|
Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. Yesterday, hospitalizations in the United States fell below 60,000 for the first time since November 9, according to data from the COVID Tracking Project at The Atlantic. This milestone is not just another round number. In the spring and summer waves, hospitalizations peaked at just fewer than 60,000 both times. In other words, for the first time in three months, the spread of COVID-19 has receded enough that it now matches the worst of the early pandemic. As welcome as this change might be—it’s a relatively rapid decline from the peak of 132,474 hospitalizations on January 6—it also indicates how far we have to go. During the winter surge, every U.S. region hit a peak almost simultaneously, whereas the spring and summer peaks represented increases in just two regions. The decline has been rapid for similar reasons: It’s happening everywhere. By the COVID Tracking Project’s conservative definition of falling, meaning down more than 10 percent from the prior week, hospitalizations in 41 states are falling while those in nine states and the District of Columbia are staying the same. Only hospitalizations in South Dakota are increasing, and in raw numbers it’s from 82 patients to 95. The death toll has finally caught up to this trend as well. On February 18, the seven-day average of deaths was 1,998, the first time that number fell below 2,000 since December 4, and down from 3,302 on January 26. What the next months will bring is unclear. James Hamblin predicts “a quite possibly wonderful summer,” noting a shift to cautious optimism among scientists and researchers who previously hadn’t expected a return to normal until late summer or early fall. Vaccination is one reason; its effects seem to be showing up already in nursing homes. The prevalence of the coronavirus, reflected by the awful numbers of the winter surge, may have also led to “some protective effects of herd immunity,” Hamblin writes—a theory echoed by the epidemiologist Trevor Bedford. The biostatistician Natalie Dean adds that “policy and individual-level behavior change” in response to the surge may have played a role, and evidence in the testing data supports that. The unpredictable prevalence of the more infectious B.1.1.7 variant could slow the pandemic’s decline and push back that wonderful summer if vaccinations don’t continue apace. In the bigger picture, as Hamblin writes, the virus still has a chance to evolve beyond the reach of vaccines, as long as unvaccinated populations can offer the virus a harbor. Truly putting COVID-19 behind us will require solutions that are global in scale. from https://ift.tt/3pG5pfA Check out http://natthash.tumblr.com
0 Comments
Nearly a year ago, Atlantic staff writer Helen Lewis predicted the pandemic would be “a disaster for feminism,” and far too many of her predictions have proven true. With women leaving the workforce at unprecedented rates, why has the pandemic’s burden fallen so much harder on them? And what can we, as a society, do about it? Lewis joins staff writer James Hamblin and comedian Maeve Higgins on the podcast Social Distance. Listen to their conversation here: Subscribe to Social Distance to receive new episodes as soon as they’re published. What follows is a transcript of the episode, edited and condensed for clarity: James Hamblin: Almost a year ago, you made some pretty prescient predictions about how the pandemic would have a different impact on women than men. Helen Lewis: Yeah; I have an unfortunate record in journalism, which is that only my bad predictions come true. Last March, I wrote a piece called “The Coronavirus Is a Disaster for Feminism.” And the reason I said that was that I thought it would be interesting to talk to researchers about the gender dimensions of previous pandemics. And unfortunately, it’s very difficult for women when schools close and the types of jobs that women do are differently affected by pandemic responses. So I made this prediction that for lots of heterosexual couples, at least, there would be a return to the kind of breadwinner/homemaker divide—the 1950s model of what a husband and wife do—simply because men are much more likely to work full time and, in straight couples, more likely to be the higher earner. It makes sense on a couple level if you’re really worried about one of you [losing] your job. And obviously the effects for single parents, the majority of whom are women, are far, far worse. But it’s very obvious that having all of the support that was keeping women in the workforce—grandparents, extended family, and friends—having all of that taken away, as well as schools and child-care nurseries ... It’s just like being repeatedly punched in the face by a giant bear, effectively, for women in this crisis. Maeve Higgins: The numbers are massive in America. 2.4 million women have exited the workforce since you wrote that piece, compared with less than 1.8 million men. Almost one million mothers have left the workforce, with Black mothers, Hispanic mothers, and single mothers among the hardest hit. Lewis: And I think we’re going to see the results of this for years and years. One of the long-term effects will be pension and Social Security contributions. If you’re not working and paying into that system, it can really affect what money you have when you retire. One of the biggest predictors of poverty in older women is getting divorced—because they lose access to their husband’s pension, and they may have had to take a career break themselves. Well, if far more people have had to take a career break or one has [had that] forced on them by being fired, that has effects for the rest of their lives. It’s not just about the fact you’re going to find it quite sketchy the next year or two as you struggle to make ends meet. It’s going to have an impact until you’re dead, essentially. Hamblin: Is it worse than you had imagined? Lewis: It’s a tough question to untangle, because different countries have had very different responses, both in terms of being able to contain coronavirus and the policy response. If your case rates go up to a certain amount, you have to close schools. Britain has been much more reluctant to close schools than America, but nonetheless, they are currently closed now for all except vulnerable children. The U.S. is in this particularly bad situation [in that] it has very little federally funded leave—the employment-rights situation is very low—and it’s got a pandemic that’s been raging absolutely out of control. America is probably one of the worst-hit sets in the world, really—more so than countries which are poorer than America but have managed their pandemics better. Hamblin: [President Joe] Biden has a recovery plan with some proposals to help working families. What do you think would be most important? What’s possible, and what could be done in coming weeks and months to try to stem some of this damage? Lewis: The Biden proposals are interesting. There’s an $8,000 tax credit to spend on child care. Also, this idea of a much greater entitlement to paid sick leave. Both of which would be hugely beneficial: not just for the individual people involved, but also the social ability to control the pandemic. One of the problems consistently has been the idea that you have to stay at home and self-isolate. Which, if you’re in a precarious, low-paid job, you can’t [easily work from home]. Pandemic infection has often been driven by people who are too poor to do the thing that we would want them to do, so I’m hopeful that it’s possible for the Biden team to make a case that this [isn’t] feminist special pleading. This is actually about helping the whole of society manage the pandemic better. The one thing that the U.S. has been really bad at is opening schools. And I don’t know whether or not that is a lack of will, a reflection of the fact that you’re looking at individual state-level decisions, a fact that the teaching unions have been very reluctant because of huge fears about whether or not workers will be protected if they go back. But other countries have been much more aggressive about saying: Children really suffer when they’re out of school. This is the first thing that we would reopen and the last thing that will close. And I think that America has really suffered from that. And when you look at the more fine-grained details of which women are doing worse, it’s women in their late 30s and 40s [who are] particularly badly hit, because they’re often the ones with a nine-year-old, a six-year-old, and a three-year-old. And that’s the point at which trying to do that and home working becomes just physically impossible. The New York Times did this really good thing called Primal Scream where they had a helpline that people could just phone up and scream. Higgins: If they had the time! Lewis: I imagine a lot of people found it very therapeutic. But one of the pictures that went with it was really fascinating. It was of a guy sitting in his home office and a woman on the phone doing a work call while also trying to potty-train the toddler. And people were very hard on the guy. And if you read the story, he was working three jobs, but that is exactly the picture that I’m talking about. You’ve ended up with breadwinner/homemaker without anybody really wanting that to happen. And I think that there will be a lot of women who feel really sore about that. They worked really hard. Women are now more likely to go to college than men in America. We’re looking at generations of women for whom having a good job and a profession has been an important part of their life, as well as having a family. And they’ve basically been told by their government and by society: Sorry, we’ll get to that if we can. from https://ift.tt/3scOu66 Check out http://natthash.tumblr.com The summer of 2021 is shaping up to be historic. After months of soaring deaths and infections, COVID-19 cases across the United States are declining even more sharply than experts anticipated. This is expected to continue, and rates of serious illness and death will plummet even faster than cases, as high-risk populations are vaccinated. Even academics who have spent the pandemic delivering ominous warnings have shifted their tone to cautiously optimistic now that vaccination rates are exploding. Until very recently, Anthony Fauci had been citing August as the month by which the U.S. could vaccinate 70 to 80 percent of the population and reach herd immunity. Last week, he suddenly threw out May or early June as a window for when most Americans could have access to vaccines. Despite some concerns about new coronavirus variants, Ashish Jha, the dean of the Brown University School of Public Health, told me he doesn’t see viral mutation as reason to expect that most people couldn’t be well protected within that time frame. If all of this holds true, it would mean that many aspects of pre-pandemic life return even before summer is upon us. Because case numbers guide local policies, much of the country could soon have reason to lift many or even most restrictions on distancing, gathering, and masking. Pre-pandemic norms could return to schools, churches, and restaurants. Sports, theater, and cultural events could resume. People could travel and dance indoors and hug grandparents, their own or others’. In most of the U.S., the summer could feel … “normal.” The feeling could even go beyond that. The pain wrought by the virus has differed enormously by location, race, and class, but a global pandemic still may be as close as the world can come to a shared tragedy. Periods of intense hardship are sometimes followed by unique moments of collective catharsis or awakening. The 1918 influenza that left the planet short of some 50 million people—several times as many as had just been killed in a gruesome war—gave way to the Roaring ’20s, when Americans danced and flouted Prohibition, hearing the notes that weren’t being played. For some, the summer of 2021 might conjure that of 1967, when barefoot people swayed languidly in the grass, united by an appreciation for the tenuousness of life. Pre-pandemic complaints about a crowded subway car or a mediocre sandwich could be replaced by the awe of simply riding a bus or sitting in a diner. People might go out of their way to talk with strangers, merely to gaze upon the long-forbidden, exposed mouth of a speaking human. In short, the summer could feel revelatory. The dramatic change in the trajectory and tenor of the news could give a sense that the pandemic is over. The energy of the moment could be an opportunity—or Americans could be dancing in the eye of a hurricane. The life expectancy in the United States is now a year shorter than before COVID-19. No other country has endured so much death and illness. But for all the failures that led to this point, the U.S. does finally seem to be experiencing some protective effects of population-level immunity. Recent research from Columbia University estimates that the U.S. is already much closer to Fauci’s stated threshold of 70 to 80 percent than our case numbers suggest. Owing to minimal and patchwork testing efforts, lead researcher Jeff Shaman told me, the actual number of infections in the U.S. has likely been about five times higher than reported. This would mean that about one in three Americans has already been infected by SARS-CoV-2. This does not alter the goal of vaccinating as many people as possible, but it does mean that while vaccines are rolling out, transmission rates should fall much more rapidly than if the population were all totally susceptible to the virus. In some parts of the United States that have been hit extremely hard by the virus, the numbers give a sense that—if vaccination continues apace—the worst is behind us in those areas. In North and South Dakota, where leaders have been reluctant to require preventive measures, the per capita death rate is about 34 percent higher than the national average, and 13 percent of the population has had a confirmed case. “That