoes the organizer and abolitionist Mariame Kaba in saying “hope is a discipline”—not a fuzzy emotion, but the product of effortful work. And “in the process of imagining what could be better, I find hope,” Adler-Bolton said. from https://ift.tt/zhBqbM1 Check out http://natthash.tumblr.com The past two and a half years have been a global crash course in infection prevention. They've also been a crash course in basic math: Since the arrival of this coronavirus, people have been asked to count the meters and feet that separate one nose from the next; they’ve tabulated the days that distance them from their most recent vaccine dose, calculated the minutes they can spend unmasked, and added up the hours that have passed since their last negative test. What unites many of these numbers is the tendency, especially in the United States, to pick thresholds and view them as binaries: above this, mask; below this, don’t; after this, exposed, before this, safe. But some of the COVID numbers that have stuck most stubbornly in our brains these past 20-odd months are now disastrously out of date. The virus has changed; we, its hosts, have as well. So, too, then, must the playbook that governs our pandemic strategies. With black-and-white, yes-or-no thinking, “we do ourselves a disservice,” Saskia Popescu, an epidemiologist at George Mason University, told me. Binary communication “has been one of the biggest failures of how we’ve managed the pandemic,” Mónica Feliú-Mójer, of the nonprofit Ciencia Puerto Rico, told me. Here, then, are five of the most memorable numerical shorthands we’ve cooked up for COVID, most of them old, some a bit newer. It’s long past time that we forget them all. 2 doses = fully vaccinated At the start of the vaccination campaign, getting dosed up was relatively straightforward. In the United States, a pair of Pfizer or Moderna shots (or just one Johnson & Johnson), then a quick two-week wait, and boom: full vaccination, and that was that. The phrase became a fixture on the CDC website and national data trackers; it spurred vaccine mandates and, for a time in the spring and summer of 2021, green-lit the immunized to doff their masks indoors. Then came the boosters. Experts now know that these additional shots are essential to warding off antibody-dodging variants such as the many members of the Omicron clan. Some Americans are months past their fifth COVID shot, and the nation’s leaders are weighing whether vaccinated people will need to dose up again in the fall. To accommodate those additions, the CDC has, in recent public communications, tried to shift its terminology toward “up to date.” Katelyn Jetelina, an epidemiologist at the University of Texas Health Science Center at Houston, prefers that phrase, because it “allows for flexibility” as recommendations evolve. It also more effectively nods at the range of protection that vaccination affords, depending on how many doses someone’s gotten and when their most recent dose was. But fully vaccinated has been hard to shake, even for the CDC. The agency, which did not respond to requests for comment, maintains that the original definition “has not changed,” and the term still features heavily on CDC websites. Maybe part of the stubbornness is sheerly linguistic: Up to date means something different to everyone, depending on age, eligibility, health status, and vaccine brand. Fully vaccinated is also grabby in a way that up to date is not. It carries the alluring air of completion, suggesting that “you’re actually done with the vaccine series,” maybe even the pandemic overall, Jessica Malaty Rivera, an epidemiologist and adviser at the Pandemic Prevention Institute, told me. All of this may be partly why that uptake of boosters—which sound optional, even trivial, compared with the first two shots--remains miserably low in the U.S. < 6 feet + > 15 minutes = close contact Since the pandemic’s early days, Americans have been taught to benchmark our risk of exposure to the virus by two metrics: proximity and duration. Get within six feet of an infected person for at least 15 minutes over a 24-hour period, and congratulations—you’ve had a “close contact.” Even now, the CDC advises that this kind of encounter should trigger 10 full days of masking and, depending on your vaccination status and recent infection history, a test and/or a five-day quarantine. Thresholds such as these made some sense when researchers weren’t yet savvy to the virus’s main modes of transmission, and at least some efforts were made to contact trace, Jetelina told me. “You needed some metric so you could call people.” Nearly all contact-tracing attempts, though, have long since fizzled out. And scientists have known for years that SARS-CoV-2 can hitch a ride in bubbles of spittle and snot small enough to drift across rooms and remain aloft for hours, especially in poorly ventilated indoor spaces. Pathogens don’t slam up against a magic wall “at the six-foot mark,” Malaty Rivera said. Nor will viruses bide their time for 14 minutes and 59 seconds before launching themselves noseward at 15 minutes on the dot. Exposure is a spectrum of high to low risk” that factors in, yes, proximity and duration, but also venue, ventilation, mask quality, and more, Popescu said. “It’s not just ‘exposed’ or ‘not exposed.’” The CDC acknowledges that SARS-CoV-2 can move beyond six feet—but the scientific justification behind its guidelines on preventing transmission was last updated in May 2021, just before the Delta variant bamboozled the nation. Since then, the coronavirus has gotten even more contagious and crafty—better at transmitting, better at dodging the antibodies that people raise. “Even passing interactions and encounters have led to people becoming exposed and infected,” Malaty Rivera said, especially if people are indoors and a ton of virus is being volleyed about. And yet, the mantra of “six feet, 15 minutes” has stayed. Schools have even cut the guidance in half, counting close contact only when children are less than three feet apart. 5 days = end of isolation In the beginning, isolation numbers loomed large: Infected people had to wait at least 10 days after their symptoms began, or after their first positive test result, before they could reenter the world. Then, at the start of 2022, the CDC slashed the duration of isolation to just five days for people with mild or asymptomatic cases (regardless of vaccination status), as long as they kept masking and avoided travel through Day 10. You didn’t even need a negative test to go about your life. This guideline has been perpetually behind the times. For much of 2021, truncating isolation might have made sense for vaccinated people, who clear the coronavirus faster than folks who haven’t gotten their shots, especially if negative tests confirmed the safety of exit. But only after the rise of Omicron did the guidance change—and it was based mostly on pre-Omicron data. The shift in guidance arrived just in time for the coronavirus to bust it wide open. After nearly two years of COVID symptoms starting around the time people first began to test positive, test positivity with Omicron and various iterations is now quite frequently lagging the onset of illness. Many people now report strings of negative results early in their symptom course, then positives that persist into their sixth, seventh, or eighth day of sickness or later, raising the possibility that they remain quite contagious past when formal isolation may end. “I find it impossible to believe you can end isolation without testing,” Malaty Rivera said. [Read: A negative COVID test has never been so meaningless] And yet, many workplaces have already embraced the five-day rule with no exit test, using that timeline as the basis for when employees should return. With masks largely gone, and paid sick leave so uncommon, defaulting to five days could drive more transmission—in some cases, likely inviting people back into public when they’re at their infectious peak. Infection + 90 days = no retest According to CDC guidelines, people who have caught SARS-CoV-2 don’t need to test or quarantine if they’re exposed again within 90 days of their initial infection. This recommendation, which appeared in the pandemic’s first year, was designed in part to address the positives that can crop up on PCR tests in the weeks after people stop feeling sick. But the CDC also touts the “low risk of subsequent infection for at least 6 months” on one of its pages, last updated in October 2021. Reinfections “can occur” within 90 days, but that’s “early.” That framing might have once been pretty solid, before the era of widespread at-home antigen testing—and before the rise of antibody-dodging variants, Popescu said. However, reinfections have gotten more common, and far closer together. They were happening even in the era of Delta; now, with so many immunity-evading Omicron offshoots at the helm, and masks and other mitigation matters mostly vanished, they’ve become a quite-frequent fixture. The number of people who have caught the virus twice within just a matter of weeks “has grown so much that we should forget these windows,” Malaty Rivera said. Even the Department of Health and Human Services secretary recently tested positive twice in the same month. [Read: You are going to get COVID again … and again … and again] And yet, with these guidelines in place, many people have been lulled by the promise of rock-solid post-infection immunity, assuming that a new crop of symptoms are “anything but COVID,” Malaty Rivera said. That thinking is not only allowing a growing share of contagious coronavirus cases to go undetected—it’s also stymieing the study of reinfection dynamics writ large. Many studies, including those cited by the CDC in its guidance, won’t even count reinfections earlier than 90 days. But the 90-day number, Malaty Rivera said, is no longer relevant. “It has to be deleted from people’s minds.” 