probably means that 60 or 65 percent of the population has been infected there,” Shaman said. “That could mean they’re creeping up on herd immunity.” Indeed, North Dakotans have seen relatively few cases this winter, even while most of the U.S. saw a horrific surge. The state’s mask mandate expired a month ago. For the past six days, the state has reported zero COVID-19 deaths. [Read: The good news of COVID-19 is sticking, for now] The warming weather and longer days should also decrease transmission. In much of the world, summers have proved safer than winters during the pandemic, “apparently by virtue of how much time people spend outdoors, and how likely they are to keep windows open and have fresh air circulating,” says Saad Omer, a vaccinologist and the director of the Yale Institute for Global Health. Light and heat can kill the virus directly, but their main effect seems to be making the world more hospitable for us simply to go outside, be social, move our bodies, and improve our baseline levels of health. Although most experts are hesitant to make concrete predictions about exactly when the U.S. can consider its outbreak over, personal plans can be revealing. Jha has famously been hoping to have a July 4 barbecue in his backyard, including 20 people. By August, he told me, he hopes to travel with his family. The pandemic expert and former assistant secretary of homeland security Juliette Kayyem told me much the same last month: “I have plans to travel abroad in August. I feel like the world will start to move well before then.” Where exactly that world is going, however, is far from certain. A beautiful, COVID-free summer may be a vision of hope, and possibly a reality for many, but optimistic projections about the coming months in the U.S. can mean losing sight of a far more unsettling global picture. As things get better, the world could fall into the same patterns that got us to the point of nearly half a million American deaths. “I’m feeling generally optimistic for the U.S. this summer,” Omer says. “But I’m also having nightmares.” Under no circumstances is the coronavirus simply going to disappear this summer. Cases will drop, and restrictions will lift in many places. But rather than an abrupt end to the pandemic, the coming months will be more like the beginning of an extended and still-volatile tail of the outbreak globally. What that will look like, and how long it will last, depends on how nations cooperate and coordinate—or fail to. Regardless of how quickly the immediate threat of viral illness subsides in the U.S., America’s choices in the coming weeks and months could mean the difference between a pandemic that ends this year and one that haunts everyone indefinitely. Though Shaman’s projections about herd immunity may sound hopeful, the fact that the U.S. was able to identify such a small fraction of our cases is evidence of profound, persistent failures in detection, communication, and prevention. Rapid testing will be key to containing local outbreaks, especially next fall and winter. This infrastructure is not yet in place, nor do many Americans have easy access to high-quality masks. We also have a far-from-impeccable record of accepting lifesaving vaccines when they are on offer. Even assuming that almost everyone gets their shots as soon as possible, the Columbia researchers estimate that in the U.S. alone, roughly 29 million additional cases could occur between now and July, depending on how Americans decide to act and which restrictions states choose to lift. “We should really be redoubling our efforts to control the virus,” Shaman said. Variant strains that increase the transmissibility of the virus could also throw these estimates off, Shaman noted. As the virus mutates, the reliability of immunity from prior infections also changes. The recent outbreak in Manaus, Brazil, suggested that even high levels of past infection didn’t necessarily protect a population for long. Fundamentally, we still do not know how herd immunity will work—if it even does. “The most important thing to remind ourselves of is that herd immunity is only relevant to consider if we have a vaccine that blocks transmission,” says Shweta Bansal, a biologist at Georgetown University. If it turns out that vaccinated people can still carry and spread the virus, then a group cannot assume that they are protected because people around them are vaccinated. It would mean that the finish line is not 70 percent, but 100. [Read: The Brazil variant is exposing the world’s vulnerability] In the absence of a mythically perfect vaccine, the value of each dose depends almost entirely on how that dose is deployed. The situation in North Dakota, for example, stands in stark contrast to Vermont, where only 2 percent of the population has had a documented infection. In a place with low levels of immunity, each dose of the vaccine is more valuable than it would be elsewhere—more likely to save a life or prevent a chronic disease. The Trump administration’s approach to vaccination, since inherited by Joe Biden, was to leave it up to states to handle distribution individually, rather than allocate based on where the vaccines could have the biggest impact. Such an approach leaves pockets of the country open to surges in death and disease, despite national averages falling. As Bansal put it, even assuming that the vaccines do make herd immunity possible, the path will not be a straight line so much as “playing a game of whack-a-mole with COVID outbreaks.” If the differences in vulnerability are significant between towns, counties, and states, the global disparities are chasms. Vietnam, for example, is a country of 97 million people that has had fewer than 1,600 cases of COVID-19 and 35 deaths. They have done an exemplary job of controlling the virus, and presumably have very low levels of immunity. Nonetheless, the current scheme of vaccine production—wherein every country is on its own to produce or procure vaccines from private companies selling them at a profit—leads to redundancies at every level, from innovation to distribution, and severe misallocation when comparing one population with another. The coming months could see, for instance, vaccines going to healthy 20-year-olds in North Dakota before much older, chronically ill people in places such as Vietnam. Americans might have to wonder whether we’ll need to wait until April or May to get shots, but many low-income countries may not have widespread access until 2022, or possibly even 2023, notes Ruth Faden, a bioethics professor at Johns Hopkins University. This haphazard approach will mean deaths among high-risk people around the world who could’ve been saved by doses that went to teenage Americans this summer. “From a standpoint of global equity, this is profoundly wrong,” Faden says. Morality aside, it’s also dangerous for everyone. Providing the virus with new places to spread will allow it to linger with us indefinitely. The longer it sticks around, the more time it has to mutate—which is bad news for the entire world, Americans included. “As long as there are large swaths of people who are unprotected, then we’re going to see variants continue to pop up,” Faden says. “And it’s likely that some of those variants will evolve to escape the power of vaccines.” If we are lucky, year over year, SARS-CoV-2 will evolve to cause milder disease than it has these past two years. That would be consistent with the virus that spread in 1918, which became the seasonal flu. It never again produced the same level of mortality as it did during its first two years, but the virus continues to evolve and kill hundreds of thousands of people every year. Most of us have come to accept this as inevitable. For the coronavirus, that fate is not yet entirely sealed. It could still be avoided if we can draw as close as possible to global herd immunity, not a patchwork of immunized nations. This would require a unified effort of governments and pharmaceutical companies to ramp up vaccine production and coordinate distribution. “The reason we have to do all this careful rationing of the vaccines is that the supply is constrained, and the logistics of distribution weren’t worked out in advance,” says Ed Kaplan, a professor at Yale School of Management who has worked extensively in bioterrorism preparedness. “You need a centralized strategy.” Many experts see the United States as singularly positioned to make this happen. “We need to get vaccine manufacturers together and increase production tenfold,” Jha, the dean at Brown, told me, “and the World Health Organization isn’t going to do it.” The WHO has aligned with other groups to form an advocacy network called COVAX, which has relied on donated doses from countries such as Russia and India, while the U.S. and Canada are focused on building up their own supplies. But no other country has the combination of wealth, influence, and infrastructure to orchestrate a definitive, global vaccination movement, Jha said. “Only the U.S. could lead an effort like that.” [Read: What’s the use of a pretty good vaccine?] After President Donald Trump abandoned the World Health Organization, abdicating responsibility to the global community and squandering American credibility, Biden promised to rebuild the country’s reputation as a leader in health and humanitarian efforts. So far, though, his vaccination approach has been emphatically “America first,” having negotiated deals to secure doses for everyone within our borders, with little mention of a pandemic beyond them. Public-health experts have proposed what a more ambitious initiative might look like, based on the way the U.S. invested in the HIV pandemic. Biden could establish the President’s Emergency Plan for Vaccine Access and Relief, or PEPVAR, modeled on the PEPFAR strategy to lead global AIDS eradication, which has been a boon for U.S. diplomacy as well as global health. As opposed to simply donating money or a certain number of vaccines, the U.S. could build a coalition that can actually solve this problem—and stand ready to address any emerging variants or new coronaviruses in the coming months and years. “We will look back with regret on the months the U.S. wasted by not engaging globally,” says Omer, the Yale vaccinologist. “It’s a leadership opportunity. What better moment to rally the world?” This is what could truly make the summer historic. Instead of aspiring to go back to the way things were, we go forward to how things could be. The canonical image of the Summer of Love may be most useful as a cautionary tale. In 1967, a visible minority listened to the Grateful Dead and discovered LSD, but their anti-war sentiment did not stop the U.S. from bombing civilians in Southeast Asia, and Richard Nixon won the White House that fall. The post-pandemic 1920s gave way to yet another war, and a world that would later be unprepared for a global outbreak of a deadly respiratory virus, despite 100 years’ notice. This summer could bring cause for celebration over not simply having made it through this morbid winter alive, but having built a system that can end this pandemic—and stop the next one. It could be when we ensure that no plague of this magnitude happens again. from https://ift.tt/3axrRD6 Check out http://natthash.tumblr.com Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. All major indicators of COVID-19 transmission in the United States continue to fall rapidly. Weekly new cases have fallen from 1.7 million at the national peak in early January to fewer than 600,000 this week, and cases have declined in every state. As we’ve seen at many points in the pandemic, case numbers are changing most quickly, with hospitalizations and deaths declining after a delay: Cases have been falling sharply for five weeks, hospitalizations for four, and deaths for two. In this week’s numbers from nursing homes and other long-term-care facilities, we are now seeing solid declines in deaths correlated with COVID-19 vaccinations in this most vulnerable population. If we look at cartograms of the United States showing weekly new cases for the worst week in January and for the week ending yesterday, the drop in the number of cases in each state is startling. Although states are still reporting large numbers of cases, many more parts of the country show absolute levels much closer to what we saw before the most recent surge accelerated nationally in October. COVID-19 hospitalizations, too, have fallen very sharply. Every region and subregion of the U.S. now shows substantial declines in the number of hospitalized COVID-19 patients. Despite the declines, the total number of people hospitalized is still very high—hospitalizations have yet to fall far enough to reach even the peaks of the two previous surges, which both rose to roughly 60,000 hospitalizations. Here’s what we can tell about cases and deaths among Latino people. Throughout the pandemic, the age-adjusted risk of contracting and dying from the coronavirus has been higher for people of color. With the easing of the huge outbreaks in Arizona and California, we reviewed the data states have reported for Latino people, a group that saw disproportionate numbers of cases and deaths in those states. According to CDC data, Latino people have been 1.3 times more likely to be infected and 2.3 times more likely to die throughout the pandemic in the U.S. compared to white people. But the regional story is quite complex: The effects of the pandemic on Latin American populations have shown wide variation from urban Los Angeles to the rural South. In the West this winter, the huge outbreaks in Southern California and Arizona drove a massive spike in deaths among Latino people, but in the Midwest and Northeast, even as deaths rose Latino deaths did not precisely follow. The differences by region and demographic group are obscured in the top-line numbers and nationwide comparisons. Better state-level race and ethnicity data continue to be necessary to understand these differences in how the pandemic is playing out.
Vaccines are finally showing up in the data, right where we most want to see them. According to the CDC, more than 16 million Americans have now received two doses of either the Pfizer-BioNTech or Moderna vaccine since late December. At least 1.8 million of these fully immunized people are residents of or staff in nursing homes or other long-term-care facilities, and more than 900,000 of that 1.8 million are residents. More than 4 million residents and staff in long-term-care facilities have received at least one dose of a vaccine. Like many people, we expected to see the effects of vaccine distribution show up first in long-term-care facilities. But for weeks, we didn’t see much happening in the data. In retrospect, this makes sense: Many of the people dying of COVID-19 who were reported dead in early February probably contracted COVID-19 in December, given the time it takes for the disease to overcome a body’s defenses and the lags in data-reporting pipelines. As each week passed, we watched and waited to see a clear signal that all those first and second doses were having an effect. During the clinical trials, all of the front-runner COVID-19 vaccines were 100 percent effective at preventing hospitalizations and deaths, even among the oldest participants. In the past two weeks, preliminary (not yet peer-reviewed) real-word data have started to come in, most recently from Israel, showing similar effectiveness in preventing severe illness and even reducing viral load—a finding that could indicate reduced viral transmission. During yesterday’s White House press briefing, Anthony Fauci noted that this research has “very important implications from a public-health standpoint for interfering and diminishing the dynamics of the outbreak.” Now, with the data through February 11, the shift is clear: Deaths are falling in long-term-care facilities. Cases, too, have plummeted. As important, deaths in these facilities are declining not just in absolute numbers, but as a share of COVID-19 deaths in the whole country. In early January, the percentage of COVID-19 deaths associated with outbreaks in long-term-care facilities decreased below 30 percent for the first time since we began collecting LTC data, in May, and it has continued to decrease since. This change correlates strongly with mass vaccinations in these facilities. First, the absolute numbers: Excluding data from Missouri and New York—both of which dumped large numbers of undated deaths into their LTC data in the past month, confounding analysis of both their individual states and the national numbers—the number of deaths in long-term-care facilities has fallen 50 percent from the peak of reported deaths in mid-January. But deaths are clearly falling among all age groups in the U.S., so one could imagine that the declines in long-term-care facilities merely reflect this broader pattern. To test this theory, we looked at the share of deaths that were linked to long-term-care facilities. Remember that these facilities are home to less than 1 percent of the U.S. population. For months, the share of deaths linked to long-term-care facilities bounced between 30 and 40 percent. In mid-January, it was still 29 percent. Then, over the past three weeks, the share of deaths associated with LTC outbreaks began to decline. For the week ending February 11, long-term-care-linked deaths represented just 18 percent of total reported deaths in the states where we have these data. One way to think about this is that the share of deaths associated with long-term-care facilities has been cut in half since early January. Cause and effect have been very difficult to establish in the United States throughout the pandemic. Our national patchwork of data sets and policies has confounded many simple analyses that try to explain why cases or deaths are rising or falling. But this week, we have clear evidence that the vaccines are saving lives in exactly the places where we would expect to see their effects show up first. We are—at long last and after so many failures—beginning to protect the most vulnerable. This week, in Texas, a major crisis has unfolded. Record-cold temperatures locked up the state’s energy infrastructure, causing huge power outages. Local news reports suggest that this slowed or stopped vaccination distribution and administration in many parts of the state. Testing sites were also closed in some areas, like Hidalgo County. It’s not just operations but also reporting that can be disrupted. Over the past year, we’ve seen that major storms can cause significant problems with the COVID-19 data that states report. Sometimes, these problems are easy to spot. A state will simply outright say: We cannot post data today. Other times, the wobbles a storm introduces into the data are not as visible. If people are having trouble moving around a city because of a storm, they are also less likely to seek out testing or even seek medical attention. Because authorities are still able to report something, the interruption is not immediately obvious. As we noted in last week’s update, the early-February snowstorm in New York created data disruptions that artificially depressed COVID-19 statistics for several days. Then, a week later, with normal data pipelines, the seven-day average bounced upward, making it seem as if the decline in tests and cases had reversed. But that was not the case in reality. There are more important issues in the state of Texas right now, but it would not be surprising to see a similar dip and then rebound over the next couple of weeks. With alarm about the variants of concern running high, we caution that it might be difficult to distinguish a data artifact from a fast-moving outbreak with just a week of data. Mandy Brown, Artis Curiskis, Alice Goldfarb, Erin Kissane, Alexis Madrigal, Kara Oehler, Jessica Malaty Rivera, and Peter Walker contributed to this article. from https://ift.tt/3pBzJI2 Check out http://natthash.tumblr.com To celebrate the holidays, the fitness influencer Cory Boling did mountain climbers in his apartment in a pair of camouflage swim trunks. His twin brother, Calvin, did squats while holding a kitchen stool. The duo—muscular, cheerful, constantly shirtless—were two of the most eager participants in a holiday-season Instagram campaign run by the Oklahoma City County Health Department with the help of the influencer marketing agency XOMAD. Their posts were #ads, as well as invitations to stay home for Christmas, wear a mask, stop the spread, keep it tight. For the health department, this was an experiment—a test of whether social-media influencers could reach Oklahoma residents with paid messages, steering them toward behaviors that benefit public health. Now the department has doubled its budget for the real campaign: the one to get Oklahoma residents vaccinated against COVID-19. It is a relatively new and promising approach to vaccination drives, but also one whose effectiveness, and potential downsides, remain unknown. Americans’ willingness to receive a COVID-19 vaccine has been rising steadily since last fall, but a large proportion—a bit less than one-third of those surveyed, according to the most recent polls—is still hesitant. Lisa Sherman, the president of the Ad Council, describes the task of persuading these holdouts to get their shots as “literally the most significant public-education effort we’ve ever undertaken” (and the Ad Council has undertaken some pretty significant public-education efforts in the past). To make things even harder, public-health communicators no longer have the benefit of public figures such as Elvis Presley, who once gave a lift to a national immunization campaign with a single photograph of a rolled-up sleeve. These days, even our most mass-appeal celebrities are not nearly as appealing. Each of them has done something to annoy some chunk of the population, and I’m even talking about Bruce Springsteen right now, and I’m even talking about Hilary Duff. In a pinch, local governments are turning to influencers. Lots of them. As many influencers as they can get. “More is better,” says Jeff Niederdeppe, a communications professor at Cornell University who studies the effectiveness of public-health campaigns. The “level of exposure to the message makes a huge, huge difference.” The biggest public-health campaign of the 21st century so far will involve all the classic tools—TV and radio spots, flyers, and billboards—but an army of influencers may end up being just as central. Whether that army will be successful, though, is another question. No offense at all to the boys with the immaculate biceps, but it’s worth asking what might happen when the nation’s health outcomes are put in the hands of the boys with the immaculate biceps. Influencers look like a simple solution to a common problem for public-health communicators: They need to reach people who don’t want to be reached, but who spend a lot of time on the internet. Familiar faces can affect health-related behaviors, for better or worse. (Imagine a Millennial who vapes because she saw it on Instagram and who gets an annual mammogram because she read about Angelina Jolie’s double mastectomy.) So a local health department might try to use that influence for highly targeted outreach that fills the gaps in traditional media campaigns. Rob Perry, the CEO of XOMAD, told me that his public-health efforts tend to draw on influencers with fewer than 10,000 followers. “What’s important is that they’re not professional influencers,” he said. “They have jobs. The vast majority have never even been paid for a post before we contact them. They have real connections with their followers, and their content is seen as organic.” These campaigns are built on good information, because influencers are able to confer with experts on XOMAD’s custom-built forums. But the campaigns are not specifically about information. They’re about personal stories, emotional appeals, and that buzzword, authenticity. The tactic is a borrowed one, taken from anti-vaccine activists and the vaccine-suspicious wellness influencers who have been parroting their talking points on social media for the past decade. Prior to the pandemic, “the phenomenon of anti-vaccine messaging was going through these networked, authentic voices,” says Kate Starbird, a disinformation researcher at the University of Washington. “The rhetoric is, You can’t trust the government; you can’t trust science; you can’t trust the pharmaceutical companies.” If the government’s top-down communications aren’t getting through, why not try doing what the anti-vaxxers do, and go bottom-up? As far back as 2013, parent groups were floating just this idea, that the anti-vaccine movement’s strategy—its use of personal stories and “authentic” messaging from online influencers—could be weaponized against it. Some public-health researchers have come to similar conclusions, noting that facts alone are often not enough to inspire positive feelings about vaccines. Meanwhile, there is evidence that “social information” encountered on the internet—comments on an online article, for example—can be effective at shifting attitudes and behaviors. Starting with the 2018–19 