200 cases + 10 hospital admissions per 100,000 = mask? As obsolete as some of America’s COVID calculations may be, updates aren’t a universal win, either. Take the most recent iteration of mask recommendations from the CDC. The agency would like everyone to mask indoors if their county hits a “high” COVID community level, a threshold that is met only when the region logs 200 or more infections per 100,000 people in one week, and if local hospitals see more than 10 COVID-related admissions per 100,000 people in a week, or fill at least 15 percent of their inpatient beds. Currently, roughly 10 percent of U.S. counties are in the “high” category. [Read: The Biden administration killed America’s collective pandemic approach] But waiting to just suggest masks at those levels of transmission and hospitalization—not even require them—leaves far too much time for widespread disease, disability, even death, experts told me. A bar that high still lets long COVID slip through; it continues to imperil the vulnerable, immunocompromised, and elderly, who may not get the full benefit of vaccines. Case rates, Malaty Rivera pointed out, are also a terrible yardstick right now because so many people have been testing at home and not reporting the results to public-health agencies. In Puerto Rico, Feliú-Mójer and her colleagues have been struggling to reignite enthusiasm for mask wearing as their community battles its second-largest case wave since the start of the pandemic. A better system would flip on protections earlier—taking a preventive approach, rather than scrambling to react. But that’s a difficult stance for jurisdictions to assume “when the official map looks so green and a little yellow,” Feliú-Mójer said. It’s the problem of thresholds striking once again: No one cares to take up arms anew against the virus until the damage is already done. That’s made the pandemic that much easier to tune out—it’s either here in full force, the thinking goes, or it’s totally gone. If only the calculus were that simple. from https://ift.tt/voaRgPy Check out http://natthash.tumblr.com In the summer of 2003, just weeks after an outbreak of monkeypox sickened about 70 people across the Midwest, Mark Slifka visited “the super-spreader,” he told me, “who infected half of Wisconsin’s cases.” Chewy, a prairie dog, had by that point succumbed to the disease, which he’d almost certainly caught in an exotic-animal facility that he’d shared with infected pouched rats from Ghana. But his owners’ other prairie dog, Monkey—named for the way he clambered about his cage—had contracted the pathogen and survived. “I was a little worried,” said Slifka, an immunologist at Oregon Health & Science University. All the traits that made Monkey a charismatic pet also made him an infectious threat. He cuddled and nibbled his owners; when they left the house, he’d swaddle himself in their clothing until they returned. “It was sweet,” Slifka told me. “But I was like, ‘Can Monkey be in his cage when we come over?’” Slifka made it home pox-free, and the 2003 outbreak fizzled out. But that rash of cases was a close call: an opportunity for the virus to set up shop in a new animal host. One lasting interspecies hop, akin to the one that SARS-CoV-2 has made into white-tailed deer, and monkeypox will be “with us forever” in the U.S., says Barbara Han, a disease ecologist at the Cary Institute, in New York. In Central and West Africa, where the virus is endemic, scientists suspect that at least a couple of rodent species intermittently slosh it into humans. And as the largest-ever epidemic of monkeypox outside of Africa in history continues to unfurl--more than 2,700 confirmed and suspected cases have been reported across roughly three dozen countries—the virus is now getting plenty more shots on goal. This time, we may not get so lucky; the geography of monkeypox might soon change. Any new leaps could reshape the future for this virus, and for us. Experts consider the possibility unlikely—“low risk, but it is a risk,” says Jeffrey Doty, a disease ecologist at the CDC. Existing animal reservoirs make some diseases near impossible to snuff out; the emergence of new ones could seed future outbreaks in places where they’re not currently common. If researchers can ID some of those animals, and keep them from mingling with us, we could head off a few of those issues. But that’s a big if. With so many susceptible animals out there, figuring out which ones harbor the virus could send researchers on a yearslong race, without a clear finish line. Scientists first discovered monkeypox in the 1950s, in two species of monkeys housed at a Danish animal facility; hence the name, which will likely change soon. But in the decades since, the best evidence of the virus lingering in animals has been tugged from rodents in Central and West Africa, including rope squirrels, sun squirrels, Gambian pouched rats, and dormice. All signs point to rodents being “responsible for maintaining this virus in the wild,” Doty told me, and so he and his colleagues worry most about those mammals when they ponder what animals in non-endemic regions may pose the most future risk. But a lot of rodents scurry the planet--about 2,500 species, which together make up roughly 40 percent of known mammals. Though not all species are capable of carrying monkeypox—for example, guinea pigs, golden hamsters, and common mice and rats usually don’t—many of them can. Building the case for an animal reservoir tends to require years of fieldwork, rigorous safety protocols, and a good deal of luck. For a few viruses, the reservoir narrative is relatively neat: Hendra virus, an often-fatal respiratory infection, typically moves from bats to horses to people; most hantaviruses, which can cause lethal fevers, set up shop in one rodent species each. Monkeypox, however, is far less picky than that. Experts suspect that multiple animals keep the virus percolating in the wild. Just how many, though, is anyone’s guess. [Read: Monkeypox could be nothing—or it could be the next syphilis] The gold standard for establishing a reservoir requires isolating active virus—proof that the pathogen was xeroxing itself inside of a viable host. But in the wilds of nature, “you can break your back and end up getting only five animals from a species,” Han, who’s been using machine learning to try to predict potential monkeypox reservoirs, told me. “And what’s five animals?” They may lack the virus in question, even if other members of their population harbor it; they may have been caught at an age, or during a season, when the pathogen’s not present. And among the animals that host the virus, a reservoir might not always be the most obvious species: Rodents might be among the most commonly detected carriers of monkeypox, but zoo outbreaks and laboratory experiments have shown the virus to be capable of infiltrating anteaters, rabbits, and a hefty handful of primates, along with other un-mousy mammals. In several of these species and others, scientists have found antibodies that recognize poxviruses, hinting at past exposures; they’ve even uncovered the virus’s DNA. Only twice, though, has anyone found active virus in wild animals: a rope squirrel from the Democratic Republic of Congo in the 1980s, and a sooty mangabey, found in Côte d’Ivoire about a decade ago. Even those cases weren’t slam dunks. It takes more to “figure out which one is a reservoir, versus which ones get infected, but aren’t actually responsible for maintaining circulation of the virus in people,” Jamie Lloyd-Smith, a disease ecologist at UCLA, told me. Just because an animal could bop the virus into us doesn’t mean that it will. For that to happen, humans need to have enough contact with the animals to make exposure likely—on routine hunts for bushmeat, for instance, or in fractured landscapes where animals forage for food in and around people’s homes. Lloyd-Smith, who has been surveying residents of the Congo, said parsing what’s risky and what’s not is tougher than it sounds: Most everyone he speaks with interacts with forest creatures all the time. “It’s not like, ‘Oh, it was the people who ate the salmon mousse at the church breakfast,’” he told me. To complicate matters further, wild and domesticated animals can act as intermediaries between humans and a true reservoir, says Stephanie Seifert, a disease ecologist at Washington State University. Researchers sometimes have to traverse webs of interaction, moving through Kevin Bacon–esque degrees of separation, to pinpoint the original source. Unveiling those natural origins is key to blocking the virus from moving onto new real estate—and, perhaps, breaking existing tenancies. In Central and West Africa, for instance, where some people’s livelihoods depend on hunting and eating wild game, “You can’t just say, ‘Don’t interact with rodents,’” Seifert told me. But with more investigation, says