flu season, Kaiser Permanente put these findings into practice, sponsoring an outreach effort managed by the nonprofit Public Good Projects, specifically targeting Black and Hispanic populations with low immunization rates in several states. In its first year, the company paid more than 100 small-scale influencers to share their personal stories about getting flu shots, tagged #StopFlu. The posts look like any other influencer content: a mom doing yoga, a young couple popping a bottle of champagne, a woman in elegant white pants reclining beneath a mid-century-modern lamp. But they’re paired with text about vaccines: “This year I’m really focusing on my health, and trying to develop healthier habits. One way of doing that is getting myself and my child a flu shot ...” A peer-reviewed study of the campaign’s effectiveness was released at the end of last year. The results were mixed: Surveys showed that people who lived in targeted areas were not significantly more likely to have gotten their flu shot than those who lived in similar places without a #StopFlu campaign on social media, but the researchers also found that the influencers’ posts might have reached close to 10 million people, while generating roughly 70,000 likes, shares, and comments. That was enough for Kaiser Permanente to reboot the campaign for the two flu seasons that followed. The Oklahoma campaign has so far been similarly lacking in clear data to support the project. “We don’t have anything in terms of shifting attitudes,” says Molly Fleming, a communications supervisor in Oklahoma City County’s health department, who got the idea to use vaccine influencers from the chamber of commerce, which pays for Instagram posts encouraging tourism in the area. “The metrics we have are more about how many influencers and how many posts and their reach and that kind of thing,” she told me. (For the upcoming campaign, the health department predicts it will reach 2.45 million people across various social platforms, with a focus on 18-to-34-year-olds.) This makes sense to the extent that the success of many traditional marketing campaigns is measured in anecdotal evidence or in-house data analysis. So far, XOMAD’s influencer campaigns have produced encouraging stories about declining COVID-19 case numbers in Oklahoma City, or informational-app downloads in New Jersey, but that’s not quite scientific. When I asked Niederdeppe what kind of information social scientists and public-health experts would need to determine whether an influencer push on public health had been successful, he sent a bulleted list. First of all, they’d want to know if a campaign reached a large proportion of its target audience—not just whether people had seen it, but whether they could remember it later. Was there evidence that the people who remembered the ads were more likely to say they planned to get vaccinated? Could every other possible explanation for changing attitudes be ruled out? These are things you won’t learn simply by looking at likes and comments, or even countywide vaccination rates. These sorts of campaigns might work, he said, but “there’s not a lot of data there.” Susan Anderson is a nurse anesthetist and lifestyle influencer who participated in a XOMAD-led campaign to promote mask wearing with the state of New Jersey around the holidays. Now she says she feels a duty to discuss the vaccine with her audience of mostly 25-to-45-year-old women—though she has some misgivings about the idea of a paid campaign on that topic. It’s one thing for a health-care worker like herself to share videos about the vaccine, she told me, but the idea that influencers with no relevant background would be posting about vaccines makes her nervous. “I don’t want someone who’s a fashion influencer to say, I went and got the vaccine; it was so cool,” she said. “If you’re saying, I’m taking this vaccine, you should be able to explain why it’s safe.” Talking about vaccines on Instagram has always been fraught. Anti-vaccine sentiments have been particularly contagious among the audiences of what used to be called “mommy bloggers,” through which stories about perceived threats to children tend to spread like wildfire. Early recipients of the COVID-19 vaccine have already been derided on Instagram as “crisis actors” or pawns in various global conspiracies, and anti-vaxxers have coordinated to derail pro-vaccine hashtags by flooding them with their own content. (It was for this reason that the #StopFlu campaign specifically asked influencers to use the term flu shot instead of vaccination.) As Renée DiResta recently argued in The Atlantic, anti-vaxxers have their own digital army, and they see this moment of uncertainty as an opportunity to advance. Could pro-vaccination influencer campaigns help to diminish that uncertainty? Visually, there isn’t much difference between a post recommending a vaccine and a post recommending that the viewer replace a vaccine with essential oils: Both convey a message about doing what feels right for you and your family. Anti-vaccine sentiment tends to spread quickly on social media, so that similarity could be an asset. (XOMAD’s Perry suggested that pro-vaccine influencers would be well positioned to spot emerging myths and misinformation on Instagram, and report them back to health departments.) But it also raises the possibility that pro- and anti-vaccine sentiments could end up as dueling Instagram trends, selected or dropped by influencers as they pick through aesthetics and consumer goods to bolster their following. In fact, when I emailed the body-building Boling twins to ask if they would participate in Oklahoma City County’s vaccine campaign, they wrote back to say no. “Because of the high controversy of the topic with the vaccine and not knowing the long-lasting effects, since it was created in under a year,” they told me, they would not be willing to post. The vaccine, they added, could hurt their brand. As for the influencers who do decide to participate in this campaign—the ones who conclude that pro-vaccine messaging would be good for their brand—nobody really knows what effect they’ll have. “Authenticity” is spoken of in reverent tones by marketers, scientists, and entrepreneurs alike in the Instagram era. But what happens when authenticity and authority are treated as competing values? If health agencies start relying on influencers’ personal stories every time they want to get vital information across—if they start swapping in more and more “organic content” in place of dreary top-down messaging—it may end up signaling, for some, that they’ve abandoned the idea of expertise itself, and turned the most significant public-education effort of our time into a battle over which side’s influencers happen to be most charming and savvy. It’s a tough spot to be in. We could certainly end up regretting these public-health influencer campaigns, though we might regret the alternatives even more. At this point, we need to try every possible method for getting pro-vaccine messaging to the people who need to hear it most. “It’s unfortunate to have to experiment in the moment,” Starbird, at the University of Washington, told me. “But we don’t really have a better option.” from https://ift.tt/3qwHLDt Check out http://natthash.tumblr.com The debates began as 2020 ended and the first vaccines were headed toward authorization. Skip the second dose, some researchers proposed—just one prick of the Pfizer-BioNTech or the Moderna formulation might be enough to do the trick. Jab No. 2 is crucial, others parried, but perhaps it can be postponed longer than the prescribed three or four weeks. No need to screw with the schedule, still others insisted, if the amount of vaccine in each inoculation gets cut in half. The details varied, but the common thread was clear: To combat the limitations of vaccine supply, these controversial proposals suggested, we should stretch the resources we’ve got. The two vaccines now cleared for emergency use in the United States, made by Pfizer-BioNTech and Moderna, respectively, were explicitly green-lit as two-dose regimens on strict schedules. But as new coronavirus variants hopscotch across the globe, and scattered reports indicate that some survivors of COVID-19 may be vulnerable to reinfection, support for tweaking the original playbook has grown. Several leading scientists have, in recent weeks, started to argue that front-loading injections—whether by adjusting the dose schedule or the doses themselves—will more quickly disseminate the partial protection afforded by a single shot. Officials in the United Kingdom are already employing such strategies for the Pfizer vaccine and another, made by AstraZeneca. Some immunological data, and historical precedent, support these types of adjustments, and more might yet emerge. Science is not a game for the dogmatic: Evidence evolves, and our first attempts at designing and doling out coronavirus vaccines certainly won’t be our last. But the details of vaccine distribution have never been a solely scientific decision—not by a long shot. In the absence of public trust, even an immunologically ideal vaccine-dosing regimen won’t be the one that protects the most people. “As a scientist, I’m delighted to hear that [other scientists are] working continually to improve the recommendations on this very important issue,” Stacy Wood, a marketing expert at North Carolina State University who studies how consumers respond to new products, told me. “But as a marketer who is working to try and persuade the vaccine-hesitant, I’m watching my task become that much harder.” All vaccines are designed as teaching tools for the body: an intro course that parades faux or harmless bits of a virus or other pathogen in front of immune cells, so they can learn how to thwart the real thing. Second shots, although not always necessary, are meant to upgrade and prolong that protection. If the first dose is Pathogen 101, the second is an intensive review session to advance the body’s knowledge and ensure that the virus has been committed to long-term memory. In clinical trials, the Moderna and Pfizer vaccines triggered larger antibody responses the second time they were administered—a strong suggestion that they’d bolstered the body’s defenses against the coronavirus. Pfizer’s dosing schedule requires three weeks between shots; Moderna’s, four. Immunity, however, is a spectrum, not a binary. Several experts have pointed out that data from both companies’ trials suggest that some protection kicks in after the first injection. Though the efficacy of a single dose wasn’t rigorously tested, one might be enough to curb the effects of the coronavirus on an otherwise vulnerable population, some argued—akin, perhaps, to driving with a single headlight, or tearing life jackets in two. At the very least, people could stand to wait longer for their second dose, some said, maybe up to a few months after their first. The dose-delay idea rapidly gained proponents—as well as some very vocal critics, many of whom pointed out that clinical trials weren’t set up to determine exactly how much protection the first dose offers, or how long it might last. If a second