Clement Meseko, a veterinarian and virologist studying the human-wildlife interface at Nigeria’s National Veterinary Research Institute, perhaps experts could eventually pinpoint just a couple of species, then recommend sustainable alternatives in their place. Improved sanitation to keep rodent pests away from humans could also help. So could doling out vaccines to people who live in the high-risk regions of endemic countries—or perhaps to worrisome wild animals themselves. (Immunizing animals is a pretty lofty goal, but may still be a better alternative to culling animals, which “often doesn’t work,” Lloyd-Smith said.) [Read: Monkeypox vaccines are too gnarly for the masses] In the U.S., amid the current rash of monkeypox cases, the CDC has recommended that infected people avoid interacting with pets, livestock, and other animals altogether. Though no cat or dog has ever been known to contract the infection, “we basically know nothing about monkeypox in common companion animals,” Doty said. For now, it’s best to play it safe. And the most meaningful way to keep the virus from surging into a new animal species, Han said, “is to control the human outbreak.” Already, monkeypox’s species range is formidable, and in today’s world, humans and animals are colliding more frequently. Amid the ongoing outbreak, Meseko, who is spending the year completing a fellowship in St. Paul, Minnesota, has been taking note of “how squirrels are just free all over the place.” Whatever threat they might pose to us, “animals are also in danger from humans,” he told me. Human activity, after all, brought monkeypox to the U.S. in 2003, and into a coterie of prairie dogs that included Chewy and Monkey. “They would not have been exposed geographically without us moving around this virus,” Seifert said. And the human desire for pets brought those prairie dogs into dozens of midwestern homes. People mobilize disease; our species, too, poses an immense infectious threat to the planet. The current monkeypox outbreak, for instance, is more sprawling and human-centric than those documented in the past. And the more opportunity the virus has to infiltrate new hosts, the more opportunity it has to expand its species range. Any trickle into animals might not be detected until too late; perhaps, some experts pointed out, it already occurred long ago, seeding a reservoir that helped the ongoing epidemic erupt. “We have no evidence of that right now,” says Grant McFadden, a poxvirus expert at Arizona State University. “But that could change on a dime.” from https://ift.tt/NK7DlY8 Check out http://natthash.tumblr.com Unprecedented flooding in the Yellowstone area on Monday, June 13, inundated homes, devoured roads, swept away bridges, isolated entire towns, and shut down one of America’s busiest and most famous national parks. It was yet another indication of the impacts that climate change is likely to have on flood- and drought-ridden communities across the West. In Livingston, Montana, a town of about 8,000 an hour north of Yellowstone National Park, dozens of people stood along a levee Monday morning, watching chocolate-milk-colored water chug through. I was one of them. A torrent of mud, foam, and logs surged by us. A cool, wet spring had left the area with a far greater snow-water equivalent than normal. Warming temperatures combined with two to three inches of rain sent more than five inches of snowmelt in the mountains in and around Yellowstone—especially the Beartooths and the Absarokas—sheeting into the Yellowstone River and its tributaries. The Yellowstone runs from the heart of the park through Livingston. I live less than a half mile from the river. By about noon, the river was raging at about 50,000 cubic feet a second. Federal data show the volume of water rushing through the river had reached about 32,000 CFS just three times over the past 130 years. But the flow on Monday nearly doubled the previous record. Soon, those same data showed, river levels were nearly two and a half feet higher than ever recorded. A climate assessment for the Greater Yellowstone Ecosystem, put together by Montana State University, the University of Wyoming, and the United States Geological Survey, among others, showed that the Upper Yellowstone area warmed by about 2 degrees Fahrenheit from 1950 to 2018. Over the same time period, peak river flows began arriving about 12 days earlier, and late spring rain across the Greater Yellowstone Area rose by 20 percent. “It’s amazing and awe-inspiring, but it’s also exactly what we as climate scientists have expected for decades,” says James Marshall Shepherd, director of the atmospheric-sciences program at the University of Georgia and former president of the American Meteorological Society. He explained that climate change is causing the water cycle to accelerate, fueled by earlier snowmelt combined with more and more intense rainfall. “It’s a tale of two extremes,” Shepherd told me. At the same time that much of the West is facing debilitating heat waves, extreme wildfires, and the worst drought in 1,200 years, climate change is also amplifying the worst rainfall events, including the “atmospheric river” that dumped moisture on the Yellowstone area. On Monday, the water rushing out of the mountains in and around Yellowstone National Park swelled the river and hurtled downstream. Gardiner and Cooke City, towns near the park, were cut off from supplies of food and water. Downtown Red Lodge, another park-adjacent town, was soon underwater. The floods tore huge chunks from roads throughout the northern section of Yellowstone itself. The entire park shut down, and 10,000 tourists were evacuated. “I’ve heard this is a 1,000-year event, whatever that means these days,” Yellowstone’s superintendent, Cam Sholly, said at a press conference on Tuesday. “They seem to be happening more and more frequently.” Soon, my own house was under pre-evacuation notice, along with other parts of Livingston near the river. My partner and I packed up valuables and all we’d need for a couple of nights away. We picked everything we could up off the floor in case the house flooded, and we loaded our dog into the car. We got word from a friend, Celeste Mascari, that she could use some help protecting her home. Mascari lives about 700 feet from the river and runs a Montessori school on her property. When we arrived, the school’s crawl space was already flooded, and water was fast approaching from her backyard. Mascari, who grew up in the area, said that one of her brothers had probably lost his house, while another had lost his greenhouse, and a chunk of his income with it. We surrounded the house and school with sandbags. But within a couple of hours, the water had breached the perimeter. Panicked, we created new barriers and dug trenches to help drain the water from the yard. We left when the water in the street reached the height of a car tire; we knew we had done all that we possibly could. Soon after, we got the official order to evacuate our own house. We stayed with friends who live on a hill on the other side of town. I could barely sleep, wondering what was happening to our home—and to the rest of the community. About a mile away from our house, water had begun to trickle over the levee that separated the town from the river. If the levee breached, certain chaos would follow. That trickle grew, and by about 8:30 p.m., it seemed hopeless, Erica Lighthiser, the deputy director of the nonprofit Park County Environmental Council, told me. But then, she said, some 50 community members joined the effort, filling and placing sandbags. They worked at bolstering the levee until well after midnight—and it held back the water. Lighthiser said the whole experience was a lesson in the community’s resilience. “It took everybody, and that was pretty amazing to see,” she said. “But I think it’s going to take me some more time to really process all this.” That’s a feeling I could relate to. By morning, our house was still dry. But the barriers we’d erected around Mascari’s property hadn’t held. Her school was knee-deep in water, and friends, volunteers, and I scrambled to clean up and assess the damage. The governor's office declared a statewide disaster. The local hospital in Livingston was evacuated. Employees of the local animal shelter narrowly escaped the flooding with their animals. People lost their homes and their livelihoods, and were separated from their loved ones. Livingston and other towns affected by the flooding rely on the roughly $642 million dollars, as of 2020, that Yellowstone tourism injects into local economies. Much of that money is likely to dry up along with the floodwaters. The extensive damage in the northern part of the park means that much of Yellowstone will be closed for months. “We can no longer talk about this as a future tense, that this is what’s going to happen and this is what climate change is going to do for flooding in Montana,” Shepherd, the meteorologist, told me. “It’s here.” from https://ift.tt/UMgzR8J Check out http://natthash.tumblr.com In late summer 2021, during the Delta wave of the coronavirus pandemic, the American Academy of Physical Medicine and Rehabilitation issued a disturbing wake-up call: According to its calculations, more than 11 million Americans were already experiencing long COVID. The academy’s dashboard has been updated daily ever since, and now pegs that number at 25 million. Even this may be a major undercount. The dashboard calculation assumes that 30 percent of COVID patients will develop lasting symptoms, then applies that rate to the 85 million confirmed cases on the books. Many infections are not reported, though, and blood antibody tests suggest that 187 million Americans had gotten the virus by February 2022. (Many more have been infected since.) If the same proportion of chronic illness holds, the country should now have at least 56 million long-COVID patients. That’s one for every six Americans. So much about long COVID remains mysterious: The condition is hard to study, difficult to predict, and variously defined to include a disorienting range and severity of symptoms. But the numbers above imply ubiquity—a new plait in the fabric of society. As many as 50 million Americans are lactose intolerant. A similar number have acne, allergies, hearing loss, or chronic pain. Think of all the people you know personally who experience one of these conditions. Now consider what it would mean for a similar number to have long COVID: Instead of having blemishes, a runny nose, or soy milk in the fridge, they might have difficulty breathing, overwhelming fatigue, or deadly blood clots. Even if that 30 percent estimate is too high—even if the true rate at which people develop post-acute symptoms were more like 10 or 5 or even 2 percent, as other research suggests—the total number of patients would still be staggering, many millions nationwide. As experts and advocates have observed, the emergence of long COVID would best be understood as a “mass disabling event” of historic proportions, with the health-care system struggling to absorb an influx of infirmity, and economic growth blunted for years to come. Indeed, if—as these numbers suggest—one in six Americans already has long COVID, then a tidal wave of suffering should be crashing down at this very moment, all around us. Yet while we know a lot about COVID’s lasting toll on individuals, through clearly documented accounts of its life-altering effects, the aggregate damage from this wave of chronic illness across the population remains largely unseen. Why is that? A natural place to look for a mass disabling event would be in official disability claims—the applications made to the federal government in hopes of getting financial support and access to health insurance. Have those gone up in the age of long COVID? In 2010, field offices for the Social Security Administration received close to 3 million applications for disability assistance. The number dropped off at a steady rate in the years that followed, as the population of working-age adults declined and the economy improved after the Great Recession, down to just about 2 million in 2019. Then came COVID. In 2020 and 2021, one-third of all Americans became infected with SARS-CoV-2, and a significant portion of those people developed chronic symptoms. Yet the number of applications for disability benefits did not increase. In fact, since the start of the pandemic, disability claims have dropped by 10 percent overall, a rate of decline that matches up almost exactly with the one present throughout the 2010s. “You see absolutely no reaction at all to the COVID crisis,” Nicole Maestas, an associate professor of health-care policy at Harvard, told me. She and other economists have been looking for signs of the pandemic’s effect on disability applications. At first, they expected to see an abrupt U-turn in the number of applications after the economy buckled in March 2020—just as had happened in the aftermath of prior recessions—and then perhaps a slower, continuous rise as the toll of long COVID became apparent. But so far, the data haven’t borne this out. That doesn’t mean that the mass disabling event never happened. Social Security field offices were closed for two years, from March 17, 2020, to April 7, 2022; as a result, all applications for disability benefits had to be done online or by phone. That alone could explain why some claims haven’t yet been filed, Maestas told me. When field offices close, potential applicants have less support available to help them complete paperwork, and some give up. Even now, with many federal offices having reopened, long-haulers may be struggling more than other applicants to navigate a bureaucratic process that lasts months. Long COVID has little historical precedent and no diagnostic test, yet patients must build up enough medical documentation to prove that they are likely to remain impaired for at least a year. [Read: The pandemic after the pandemic] In light of all these challenges, federal disability claims could end up as a lagging indicator of long COVID’s toll, in the same way that COVID hospitalizations and deaths show up only weeks after infections surge. Yet the numbers we have so far don’t really fit that explanation. The Social Security Administration told me last week that the federal government had received a total of 28,800 disability claims since the start of the pandemic that make any mention whatsoever of the applicant having been sick with COVID. This amounts to just 1 percent of the applications received during that time, by the government’s calculation, and would represent an even tinier sliver of the total number of long-COVID cases estimated overall. When I passed along this information to Maestas, she seemed at a loss for words. After a pause, she said: “It’s just not a mass disabling event from that perspective.” The National Health Interview Survey provides another perspective, though the population effects of long COVID are no easier to find in those data. The survey, performed annually by the federal government, measures disability rates among Americans by asking whether they have, at minimum, “a lot of difficulty” completing any of a set of basic tasks, which include concentrating, remembering, walking, and climbing stairs. The proportion of people who reported such difficulties was flat through 2021: 9.6 percent of adults were disabled in December 2019, as compared with 9.5 percent two years later. 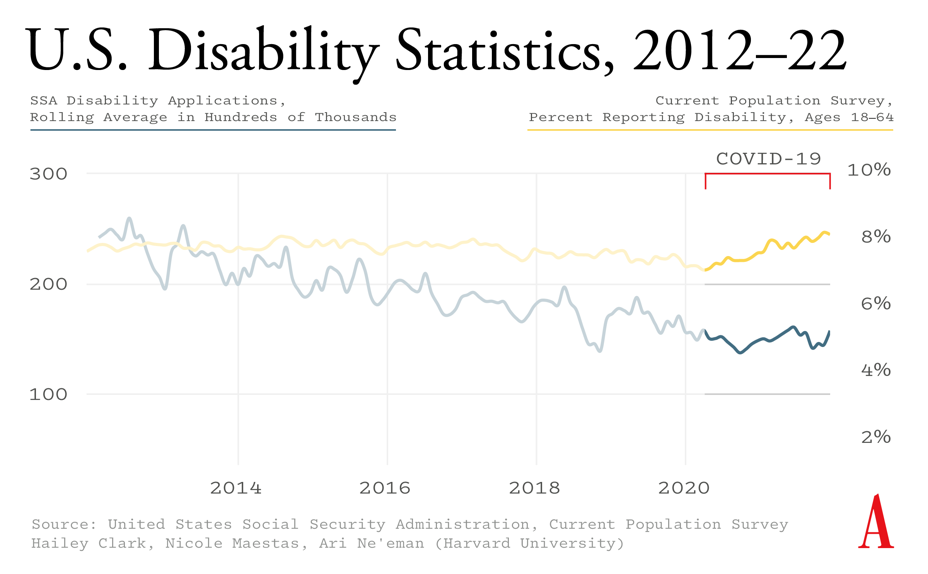
Other sources of disability data do hint—but only hint—at long COVID’s consequences. When the U.S. Bureau of Labor Statistics performs its monthly employment survey, it asks Americans a few basic questions about their physical and cognitive health, including whether they have difficulties concentrating, making decisions, walking, or running errands. By this measure, the number of people reporting such problems began to nudge upward by the middle of 2021. (Disability rates briefly appeared to decline at the start of the pandemic, when in-person interviewing went on hold.) But this increase, from about 7.5 to 8 percent of the working-age population, represents a tiny blip compared with the extrapolated number of Americans who have long COVID, and most of this new cohort is still able to work. Maestas suspects that these particular disability numbers represent the first sign of a true upswing. “As you watch them keep going up each quarter, it’s starting to look like maybe there is something going on,” she said. The survey measures described above may be affected slightly by the pandemic’s disproportionate death toll among already disabled people. They could also only ever tell one part of the story. At best, they’ll capture a certain kind of long COVID—the sort that leads to brain fog, fatigue, and weakness, among other severe impairments in memory, concentration, and mobility. One of the overarching problems here is that long COVID has been associated with many other ailments, too, such as internal tremors, sudden heart palpitations, and severe allergic reactions. None of these issues is likely to show up in the NHIS or BLS data, let alone qualify someone for long-term financial support from the Social Security Administration. If the “mass disabling event” plays out as tens of millions of cases of shooting nerve pain or diarrhea, for example, or even just a persistent loss of smell, then you might never see a large jump in the number of Americans who report having difficulty functioning. In that case, though, more Americans might end up seeking out their doctors for evaluations, tests, and treatments. A growing number of symptoms, overall, should lead to a growing burden, overall, on the country’s health-care system. The available data suggest that the opposite is true, at least for now. A report from Kaiser Family Foundation, released last fall, found that both outpatient and inpatient health-care spending was actually lower than projected through the first half of 2021—even accounting for millions of acutely ill COVID patients. “We have not seen pent-up demand from delayed or forgone care,” the nonprofit wrote. (This modest spending was recorded despite the fact that the proportion of Americans with health insurance increased during the first two years of the pandemic.) In February, the consulting firm McKinsey surveyed leaders from 101 hospitals around the country, who said that outpatient visits and surgeries were still below pre-pandemic levels. The pandemic’s effect on health-care workers must be contributing to this decline in volume, but it can’t account for all of it. Most patients can still snag a specialist appointment within two or three weeks, according to McKinsey’s data. It’s possible that many long-haulers have simply given up on