dose is delivered too late, they argued, the immune system might have forgotten its first encounter with the vaccine, essentially wasting a shot. Others warned that saddling a whole population of people with only partial protection could encourage the coronavirus to linger and mutate in the body, acquiring resistance to the antibodies mounted to quash it. [Read: What’s the use of a pretty good vaccine?] “I’m a firm believer in using products according to the labeling,” Dial Hewlett, an infectious-disease physician in New York, told me. “Until we have data to show one dosing regimen is equivalent to the other, the one that was used in clinical trials, it’s in the best interests of everyone to stick with the dosing regimen at hand.” (It’s worth pointing out that doubling the number of available doses wouldn’t double cities’ and states’ capacity to distribute them.) Still, in the past several weeks, a steady trickle of data and modeling studies have seemed to back the notion of front-loading shots, even if that means delaying second doses. Earlier this month, AstraZeneca boasted that its vaccine—a very different formulation from Moderna’s and Pfizer’s—actually seemed more effective when the inter-dose interval was extended past the originally prescribed four weeks. Johnson & Johnson’s vaccine, which is similar to AstraZeneca’s, will likely earn a go-ahead from the FDA later this month for a single-shot regimen. But the company will also be testing a two-month interval in a trial to determine whether a second shot will improve upon the first. Other multi-dose vaccines, after all, don’t need to be delivered at such a fast clip. Shots that protect against a number of other viruses, including human papillomavirus (HPV), measles virus, and two hepatitis viruses, are given months or years apart. None of these viruses are coronaviruses, and the immune dynamics might differ from vaccine to vaccine. But “a week or two [of delay] isn’t going to make any difference,” Akiko Iwasaki, an immunologist at Yale University, told me. There might even be good reason to give the immune system more time to settle down after it’s been jolted by that first jab, before it must deal with a refresher. Given the logistical hiccups that have already stymied vaccine rollout in several parts of the United States, the CDC recently updated its vaccine guidance to acknowledge that second shots can, if necessary, be administered up to six weeks after the first. Vaccine makers have largely kept mum about the reasoning behind their recommended dose schedules. But Jerica Pitts, a spokesperson for Pfizer, told me that the company’s designated 21-day interval was “a compromise” between spacing the doses far enough apart to ensure that the immune system had time to learn from the first injection, and administering them close enough together to “minimize the time from the start of immunization to protection during the pandemic.” In the rush to protect billions of people, vaccine makers don’t need an immunologically perfect schedule—they need an effective one. As scientists continue to scrutinize vaccine trial data, they are proposing other ways to stretch vaccine supply, or speed vaccine rollout by relaxing existing protocols. Some have suggested that COVID-19 survivors might be good candidates for skipping their second shot entirely, because their encounters with the actual virus may have had the same effect on the immune system as a first shot. Other scientists have proposed that Moderna’s shots could simply be cut in half to instantaneously double supply, given that the formulation contains more than triple the amount of active ingredient found in the very similar Pfizer recipe. Some have even floated the notion of allowing providers to mix and match different types of vaccines, as a way to accommodate those unable to find a second injection of the same type as their first. The coronavirus is a moving target, and both vaccines and vaccine protocols will almost certainly need to shift along with it. But some experts worry that the debate over dosing strategies will undercut public trust in the vaccines themselves. “We went through all these very carefully controlled clinical trials, and at the end, you’re like, ‘Oh, just change it up’?” says Gigi Gronvall, an immunologist at the Johns Hopkins Center for Health Security. From an optics standpoint, she told me, “that doesn’t seem like a good idea.” Those who have already made up their minds about vaccinating or not vaccinating might not be affected by these uncertainties. But people who are still unsure—the “movable middle”—might balk at the notion of scientists operating on guesswork, says Alison Buttenheim, a behavioral scientist who studies vaccine acceptance at the University of Pennsylvania. “For a decision that for some people is already pretty fraught, it just increases the chances that they’ll just throw up their hands and say, ‘Forget it.’” When the experts bicker, what sticks in people’s minds might be the arguing, rather than the merits of the arguments themselves. [Read: What if we never reach herd immunity?] Hewlett told me he’s worried that vaccine hesitancy could exacerbate disparities in Black and Latino communities, which have already been disproportionately hurt by the pandemic and where structural racism in medicine has seeded decades of distrust. “People think, Maybe I should wait until they’ve sorted it all out before I move forward,” he said. He’s already hearing the refrain of “wait and see” from some of his patients and colleagues. The evidence for delaying people’s second dose might be accumulating, but the strategy will still need to overcome behavioral biases to succeed. Multi-shot vaccines are hard to give, especially in regions of the world in which people do not have consistent access to medical resources. A wider dosing interval increases the likelihood that people will forget about or lose interest in returning, says Wood, the marketing researcher. Distant deadlines are a great excuse to procrastinate, until the task itself seems wholly unimportant. A prescribed three- or four-week gap is easier to adhere to. “If we leave it open-ended, it’s an architecture-free choice, and it’s just much less likely to happen,” Buttenheim says. “We don’t want you deciding when your second dose should be.” Vaccine regimens aren’t set in stone, even after they’re formally FDA-approved (which none of the coronavirus vaccines are, yet, only authorized for emergency use). The HPV vaccine, which was initially delivered in three doses, is now doled out in two to certain age groups. Other vaccines have been rolled into multifunctional formulas that protect against multiple bugs at once. The country might soon hit a point when the rollout rules need to change. But even when such shifts are supported by a multitude of data, implementation requires communicating them to the public, and that’s never easy—especially if trust in the vaccine is already fractured. The public can, and should, understand how progress in science is made. But during a crisis, public-health messaging requires both consistency and trust. Vaccine makers will need to maintain transparency about their products; health officials will need to build sustainable partnerships with underserved communities; advocates will need to complement data with true narratives that support the shots’ safety and effectiveness. Wood says that any changes in protocol will be, and should be described as, part of a continuous process of improvement, one that builds iteratively on the astounding success of clinical trials. “It’s not, ‘Oops, we’ve got to do something different,’” she told me. “It’s, ‘This was good. Now this is going to be better.’” from https://ift.tt/3dopPad Check out http://natthash.tumblr.com Vaccine shortages frustrate countries around the world. The lines for vaccines are illogical. But residents of wealthy nations will likely get access to doses in the coming months. It may be much longer for the rest of the world—and, as epidemiologist Gregg Gonsalves explains on the podcast Social Distance, that affects us all and should prompt dramatic action. Listen to his conversation with co-hosts James Hamblin and Maeve Higgins here: Subscribe to Social Distance to receive new episodes as soon as they’re published. What follows is a transcript of the episode, edited and condensed for clarity: Maeve Higgins: A listener named Chris left a voicemail: I have a question about vaccine manufacturing. I was wondering if they could do what we do for generic drugs. Could Pfizer, Moderna, or Johnson & Johnson give their formula—just make it public—and allow other countries or other vaccine makers to just copy their process and increase the supply? I know obviously there are business reasons. They want to make money. But I think it would make sense for maybe the Gates Foundation or a country to just pay them, and say: We’re just going to make this available to everybody to manufacture, so the whole world can have vaccines as quickly as possible. Higgins: What do you think? There’s a vaccine shortage. That seems like a cool solution. James Hamblin: That does sound like a cool idea. It’s more complicated than that might seem, but I’m also not sure it needs to be more complicated. Higgins: I saw your tweet about how the shortage doesn’t need to exist. Hamblin: Yeah, I want to address that specifically, because it became a source of much discussion. I didn’t word it exactly as I would have if I could go back, for the exact same reason: It’s more complicated than that. I think I implied—or at least I know the way people reacted to it, they thought I was saying—that they could snap their fingers and this would happen, and it would be swift and easy. And I didn’t mean that. It’s like when you say something like: We have enough money in the world for everyone to have food and shelter. We have the wealth and capacity to do that. And then you get a bunch of people that say: Well, but there are all these laws where extremely wealthy people don’t have to pay [much in] taxes, so we actually don’t. And both are right. I didn’t mean that this is going to be easy and happen tomorrow. But I do think it’s the solution that’s starting to happen and should have happened already. In any case, I’d like to talk to an expert on this, so we’re going to call Gregg Gonsalves. He’s an epidemiology professor at Yale School of Public Health (where, full disclosure: I’m also a lecturer). He was also on the show in May to talk about his career as an AIDS activist. I couldn’t think of anyone better to talk to about this than Gregg, so let’s give him a call. ~ Gregg Gonsalves joins. ~ Hamblin: Hi, Gregg. We got a listener question asking if we could just have governments produce generic versions of the vaccines. What do you think? Gregg Gonsalves: As you know, vaccines are complex biological molecules. In the case of the mRNA vaccines, [they’re] nucleic acid wrapped in these lipid nanoparticles. Most therapies we put in our bodies in pill form are simple molecules. They’re easy to produce. You have the recipe. You can make the recipe in another factory. The problem with vaccines is: They are complex amalgamations