getting medical care, because they’ve understandably concluded that treatments don’t exist or that doctors won’t believe they're sick. (The scarcity of clinics dedicated to patients with long COVID could also be a problem.) The U.K.’s Office for National Statistics has been performing one of the world’s largest long-COVID surveys, in an effort to measure the full extent of this behind-the-scenes suffering. The study shows that, as of the beginning of May, 3 percent of that country’s residents identify as having long COVID, broadly defined as “still experiencing [any] symptoms” more than four weeks after first getting sick. (Eighty percent of the U.K. population is estimated to have been infected with the coronavirus at least once.) About two-thirds of this group—amounting to more than 1 million people—say that the condition affects their ability to perform day-to-day activities. Among the survey’s most-cited chronic symptoms are weakness, shortness of breath, difficulty concentrating, muscle aches, and headaches. [Read: Being Black and disabled is a constant struggle] In its focus on persistent symptoms, the U.K. survey may be leaving out other, more insidious consequences of COVID. A CDC analysis, published last month, examined the medical records from hundreds of thousands of adult COVID patients, and concluded that at least one in five might experience post-illness complications. Some of these were of the familiar types (trouble breathing, muscle pain); others were of the ticking-time-bomb variety, including blood clots, kidney failure, and heart attacks. This study’s methods have been harshly criticized—people who have long COVID “deserve better, much better,” Walid Gellad, a professor of medicine at the University of Pittsburgh, told me—and the one-in-five statistic could be way too high. But if the CDC’s results are correct in substance—if various mortal dangers do increase by a significant degree after COVID—then the effects of these should also be detectable at the population level. Comparisons between individual study results and overall disease burden offer a reality check for extreme findings, Jason Abaluck, an economist and a health-policy expert at Yale, told me. “They allow you to put bounds on things.” Where does that leave us with long COVID? The majority of Americans have already encountered the virus, many more than once. The CDC suggests that these people will, on average, experience about a 50 percent increase in their respective risks of blood clots, kidney failure, and heart attacks, as well as diabetes and asthma. Comprehensive national disease estimates will take years to compile, but provisional rates of death from heart disease, stroke, and kidney disease haven’t really budged since 2019, and the NHIS survey has shown no increase in the number of Americans with high blood pressure or asthma. In short, here’s what we can say right now: Disability rates might be rising, but only by a little bit; the health-care system seems to be coping; deaths from post-COVID complications aren’t mounting; and the labor force is holding up. If the fact that a million Americans died of COVID skews the numbers, that’s not a factor. Long COVID, in other words, isn’t yet standing out amid the pandemic’s other social upheavals. Liza Fisher has long COVID, and she shows up in the data. The 38-year-old former flight attendant and yoga instructor from Houston became ill with COVID in June 2020. Her infection led to months of hospitalizations, procedures, and rehabilitation. She now requires a team of medical specialists, and she remains severely limited in her daily activities because of neurological symptoms, fatigue, and allergic reactions. Fisher went on medical leave from work after her symptoms began, and she never returned. In December 2020, she applied for disability benefits from the Social Security Administration, and was granted them about six months later. “Government numbers aren’t accurate, and may never be accurate,” Fisher told me. She knows of long-haulers who have applied for disability programs under better-established diagnoses, for instance, because they believed that citing long COVID wouldn’t grant them access. And she saidys that when national metrics don’t reflect the everyday reality of the long-COVID community, advocating for research, treatment, and support services becomes more difficult. [Read: The promising treatment for long COVID we’re not even trying] Frank Ziegler also has long COVID, but he hasn’t quit his job, nor has he put in a claim for any benefits. A 58-year-old lawyer from Nashville, Tennessee, Ziegler developed a mild case of COVID in January 2021. The nasal congestion he experienced was so unremarkable that he assumed at first he had a simple sinus infection. But in the course of his recovery, something about Ziegler’s appetite changed—seemingly for good. Foods he had previously loved became strangely unappetizing; he lost a significant amount of weight. Then he started noticing hand tremors, trouble breathing, and cognitive issues. A battery of medical tests came back essentially normal, but Ziegler still doesn’t feel as well as he did before catching the virus. His life has changed , but that difference might not be reflected on any government graph. “The square pegs of long-COVID patients are never going to fit into the round holes of conventional testing,” he told me. The mix of symptoms and experiences that define long COVID suggests that no single measure, or group of measures, can illustrate the suffering of long-haulers in aggregate. A “mass disabling event” is not playing out in the data we have. That could change in the months and years to come, or else it might indicate that we’re in another kind of moment, one that leaves tens of millions of Americans feeling somewhat worse off than they were before, not so sick that they can’t hold down a job or need medical attention, but also not quite back to baseline. Call it a “mass deterioration event.” “There are a significant number of people that can’t simply move on,” Ziegler told me. “Many of them have no idea why they are feeling the way they do, and they have not been able to get any relief.” That form of epidemic—one that degrades quality of life, incrementally, for millions—is likely unfolding, even as a much smaller group of patients, including Fisher, see their lives utterly transformed by chronic illness. We don’t know how bad the long-COVID crisis will get, but for many, there’s no turning back. from https://ift.tt/fWOYwb7 Check out http://natthash.tumblr.com In the past three years, the world has weathered two very different global outbreaks, caused by two very different pathogens, under two sets of very different circumstances. Unlike with the SARS-CoV-2 virus, with monkeypox, we’re entering an epidemic with highly effective vaccines—formulated to guard against smallpox—already in hand. Also unlike with SARS-CoV-2, with monkeypox, the shots stockpiled in U.S. stores are based on some pretty grody tech. Nearly all of the 100 million available smallpox vaccines are ACAM2000, an inoculation that, per FDA documentation, gets punctured “rapidly” into the arm via 15 jabs of a bifurcated, escargot-fork-esque needle, in a fashion “vigorous enough” to draw blood. In the weeks following, a gnarly, pus-laden lump blossoms, then scabs and falls away. “It’s oozy; it’s nasty; it definitely doesn’t feel good,” says Kelsey Cone, a virologist at ARUP Laboratories, in Utah, who received the vaccine about 12 years ago. And unlike with SARS-CoV-2, with monkeypox, most of us won’t have to get those shots—or any smallpox vaccine at all, at least not anytime soon. “Vaccination is not going to be the primary thing that squashes this outbreak,” says Boghuma Kabisen Titanji, a virologist and an infectious-disease physician at Emory University. Monkeypox is an older pathogen than the new coronavirus, with a richer history with humans; it spreads far less efficiently, and can more easily be snuffed out. And it will demand an almost opposite response—one that doesn’t require building widespread population immunity. Monkeypox, after all, is a different sort of emergency, in which the downsides of mass vaccination—for now—outweigh the perks. Our most abundant shot, ACAM2000, contains an active virus, related to smallpox, that can replicate inside human cells; “if you vaccinated a million people, you might result in more disease,” says Mark Slifka, a vaccinologist at Oregon Health & Science University, “than you would get from the monkeypox outbreak itself.” [Read: So, have you heard about monkeypox?] If vaccinating everyone is off the table, that leaves us with blocking the outbreak upstream—with testing, education, and behavioral change, the exact tactics the U.S. has proved itself, time and time again, incapable of sustaining. As the world attempts to juggle two pathogens at once, we may find that monkeypox is, in some ways, an advanced version of a test we’ve taken before, and very recently flunked. All that said, some of us will be nabbing smallpox shots, and sporting the subsequent scabs. Already, several countries in Europe and North America have kick-started what are called ring-vaccination campaigns—offering smallpox shots to close contacts of infected people. When supply is limited, this sort of targeted tactic “gives you the most bang for your buck,” Slifka told me, especially when a pathogen seems to be circulating in rather specific sectors of the population. A disproportionate fraction of the 1,600-plus monkeypox cases identified so far, across 35 countries, have been men who have sex with men, who likely caught the infection through intimate contact; health-care workers on the front lines of the outbreak, too, are being offered shots. Some jurisdictions are casting wider nets. Officials in Montreal, for instance, have started giving vaccines to men who have had at least two male sex partners in the past couple of weeks. These tactics are a far cry from mass immunization—which demands an abundantly clear risk-benefit calculus. The shots for SARS-CoV-2 (and many other microbes in our past and present) have that: The virus spreads swiftly and often asymptomatically, and has killed millions around the world. It is difficult to control through most other means. And the vaccines scientists have cooked up to fight it are effective and supersafe. Monkeypox, however, is “nothing like” its coronaviral colleague, says Cone, who used to work with the poxvirus. Unlike airborne SARS-CoV-2, monkeypox passes between people mostly via sustained close contact, and seems to transmit “only during the symptomatic phase,” says Dimie Ogoina, a physician at Niger Delta University who has studied monkeypox. Amid the current outbreak, most cases detected outside West and Central Africa—where monkeypox is endemic, and not particularly concentrated among men who have sex with men—have been relatively mild. [Read: We should have seen monkeypox coming] And the vaccines available to combat monkeypox have real drawbacks that many other shots do not. Because ACAM2000 contains an active virus, it may be especially risky for infants or people who are pregnant, immunocompromised, or living with HIV. The shot also comes with a small but notable risk of heart inflammation, or myocarditis, and its documentation warns of other serious side effects, including blindness, spreading the vaccine virus to others, and even death. (Still, the jab is a big improvement over its direct predecessor, Dryvax—an inoculation that many Americans over the age of 50 have—which Slifka describes as pus “ladled out of a cow.”) “You would really have to make a compelling argument,” Titanji told me, “to convince me to use ACAM as the primary tool.” A newer alternative, known as MVA (or Jynneos in the United States), built around a weaker version of the vaccine virus, is much safer. But the globe’s MVA stock is low, with most refills months away, and the vaccine has yet to be approved in Europe for use against monkeypox. Experts also lack solid intel on just how well both ACAM2000 and MVA actually work against monkeypox, because the virus—and the vaccinations that fight it—remains rare for most of the world. Even ring vaccination has its limits. The strategy works best when cases can be rapidly identified, and close contacts, speedily traced, are enthusiastic about receiving the shots. Right now, monkeypox cases are not being detected and isolated quickly enough; infected people are likely still mingling with others who aren’t immune. The disease’s symptoms also have not been consistently manifesting as monkeypox’s normally telltale unfurling from fever and swollen lymph nodes to rashes and lesions. Stigma, too, has shrouded the infection, hurting efforts to halt it. And vaccines have been declined by some of the people at risk of exposure—even by health-care workers. With vaccines cut from the headlining slot, our roster of remaining tools might be looking a touch meager. Already, the global response to the epidemic has been hamstrung by a lack of testing capacity and a sluggish behavioral response—one that experts worry is being further bogged down by understandable exhaustion after two-plus years of COVID, COVID, COVID. That inertia, if it continues, will likely cost us. This outbreak marks the first time that monkeypox has spread so steadfastly outside the regions of Africa where it’s typically found, and the virus has been slingshotting all sorts of surprises our way. “The pathogen is not new, but the way that it’s moving is new, and the way it’s presenting on people’s bodies is new,” says Keletso Makofane, a researcher at Harvard’s School of Public Health. Experts are still scrambling to get a firmer grip on the disease’s symptoms, which can be easy to confuse with those of STIs, and their severity. Some of them, including Makofane, are also working to scale up diagnostics, and map the networks that have allowed the poxvirus to spread. That knowledge will hopefully bolster efforts to root out cases and close contacts, get them into isolation and quarantine, and vaccinate the (for now) limited number of vulnerable people. The success of those strategies depends, as it has with COVID, on collective action, flexibility, and trust. “Communication with the public is crucially important,” Makofane told me, especially in ways that won’t fuel discrimination or shame. People unfamiliar with the pathogen will need to grow savvy to its symptoms and ways of spreading; they’ll need clear pathways to care. Having behavioral advice at the ready could also boost efforts to dole out shots, not least because it’ll reduce the number of people who might need them. [Read: Monkeypox could be nothing—or it could be the next syphilis] But “people don’t like making changes to their behaviors,” says Saskia Popescu, an infection-prevention expert at George Mason University. They want one-stop solutions, which most microbes do not lend themselves to. But lean too heavily on shots right now—or worse, give the false impression that they’re the most important intervention here—and the world could fall into some of the same traps of “vaccine absolutism” that have dogged the COVID-19 discourse, Popescu warned. “I worry we’re so vaccine-focused that we’re going to repeat our [COVID] failures,” she told me, and let other measures fall to the wayside as public disillusionment grows. Should the outbreak continue to balloon, so will vaccination’s role. If the virus keeps spreading and moving into new networks, a wider immunization campaign could become more pressing. Though most of this monkeypox outbreak hasn’t been severe, since the start of 2022, the virus has killed more than 70 people in West and Central Africa in 2022. And should the pathogen expand its domain, or seed itself into an animal reservoir, there’s no telling what it will bring next. The pathogen could happen upon mutations that help it spread faster, or cause more severe disease. “That’s my biggest concern,” says Rafi Ahmed, an immunologist at Emory University. “We’ve never seen deaths in high-income settings,” says Anne Rimoin, an epidemiologist and a monkeypox expert at UCLA. “But that doesn’t mean we won’t.” Unlike with SARS-CoV-2, with monkeypox, a near-best-case scenario is one in which smallpox vaccination rates remain rather low—because, having found other ways to halt the virus’s roll, we do not need them to rise. from https://ift.tt/ETNUlBx Check out http://natthash.tumblr.com In early May, 27-year-old Hayley Furmaniuk felt tired and a bit congested, but after rapid-testing negative for the coronavirus two days in a row, she dined indoors with friends. The next morning, her symptoms worsened. Knowing her parents were driving in for Mother’s Day, she tested again—and saw a very bright positive. Which meant three not-so-great things: She needed to cancel with her parents; she had likely exposed her friends; a test had apparently taken three days to register what her vaccinated body had already figured out. Tests are not and never have been perfect, but since around the rise of Omicron, the problem of delayed positivity has gained some prominence. In recent months, many people have logged strings of negatives—three, four, even five or more days in a row—early in their COVID-symptom course. “I think it’s become more common,” says Amesh Adalja, an infectious-disease physician at the Johns Hopkins Center for Health Security. [Read: COVID tests weren’t designed for this] No one can yet say how common these early negatives are, or who’s most at risk. But if SARS-CoV-2 is rewriting the early-infection playbook, “that makes it really scary,” says Susan Butler-Wu, a clinical microbiologist at USC’s Keck School of Medicine. “You can’t test and get a negative and actually know you’re negative.” Misleading negatives could hasten the spread of the virus; they could delay treatments premised on a positive test result. They also buck the current COVID dogma: Test as soon as you feel sick. The few days around the start of symptoms are supposed to be when the virus inside you is most detectable and transmissible; we built an entire edifice of testing and isolation on that foundation. Experts aren’t sure why delayed positives are happening; it’s likely that population immunity, viral mutations, and human behavior all have some role. Regardless, the virus is “acting differently from a symptom perspective for sure,” says Emily Martin, an infectious-disease epidemiologist at the University of Michigan. That’s worth paying attention to. The start of symptoms has always been a bit of a two-step: Is it COVID, or not? If SARS-CoV-2 is re-choreographing its moves, we must too—or risk losing our footing. Right now, experts are operating in a vacuum of evidence: “I don’t even know of any data that systematically evaluates this,” says