of different kinds of chemical entities. You can’t just follow a recipe. If I started a company and I wanted to make Moderna’s mRNA vaccine, I probably wouldn’t know exactly how to construct that vaccine in the same way, and I’d have to do new clinical trials. It’s not a simple question of making a generic vaccine. That being said, many people, including my colleagues who had an op-ed a few weeks ago, [have called] for a President’s Emergency Plan for Vaccine Access and Relief. They made a case that we should have public production of vaccines. A company like Moderna or Pfizer would be asked by the government, in no uncertain terms: Help us build a government factory to make your vaccine, or help us retrofit another factory to do so. Lonza is making Moderna’s vaccine as a contracted manufacturing plant, so it’s not impossible to do. It requires the ability to exactly reproduce what Moderna does for its vaccine in a set of other plants. Public production would not just be to expand access in the United States and deal with these vaccine limitations, but to do it for the rest of the world Hamblin: A smaller pharmaceutical company is doing contract work with Moderna. I know other smaller companies are doing the same. How is it possible that they’re able to produce these vaccines, but companies that aren’t under contract from Moderna aren’t? Gonsalves: At some point in the development process of Moderna’s vaccine, they said: We’re going to need to scale up. So they went to Lonza and [showed them] exactly what to do: the kinds of machinery, the kind of vats, the kind of lipid-particle processing, RNA-synthesizing machines, et cetera. They gave them very explicit, line-by-line instructions on how to do it. The reason that you and I couldn’t, as theoretical pharmaceutical company owners, just do it on our own is because we don’t know those details. If they did an actual formal tech-transfer agreement with a company, that would be fine. That’s what we’re talking about in public production. The government could say that it’s not that expensive in the long run to build up mRNA vaccine capacity. We’re not going to do it today, but in six months to a year—just as Moderna had to do over the course of 2020—we can build up capacity to do this. Moderna took billions of dollars from us. We can say: You’re going to do this. You’re going to help our new contractors around the country and in Canada and Mexico set up production facilities so we can pump out more of your mRNA vaccines. Hamblin: Right. Gonsalves: It’s totally possible. Higgins: The stakes are so high. There’s such a shortage in the U.S. and worldwide in the global South. Why is there a reluctance to hurry that along? Gonsalves: Cash is king. I don’t want to be crude, but Moderna is pretty clear that you pay to play. We bought up a whole bunch of the vaccine supply in the global North because we were where you were going to get the best bang for your R&D buck. Since the early AIDS epidemic and the early 2000s, when we had these discussions about generic medicines, many foundations—like the Gates Foundation and others—said: If you’re going to develop vaccines, drugs, and diagnostics for the globe, you need to have some sort of global-access policy. Many foundation agreements said that if you take our money, you have to agree to affordable pricing and access to the rest of the world—largely for drugs, but [the Coalition for Epidemic Preparedness Innovations] also initially did this for vaccine development. And in 2019, they reneged on it. Right before the pandemic, they took this affordable-pricing global-access clause out of their licensing agreement, leading Doctors Without Borders to go after them in no uncertain terms and say they were rolling the clock backward right before COVID-19 hit. The point is: Corporations don’t want to give away things for free. In the case of Moderna, taxpayers in the U.S. invested billions in the development of that immunogen. We’re not asking for something for free. We already paid for it. Countries are paying to ensure their own domestic needs. What we need to do—and what we’ve said across the past 20 years—is: Make your buck back in the global North, but you need to make it free and accessible across the rest of the world. Nobody’s planned for global distribution and scale-up. COVAX says maybe we’re going to hit around 20 percent of coverage in 92 low-income countries by the end of this year. Others are going to have to wait until 2022 or 2023 to get access. Higgins: So, one in five people in 92 low-income countries... Gonsalves: Yeah. And when you include all the low-income countries, around three percent of the world’s poor will get access to these vaccines. It’s grotesque. From an ethical perspective, it’s criminal. But if we’re talking about all these new variants, it’s also really dumb. If you’re interested in pushing a virus to evolve to evade your vaccines, the best way to do it is low-level pressure from incomplete, partial vaccination of your population over a long period of time. We know that some of the variants have already had expanded transmissibility. Think of three years of low-level vaccination around the world—and the plethora of variants that’s going to come spewing out across the globe, potentially being resistant to the current Moderna vaccine, the current Pfizer vaccine, the current Johnson & Johnson vaccine... We’re going to be chasing variants around the globe for the foreseeable future and basically have made a death pact for endemic spread of this virus. It’s never going to go away. We’re now on a path where we’re going to have these cycles of coronavirus outbreaks as there are gaps in vaccination across the U.S. and across the world, and as new variants emerge that might be less susceptible to vaccines that we put out into the field. Hamblin: So the half-measures can ultimately be dangerous for the world. Even if wealthy countries didn’t have a sense of morality or obligation to basic equity issues, it’s just not in their own interests. It’s dangerous to their own citizens to not think about this problem. Gonsalves: Yeah. And we said this in the context of the AIDS epidemic. Unless you deal with HIV, it’s always going to be haunting the planet. And people were like: You know what? We have antiretroviral therapy in the U.S. We can manage the disease. Sorry. Now we have a disease where it really doesn’t care where you live. It doesn’t need sex or drugs to transmit itself: just close contact without the requisite preventive measures. The self-preservation instinct right now should be really strong with us about getting global vaccination coverage quickly and broadly across the globe. But I don’t think people are thinking straight. I think they’re looking inward at their national situations. They really don’t understand that we’re all at risk until none of us are basically at risk. And who knows what happens as viral variants emerge and people start to scramble to develop vaccines targeting the new variants and forget about the needs of other countries once again? Hamblin: Right. We could be like: Sorry, we need our second round of updates before you even get one. Gonsalves: Yeah. Sorry, we screwed it up the first time. And then they’re going to screw it up again … Everybody wants to go back to normal. [But we’re going to have] waves of coronavirus infections across the planet that we’ll have to tackle with new vaccines every few years when a variant emerges. So, we’re just going to be living in a new normal. And it could reshape our lives very much like the big catastrophic moments in modern history have to generations before us. We weren’t prepared for it. We’re not rising to the challenge in a way that’s going to make quite a bit of difference. And this isn’t going to be our last time at the rodeo. Pandemics will come at us. AIDS, Ebola, H1N1, swine flu, this now. What’s going to be next? We had a chance to scale up worldwide vaccine production and readiness. If you can’t do it in the midst of a global pandemic, when does it ever get real for anybody? That’s the thing that scares me the most. As a species, we are playing with fire. Hamblin: It sounds like we’re in a moment right now where we could either accept this new normal where, indefinitely and globally, large numbers of people are sick and dying from SARS-CoV-2 and from future variants. Or we could aggressively try to stamp this out by ramping up vaccination in creative ways, like making these a public good. We started talking about a tweet that I had that was not well-worded and got a lot of criticism for the idea that a lot of places around the world could produce these vaccines if we were to think out of the box. I got a lot of pushback—that it’s not possible and only Pfizer and Moderna can basically make these vaccines. Gonsalves: Could we make double the amount of Moderna vaccine with another contractor tomorrow? No. But it took a year for the company to scale up their production capability. And we know that’s true, because there was no SARS-CoV-2 vaccine development in our imagination [not long ago]. If there was political will, the U.S. and other rich countries could underwrite a global production plan for mRNA vaccines. We could make a plan, figure out who’s going to pay for it, and then tell Moderna, Pfizer, and Johnson & Johnson: We’re going to do this as a global community. If NIH wants to exercise its patent rights and tell Moderna to use it or lose it, we can do that too. They’re going to have to provide tech transfers. We can remunerate them for whatever they want. We get that up and running so that, in six months to a year, there’s more capacity to get these highly effective vaccines out there. It’s totally possible to do. People are saying we can’t flip a switch and change everything. And Derek Lowe, who writes for Science magazine, said this in a column. We can’t do this right away. The point is: We can do it; we just can’t do it tomorrow. Hamblin: Yes. I didn’t mean to imply we could do it tomorrow. I realize it kind of read that way, but just because we can’t do it tomorrow doesn’t mean it’s not doable. Gonsalves: They wanted to shut you up. They wanted to tell you it isn’t possible, and that it’s not like a generic drug. No, we can’t do it. We can’t do the capacity. There’s a lot of people throwing up obstacles—when I just think it’s about making a large global business plan about how we’re going to do this. Higgins: Are you saying this vaccine-manufacturing step is about the pandemic either becoming permanent or not becoming permanent? Gonsalves: Well, being permanent and not being permanent—or being worse or worst-est. If we accept the status quo, it’s going to be gruesome for the planet. Horrifying. Both from an epidemiological and a humanitarian perspective. President Biden is a far better steward of our pandemic future [than was President Trump]. But I don’t think he’s thinking globally right now. I don’t think any of the European leaders are thinking this way. This is a much larger global health lift than anything we’ve done before. It’s not impossible. But people have to say vaccine coverage—as broadly and as quickly as possible—is an international