Yonatan Grad, who’s studying the viral dynamics of SARS-CoV-2 at Harvard’s School of Public Health. But several phenomena could plausibly be muddying the testing timeline. First, the immunity hypothesis, the most popular idea floated by the experts I spoke with. Perhaps symptoms are preceding test positivity, less because the virus is peaking late, and more because illness is arriving early, thanks to the lightning-fast reflexes of people’s primed immune systems. Sometimes, sickness is direct damage from a virus. But a runny nose, muscle and joint aches, chills, fevers, fatigue—which are common across many respiratory infections—can also be “signs that the immune system is being activated,” says Aubree Gordon, an infectious-disease epidemiologist at the University of Michigan. When the pandemic began, infections happened exclusively in people who’d never encountered the coronavirus before; illness took several days to manifest, as the virus churned itself into a frenzy and the immune system struggled to catch up. “Once people are vaccinated, though, their immune systems kick in right away,” says Emily Landon, an infectious-disease physician at the University of Chicago. (Prior infection, too, could have an impact.) If the body makes fast work of the invader, some people may never end up testing positive, especially on antigen tests. (PCRs are generally more sensitive.) Others may see positives a few days after symptoms start, as the virus briefly gains a foothold. But some of the experts I spoke with were a little hesitant to give the immune system all the credit. Some unimmunized people have experienced early negativity, too, and many people who have gotten their shots still test positive before falling ill. SARS-CoV-2 traits, too, could be flipping the sickness script, which brings us to the virus hypothesis. Any member of the Omicron cohort is “just a different beast,” says Ryan McNamara, a virologist at Massachusetts General Hospital. It struggles to penetrate deep into the lower airway, and may not accumulate to the densities that Delta did in the nose, which could make false negatives more likely. A couple of studies have also found that Omicron may, in some people, be detected in the mouth or throat before the nostrils. In practice, “it’s really hard to separate if all of this is a property of the virus, or a property of the immune system, or both,” says Roby Bhattacharyya, an infectious-disease physician at Massachusetts General Hospital. Take Omicron’s symptom profile, for instance. This variant seems to more often prompt sneezier, head-cold-esque symptoms than those that came before it, and less often causes loss of taste and smell. And, on average, people infected in recent surges have been showing symptoms three days after exposure, far faster than the incubation period of five or six days that was the norm in the pandemic’s early days. But those patterns could be attributable to either the peculiarities of the Omicron clan, or how much more immune the average Omicron host is. [Read: Next winter, what if we test for even more viruses?] And testing and sickness severity involve “just so many variables,” says Ali Ellebedy, an immunologist at Washington University in St. Louis, similar to the diversity in reactions to vaccines—some people feel side effects, others don’t—or virus exposures. Some people never get infected, even after spending days with infectious people, while others seem ultra-susceptible. People’s vaccination status, age, genetics, even the dose of virus, can affect if, when, or how they feel ill, and whether their infection registers on a test. Symptoms and test accuracy are also both subject to human bias. People can’t always remember when they started feeling sick. And user error can muddle diagnostics. “Are people really doing 15 seconds in each nostril, and really scrubbing each time?” Landon said. Even super-sensitive tests will miss the virus some of the time. A good portion of the specimens taken from sick people in medical settings “come back negative for everything,” Martin told me. Coinfections are also possible: People who feel sick and test positive “late” may have actually caught something else first, only to develop COVID later on. “There are easily five to eight other viruses circulating right now,” says Melissa Miller, a clinical microbiologist at the University of North Carolina at Chapel Hill. It’s also allergy season in much of the U.S. And coronavirus tests can spit out false positives—though they’re unlikely to do so several days in a row. Without more data, it’s hard to know how to best address early negatives. For more clarity, “you’d probably need a human challenge experiment,” in which vaccinated and unvaccinated volunteers are deliberately infected with SARS-CoV-2, then repeatedly tested and monitored for symptoms over time, Gordon said. But based on the stories emerging, the issue doesn’t really seem rare. “I think I’ve had maybe 20 friends in the last five weeks” catch the virus, Jesse Chen, a vaccinated 27-year-old in New York, told me; most of them experienced delayed positivity, including Chen herself. If this is happening more, then “you cannot trust a negative rapid test at the beginning of illness,” Landon told me. And while the CDC and test makers have long said that negative results can’t rule out a SARS-CoV-2 infection, it’s not clear how these early-illness testing issues fit into diagnostic guidance. Kimberly Modory, a spokesperson for Abbott, which makes the widely used BinaxNOW SARS-CoV-2 test, wrote in an email that “people should continue to follow our test instructions, which is to test twice over 3 days, at least 24 hours (and no more than 48 hours) apart.” Another popular brand, iHealth, offers similar instructions. (CDC and iHealth did not respond to a request for comment.) Many of these protocols, though, were developed when far fewer people had been vaccinated or infected, and Omicron and its offshoots weren’t yet dominant. And they have missed some recent infections. Furmaniuk, for instance, green-lit herself for dinner with two iHealth tests. And Ellen Krakow, a triply-vaccinated 58-year-old from Long Island, didn’t get a positive antigen result until she took her third BinaxNOW, on her fourth day of symptoms. (A PCR test, collected on her third day, did turn positive first.) Until experts know more, several researchers recommended that people test with caution. Positives are still reliable, Landon told me. But people who are symptomatic and recently exposed might have good reason to be skeptical of negatives. “If you’re turning symptomatic, assume you’re infectious,” Grad told me—with something, even if it turns out not to be SARS-CoV-2. “People forget that, baked into all the recommendations, is that as soon as you turn symptomatic, you’re supposed to be behaving differently,” Martin told me. “A negative test shouldn’t be a pass to go out.” Landon also raised concerns about the implications of early negatives for the duration of isolation. In January, the CDC cut recommended COVID isolation time in half, saying that people could stop sequestering themselves after just five days, counting out from when their symptoms started, as long as they masked for the five days following. The agency justified its decision by noting that a majority of people were no longer infectious by that point—but used data that almost entirely predated the Omicron surge. [Read: America’s COVID rules are a dumpster fire] Based on the evidence that’s emerged since, “five days is ridiculous optimism,” said Landon, who recently ran a study showing that a large fraction of people continue to test positive after their fifth isolation day, raising the possibility that they’re still shedding the virus in gobs. Rebecca Ennen, a vaccinated 39-year-old in D.C., didn’t even get her first positive result until Day Six of her illness, as her symptoms were on their way out. “It was just bizarre,” she told me. “I was on the mend.” So Ennen continued cloistering for another five days, until she finally tested negative again. Others, including Gordon and Furmaniuk, have also waited to test out of isolation; it’s what Bhattacharyya “would do too, if it were me.” But such a mindset hardly seems sustainable, especially for people who are frequently exposed to respiratory microbes, including parents of very young kids, or who have bad allergies, or who don’t have rapid tests to spare. Isolation still takes people away from work (and income), school, and their families. It’s also emotionally harrowing. Krakow, of Long Island, didn’t test negative again until 14 days into her illness. “I was isolating for beyond two weeks,” she told me. All of this means that our guidelines and perceptions of the virus may soon need to adjust—likely not for the last time. Butler-Wu, the USC clinical microbiologist, recently advised a friend who had received more than half a dozen negative test results—antigen and PCR—that her respiratory illness probably wasn’t COVID. The friend ended up visiting Butler-Wu, only to test positive shortly thereafter. “That really shook me,” Butler-Wu told me. “It flew in the face of everything I knew from before.” It was a reminder, she said, that the pandemic is still serving up plot twists. “I do this professionally,” she said, “and I still made the wrong call.” from https://ift.tt/OJlUuAz Check out http://natthash.tumblr.com The first