goal. It’s not based on charity. Maybe slightly, a little bit. But mostly it’s self-preservation. Because we’re going to be asked to do this again with another pandemic. At some point, we’re gonna have to make a collective decision to act together for our collective self-interest. But right now, it’s every man and woman for himself; every pharmaceutical company for themselves. We’re not on the right path yet. Things are looking up in the United States in terms of the national leadership, but the global situation is pretty catastrophic. from https://ift.tt/2N6OxBc Check out http://natthash.tumblr.com To locate some of the world’s most superpowered cells, look no further than the human immune system. The mission of these hometown heroes is threefold: Memorize the features of dangerous microbes that breach the body’s barriers. Launch an attack to bring them to heel. Then squirrel away intel to quash future assaults. The immune system is comprehensive, capable of dueling with just about every microbe it meets. It’s archival, ace at memorizing the details of its victories and defeats. It might be complicated, but it is also, simply put, cool as hell. Now, a year into a pandemic, our immune systems face a new challenge. The coronavirus has picked up mutations that boost its ability to hop from human to human and thwart some of the antibodies that have reliably conquered it before. The protection offered by vaccines appears riddled with holes. Viruses evolve fast—faster than humans ever could. If the pandemic is a race, the coronavirus seems, at times, on the verge of lapping us. But the immune system is not doomed to be discombobulated by a never-ending barrage of shape-shifting variants. For every trick the virus plays, the immune system arguably has an equally impressive one. Vaccines remain an essential ally, armoring the body before it encounters the virus. And although the variants have opened up gaps in that chain mail, the pliancy built into our bodies can at least buy time to repair them. “Yes, we should be concerned,” Ali Ellebedy, an immunologist at Washington University in St. Louis, told me. “But I think we should also be optimistic.” [Read: What’s the use of a pretty good vaccine?] When any infectious interloper hits, the body’s first responders—the less specialized cells of the innate immune system—rush in to wallop it. Those cells also gather information on the invader and ferry it to the lymph nodes, where they parade pieces of the pathogen in front of the body’s longer-term defenders, the cells of the adaptive immune system. Among these adaptive cells are B cells, each wired to recognize a slightly different hunk of foreign matter. During their development, individual B cells will mix and match segments of genes that encode antibodies, generating billions or trillions of unique combinations. The result is a multitude of Y-shaped molecules that can collectively “respond to any foreign pathogens they see,” says Kim Jacobson, an immunologist at Monash University in Australia. The focus of these antibodies is so laser-sharp that they can differentiate even the individual nooks and crannies that decorate a virus’s surface. The large majority of B cells won’t be triggered by the chunks of virus shuttled in during any given infection. But the few that are will begin to rapidly copy themselves in hopes of joining the fray. Some will immediately transform into antibody factories, pumping out gobs of the Y-shaped molecules to run rapid viral interference. Others, however, will remain in the lymph nodes to further study the virus. Here they will split themselves into more B cells, deliberately introducing errors into their genetic code. If the original genetic scramble created antibodies prepared to take on all manner of pathogens, these random but more subtle tweaks have a chance of enhancing the ability to vanquish the specific virus at hand. The process is a bit like evolution on steroids: Mediocrity gets repeatedly weeded out, leaving only the sharpest and strongest killers behind. By the time a virus has vacated the body, the antibodies being produced against it are, on average, more precise and potent. Much of this painstaking refinement continues after the virus itself is gone: Certain innate cells will cling to scraps of viral corpses—macabre souvenirs of maladies past—to keep the B cells’ boot camp open in the lymph nodes. In a study published last month in the journal Nature, researchers found that the antibodies of COVID-19 survivors continue to strengthen their grip on the coronavirus for several months. “Over time, our antibodies just become better,” Ellebedy said. After infection is cleared, most of the B cells that rallied to the fore will die off, their life purpose fulfilled. But some cloister themselves in the bone marrow, eking out small quantities of antibodies. Others—the so-called memory contingent—will drift quietly throughout the body like sentinels, scanning the blood and tissues for trace signals that the same virus has returned to trouble them again. Called back into action, these memory B cells can immediately start pumping out antibodies. Or they can reenter training centers in the lymph nodes to continue their education on the virus, honing their defensive skills further. [Read: Immunology is where intuition goes to die] In epic tales of the immune system, B cells and their antibodies tend to hog the limelight. Antibodies, which are proteins that drift through the blood, are easy to capture and measure; they’re sometimes powerful enough to waylay a virus before it has the chance to break into a cell. But no antibodies would be produced without the help of T cells, which coax B cells into maturing and play vital roles in their training regimen—loyal wingmen at the ready. T cells are also formidable foes in their own right, capable of recognizing virus-infected cells and forcing them to self-destruct. T cells don’t undergo the same supercharged mutation process that their B-cell colleagues do. They are stuck with the pathogen sensors they’re born with. But the starting repertoire of T cells, and the number of bugs they can recognize, is similarly massive. And like their B-cell counterparts, T cells are capable of remembering past pathogenic encounters—and their discerning gaze is especially difficult to elude. When viruses undergo a substantial costume change, it can disrupt this iterative process. It’s a big part of why flu vaccines have to be updated every year, Ellebedy said: “We are always trying to catch up with the virus.” But coronaviruses mutate far more slowly than flu viruses do. And this new one has yet to undergo a makeover that fully neuters the vaccines we’ve developed against it. “I think there’s probably a very small probability that there will be complete escape,” David Masopust, an immunologist at the University of Minnesota, told me. B cells and T cells develop so many unique ways of recognizing a given virus that any one mutation, or even a handful, won’t fully thwart them. A change to the equivalent of a virus’s elbow, for example, will have little impact on a T cell’s ability to recognize its earlobe. Memory cells will rapidly seize upon commonalities between the two versions of the virus; in some people, this alone could be enough to nip an infection in the bud. Certain memory cells—especially T cells—might have enough flexibility to recognize a modified version of their viral target. Experts call this “cross-reactivity,” and it’s a crucial part of the T cell way of life, Laura Su, an immunologist at the University of Pennsylvania, told me. Some scientists have hypothesized that T cells previously marshaled against other coronaviruses, such as those that cause common colds, might even play a small role in quelling this new one. Even in the complete absence of memory and cross-reactivity, the body still has a huge reserve of backup cells—the multitude of B and T cells that were not triggered by the first go-round with the virus, Su said. The war against variants is not a fight just for veterans: Chances are, rookies are waiting in the lymph nodes to be called to the front lines. Depending on the extent of the virus’s metamorphosis, another infection, perhaps another illness, may be possible. But the body is not left wholly defenseless. [Read: What if we never reach herd immunity?] In South Africa, where an immunity-dodging coronavirus variant was recently identified, drops in vaccine efficacy showcase the tight foxtrot between the virus’s mutability and the immune system's adaptability. Johnson & Johnson’s numbers fell from 72 to 57 percent; Novavax’s, from 89 to 49 percent (though this last number ticked up to 60 percent when the researchers considered only people who were not living with HIV, a virus that blunts the immune system). But neither vaccine’s efficacy plummeted to zero—not even close. Most vaccinated immune systems, it seems, have yet to be fully flummoxed by the variant. “The biggest misconception is these immune responses are all or none,” Marc Jenkins, an immunologist at the University of Minnesota, told me. But as my colleague Sarah Zhang has written, vaccines function more like a dimmer than a light switch, tuning down the risk of serious COVID-19 along a hazy spectrum. Importantly, the vaccines still seem to largely ward off severe disease and death—a hint that residual antibodies and T cells are still making a dent, Jenkins said. The stunning data from Moderna’s and Pfizer’s trials, which suggest that their vaccines are about 95 percent effective at preventing COVID-19, also leave more wiggle room for unexpected hurdles. (Scientists also expect that these vaccines will undergo mild to moderate dips in efficacy against the variants, based on early data from laboratory experiments.) The protection offered by vaccines doesn’t need to be bulletproof to have an effect. “Even if vaccination does not prevent infection, the B cells and T cells will prevent severe disease and bolster immunity, which is incredibly important,” Smita Iyer, an immunologist at UC Davis, told me. One unusual phenomenon that’s been documented with flu viruses did give a few immunologists pause. In some cases, immune cells may be so taken with one version of a virus that they struggle to react to another. Although memory cells might still react strongly to parts of the virus that are familiar, their responses to the changed bits will be considerably lackluster—the result of a kind of stubborn imprinting that leaves cells “stuck in the past,” as Su described it. Scientists aren’t sure exactly why or how this bias occurs. But the cells’ recalcitrance can imperil the body’s ability to catalog new versions of a virus and guard against them in the future. Nothing yet suggests that this problem is cropping up with the new coronavirus, Ellebedy said. But researchers will be on the lookout as the variants continue to disperse across the globe. Vaccine makers are already starting to retool their formulations to account for the new variants: Some have set their sights on strain-specific boosters, while others tinker with recipes that could tackle multiple virus versions at once. But the vaccines we have still work—and rolling them out widely and rapidly will help starve the virus of new hosts, and new opportunities to mutate and surge further ahead. “Viruses evolve—that is a fact,” Iyer told me. “The best solution is to stop the viruses from spreading.” from https://ift.tt/2NpxKcn Check out http://natthash.tumblr.com Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. Nationally, all signs point to continued rapid easing of the pandemic’s deadly winter surge. Cases are down 23 percent from the previous week and down 57 percent from the country’s all-time peak in early January when the U.S. recorded 1.7 million new cases in a single week. Hospitalization numbers confirm this rapid decline: There are about 77,000 people hospitalized with COVID-19 in the U.S. as of February 10, down 42 percent from the country’s January 6 record of about 132,000 people. Reported deaths dropped for the second week in a row, with 19,266 deaths reported this week—almost 10 percent fewer than were reported in the previous week. (We have excluded from this count the 1,507 historical deaths Indiana reported with no corresponding dates on February 4; these deaths are included in our API and cumulative death count.) Testing dropped 8 percent this week, the third week of declines for that metric. 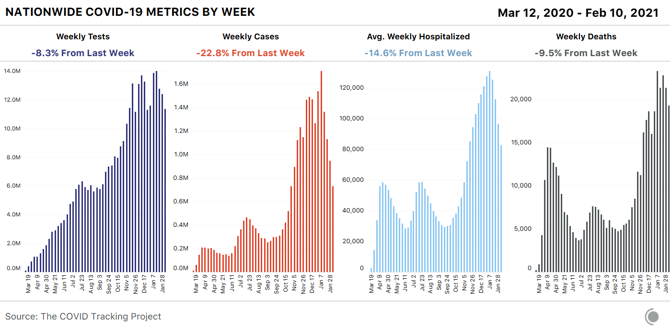