reports of monkeypox cases in Europe began to surface in mid-May. A week later, there were 92 confirmed cases outside the Central and West African countries where the disease usually circulates; now there are 1,200. By the end of this month, who knows? “If you’d asked me two weeks ago, I would have anticipated that there might be a few thousand cases globally related to this current outbreak” before it ended, Jay Varma, a population-health professor at Weill Cornell Medical College, told me. “But I’ve become much more pessimistic.” Where, exactly, is the outbreak headed? When I asked five experts for their predictions, they would say only one thing for certain: Monkeypox is not the next COVID-19. It’s simply not transmissible enough to cause infections on the scale of the pandemic, nor does it seem to be a particularly deadly virus. (None of the 1,200 patients has died so far.) But beyond that, their views ranged widely: The outbreak may be over before we know it; or it might become a modest, intermittent problem; or it could transform into an ever-present risk and inconvenience, like the next genital herpes. Here are three possible paths monkeypox could take. The Rosy Scenario: A Quick Fizzle This is not the first time monkeypox has entered the United States. At least 47 people in six states fell ill from the virus in 2003 after interacting with infected pet prairie dogs (legal to own in most states!). The spread was contained within a couple of months, and nobody died; two people got seriously sick, but they recovered. [Read: We should have seen monkeypox coming] This time around, prairie dogs are not involved. Most, if not all, of this year’s monkeypox cases in the U.S. appear to have resulted from person-to-person contact. That makes the public-health response more complicated than euthanizing potentially infected animals, as officials did in 2003. We might still quash the spread quickly through immunization, Amesh Adalja, a senior scholar at the Johns Hopkins Center for Health Security, told me. After all, the U.S. has a stockpile of smallpox vaccines on hand that would also work against this outbreak. (The exact size of the stockpile remains unclear.) “Monkeypox is a containable virus,” he told me. The 2003 outbreak was brought to heel, in part, through a tactic called ring vaccination, in which the close contacts of an infected patient are all inoculated. This works because contact tracing for monkeypox is relatively easy thanks to the physical proximity necessary for its transmission, and because vaccinating someone who has recently been infected can keep them from becoming contagious. Adalja predicts that ring vaccination will likely outpace the spread of monkeypox in the U.S. in a matter of weeks, and that cases will fall to zero within about three months. The Medium Scenario: A Sporadic Problem Monkeypox already breaks out from time to time in Central and West Africa. Experts say that’s because the virus is endemic in local animal populations, probably some kind of mammal. The same could happen here in the U.S.: If enough American wildlife get infected through interactions with infected humans, then monkeypox could circulate in silence after human cases drop to zero. Every so often, an animal would infect a person, that person would spread the virus to some close contacts, and another minor outbreak would form, then fizzle out. Repeat indefinitely. Bhargavi Rao, who worked in the Democratic Republic of Congo and the Central African Republic as the head of emerging and infectious diseases at Doctors Without Borders, told me that a spate of monkeypox infections is “not the sort of thing that overwhelms a community.” She said she thinks the risk of monkeypox becoming endemic in animals outside Central and West Africa is “very low,” but if it did, its effects would be akin to those of modern anthrax, rabies, or bird flu; that is, it might cause occasional disruption and lead to occasional culling of animals, but it wouldn’t generally affect daily life. (James Diaz, the director of environmental and occupational health at Louisiana State University, told me that he suspects monkeypox might already be endemic in American wildlife—but also that there’s no hard evidence to support this claim.) The fact that many recent cases have been recorded in and around big cities could lead to different outcomes, though. In the countries where Rao worked, the disease mostly jumps from wildlife to farmers and bush hunters who live in isolated communities. She said there’s no way of knowing how big an outbreak might get in an American metropolis, even as those at risk would generally have better access to testing and vaccines. If the outbreak were big enough, the virus might become endemic in rodent populations, causing further urban outbreaks down the line. “When it’s in the rats, there’s nothing you can do,” Adalja told me. The Bad Scenario: Another Syphilis We’ll be dealing with something entirely different if the current outbreak can’t be stopped. Both Rao and Adalja said such an outcome seems unlikely because monkeypox patients are generally not infectious before they’re symptomatic, and the world already has tests, vaccines, and treatments for the virus. But the conventional wisdom about monkeypox might not hold for this outbreak. Varma, who helped lead New York City’s response to COVID, is much more worried than the other experts I spoke with. “I would say it’s less than 50 percent probability that we will contain this,” he said. That’s not to say that one-third of the country is likely to come down with monkeypox in the next six months. Varma predicts that monkeypox will continue to circulate at low levels and stay concentrated in the community of men who have sex with men. (To be clear, monkeypox is not a sexually transmitted infection. The CDC has said that “a high number” of cases so far have involved men who have sex with men, but the disease can be spread through sexual or nonsexual contact between anyone.) If that’s what happens, then monkeypox would be similar to syphilis, Varma said, which affects about 0.04 percent of Americans, most of them men who have sex with men. In Varma’s absolute worst-case scenario—which he thinks is less likely—monkeypox could spread through all sorts of communities, including children and pregnant women, and become as common as genital herpes, with more than 12 percent of Americans infected. Jim Downs[: Gay men need a specific warning about monkeypox] Again, this would not spell civilizational collapse. Very few people who contract monkeypox die from it or get seriously sick. Even if monkeypox did become widespread among the American population, Adalja told me, routine vaccination could eliminate much of the associated risks to people’s health. But the more people who get sick, the greater the likelihood that someone will experience a rare and serious complication. Population-scale vaccination, too, could have some downsides. We also don’t know how the disease will change. DNA viruses, including monkeypox, are generally stable, and evolve into new strains slowly. But “it’s never a good thing to let a zoonotic virus spread unchecked in humans,” Boghuma Titanji, an infectious-disease specialist at Emory University, told me. “The reality is you do not know what the adaptation of that virus in a new host will do.” It could become more or less transmissible, more or less capable of causing serious disease and death. Or it could stay pretty much the same. No one will be able to accurately forecast the future of this outbreak until we’re certain of the present. And we’re just not there yet. The virus’s incubation period averages one to two weeks, but can stretch as long as three, which means the cases we’re seeing now reflect the spread of the virus many days ago. We’re also not testing enough to keep track of the outbreak, Titanji told me. Testing is especially important because cases in the current outbreak look so different from classical monkeypox. Historically, monkeypox lesions developed around the tongue and mouth first, followed by a rash on the face, arms, and legs, which progressed into lesions; those symptoms were easy to see. The recent outbreak, however, has included many patients who have only a handful of lesions, concentrated around their genitalia and anus. In the past, U.S. cases of monkeypox were travel-related, and people who fell ill showed up to travel clinics or told their doctor they’d been out of the country; now patients might show up at sexual-health clinics to investigate the scabs on their private parts. The more accessible testing is, the easier it will be for patients to be identified and advised to isolate, while vaccines are provided to their contacts. “The sooner you can get a lab-confirmed infection, the sooner people take it seriously,” Varma said. For now, we still don’t know how many people around the country are infected, nor how many others will eventually get sick. When I asked Titanji how and when we’ll know which path we’re on, she said it’s difficult to tell, and not worth guessing. “Every time a virus crosses species and gets into a new species, and it’s transmitting itself and causing outbreaks, you are in a gray zone.” from https://ift.tt/cexinKq Check out http://natthash.tumblr.com |
Authorhttp://natthash.tumblr.com Archives
April 2023
Categories |
 RSS Feed
RSS Feed

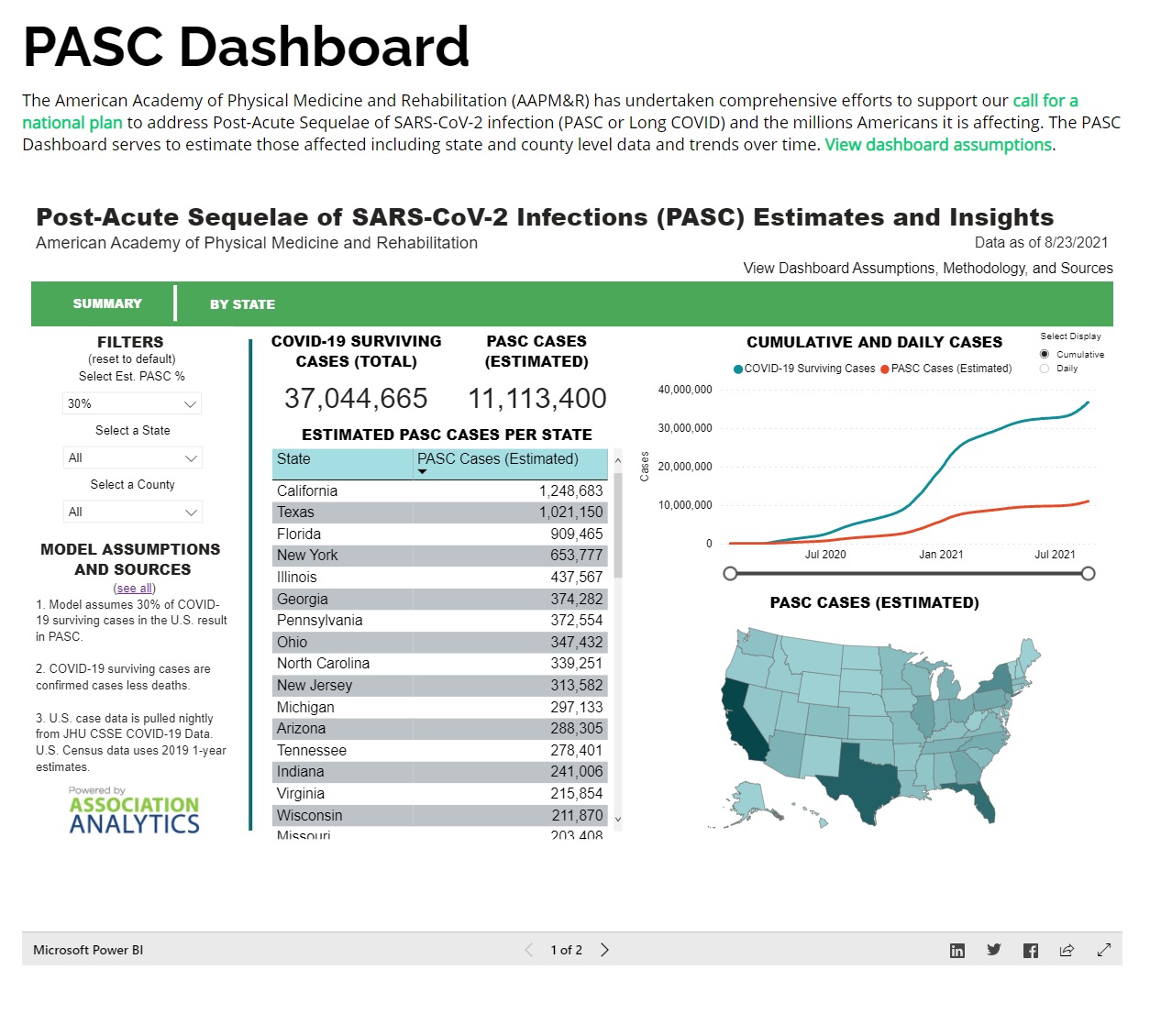{kind=link}