Data users planning to switch to federal data sources when our project ceases data compilation in March will be interested to note that the CDC’s case data match ours almost exactly: The two data sets are 0.018 percent apart on the seven-day average as of February 9. 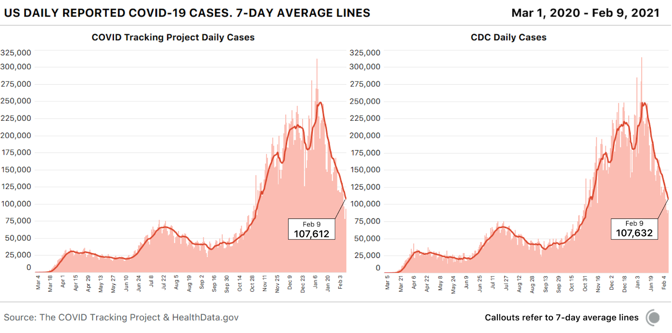
The national case decline is still reflected in a strong downward trajectory in three of the four U.S. census regions—but notably, the Northeast is no longer showing a case drop. We decided to look into that regional signal by investigating regional hospitalizations. 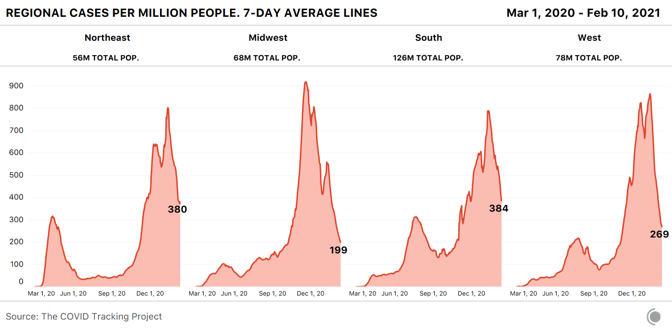
We often refer to current hospitalizations as a way of helping us understand the severity of COVID-19 outbreaks across the country, but it’s not the only useful hospital metric for this purpose. The current-hospitalizations metric measures the burden on hospitals effectively, but because it is affected by both new COVID-19 admissions and COVID-19 patients leaving the hospital, it’s not as good at revealing the direction of outbreaks. Particularly given that more transmissible variants of SARS-CoV-2 have been identified in much of the country, we’ve also been watching the new hospital-admissions data from the Department of Health and Human Services for early signals of directional change in outbreaks. A per capita view of the new admissions data suggests that the Midwest, South, and West are all continuing to see new COVID-19 admissions decline, but the Northeast is now showing a small but noticeable increase in new admissions in the seven-day average. The little upward hook in the seven-day average of the Northeast’s hospital admissions chart looks surprisingly similar to the one we saw in regional cases. But where is it coming from? A state view shows where this admissions data might indicate a worsening situation: Connecticut and New York, especially, are showing notable increases in new admissions. But as we saw during the winter holidays, a confounding factor is in play for some metrics in the Northeast—not a holiday, this time, but the weather. 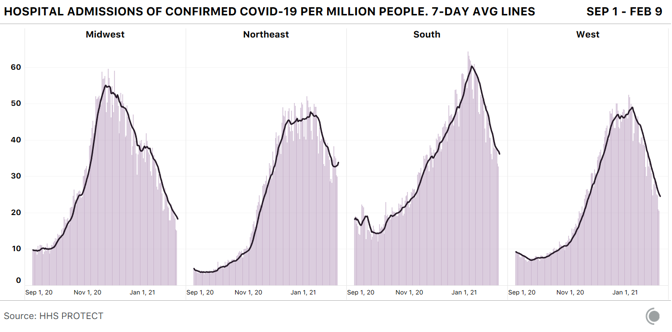
The nor’easter that affected much of the region from January 31 to February 3 appears to be visible in both case and test data as a drop followed by a recovery—and the storm very likely depressed hospital admissions as well, accounting for much of the matching upward tick we’re seeing in that metric in recent days. 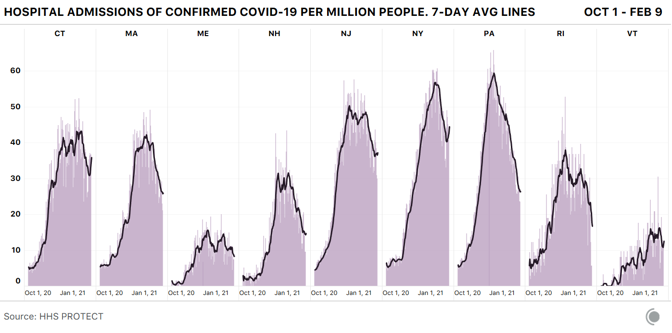
Still, the storm doesn’t explain other worrying indicators: New York currently has the highest per capita number of COVID-19 hospitalizations in the country, and the state’s hospitalizations aren’t falling as rapidly as they have in the recent hot-spot states of Arizona, California, and Georgia. And in a high-population state like New York, high per capita numbers translate into very high absolute counts. The facility-level hospitalization data from HHS provide an overview of COVID-19 hospitalizations across the U.S., including a look at the astonishing scale of hospitalizations in and near New York City. 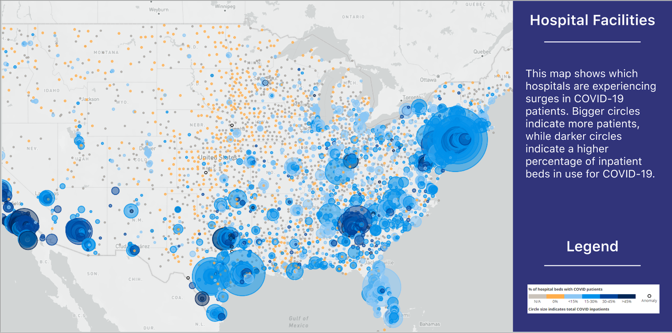
Meanwhile, restaurants in New York State will be permitted to reopen indoor dining at 25 percent capacity beginning tomorrow. We continue to watch every metric closely in the Northeast—and the rest of the country—and we caution data observers to take particular care when identifying short-term trends that may be explicable by non-pandemic factors. This week’s chart excludes data from both Missouri and New York, both of which recently released very large cumulative additions to their data for long-term-care facilities without any corresponding historical time series, resulting in artificial spikes in our national data. The figures from these states are important, and remain in our data set, but when charted, they obscure trends from the rest of the country. Those trends are good: Nursing homes and other long-term-care facilities saw decreases in cases and deaths in our most recent week of data for these facilities, which runs January 28 through February 4. We wrote about Missouri’s release of cumulative historical data on cases and deaths associated with long-term-care facilities in last week’s update, and this week, we have even more confusing data from New York State. Throughout the pandemic, we’ve known that New York’s reported deaths from long-term-care-facility outbreaks were an undercount, because the state attributed deaths to long-term-care facilities only if patients actually died in the long-term-care facility. Any resident who contracted COVID-19 in an outbreak in a nursing home or assisted-living facility in New York and then died after being taken to a hospital, for example, was counted as a COVID-19 death in New York State, but not as a long-term-care-facility death. On January 28, after New York Attorney General Letitia James called attention to New York’s undercount of deaths in nursing homes, state Health Commissioner Howard Zucker issued a statement that attributed to New York State nursing homes an additional 3,829 deaths that occurred as far back as March 1, 2020. In the two weeks since this statement, New York has added a total of 5,620 deaths associated with nursing homes and long-term-care facilities to its dashboard, nearly doubling the state’s cumulative count of deaths associated with these facilities. New York has not provided any dates for these deaths, so we’re unable to backfill them into the correct weeks. Based on average reporting from the state in January, it is likely that up to about 600 of these deaths took place recently. This suggests that the state’s audit has to date revealed approximately 5,000 deaths associated with outbreaks in nursing homes and assisted-living facilities that the state had previously declined to attribute to those outbreaks. Meanwhile, a peer-reviewed study of more than 13,000 U.S. nursing homes published this week in JAMA Network Open suggests that nursing homes with the highest proportions of nonwhite residents experienced COVID-19 death counts that were more than three times higher than those of facilities with the highest proportions of white residents. The testing decline we’re now seeing is almost certainly due to a combination of reduced demand as well as reduced availability or accessibility of testing. Demand for testing may have dropped because fewer people are sick or have been exposed to infected individuals, but also perhaps because testing isn’t being promoted as heavily. The resolution of holiday reporting backlogs also almost certainly produced an artificial spike in the number of tests reported in early January—which means the decline we’re seeing now looks particularly dramatic when measured against that postholiday spike. 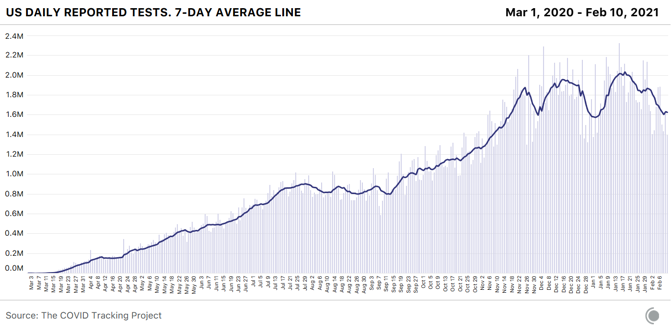
Even if we adjust for holiday effects and estimate that we’re really testing only 1 million fewer people each week than we did a month ago, that’s unequivocally the wrong direction for a country that needs to understand the movements of the virus during a slow vaccine rollout and the spread of multiple new variants. According to public-health experts, we’re also still not doing enough testing, —and we weren’t doing enough even at the January testing peak. Back in October, the Harvard Global Health Institute and NPR released testing targets that set a national target of about 2 million PCR tests a day. If we discount holiday effects, the United States finally hit that target in the week ending January 20, when states reported about 14 million tests—though the number immediately began dropping. But the HGHI test targets were based on October 1 case counts, and even after weeks of declines, we’re seeing more than twice as many new cases a day now as in early October. Vaccinations are only one component of the effort to get the pandemic under control and prevent another devastating surge. We need to be testing at our full capacity—and increasing that capacity—to keep eyes on the pandemic as we move into spring. Both testing and hospitalization data are crucially important COVID-19 metrics, helping us understand how the pandemic is changing and how to interpret other data we’re collecting. The race and ethnicity data for these metrics remain deeply inadequate in both state and federal data sources. Nearly a year into the U.S. pandemic, only 23 states report or have reported any data about the race and ethnicity of people hospitalized with COVID-19, and only nine states share data about the race and ethnicity of people who receive COVID-19 tests. As Marcella Nunez-Smith, the chair of the Biden-Harris COVID-19 Health Equity Task Force, said at a Kaiser Family Foundation briefing in December 2020, “There is violence in data invisibility. We cannot address what we cannot see. We are making a choice every time we allow poor-quality data to hinder our ability to intervene on racial and ethnic inequities.” 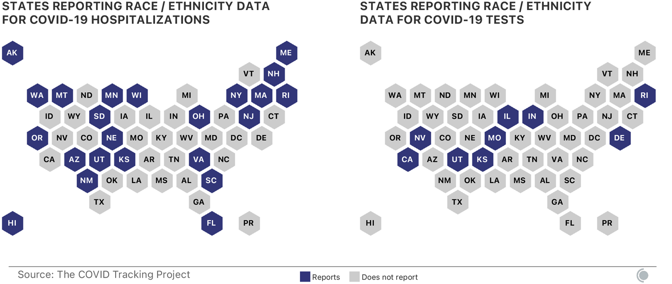
Although media and policy attention is increasingly focused on the lack of demographic data for vaccinations—data on race and ethnicity are missing for about half of all first doses administered in the first month of the U.S. vaccine rollout, according to a CDC report—demographic data for other COVID-19 metrics remain essential for identifying inequities in either impact or response. Without good, public demographic data on hospitalizations and tests, there can be no accountability for efforts to identify and address inequities. States and the federal government should work together to ensure that hospitals and testing providers are collecting sufficient demographic data, and that these data are rapidly and publicly shared. from https://ift.tt/378uN74 Check out http://natthash.tumblr.com 
On her first night home from the hospital, between bouts of writhing in pain, my grandmother stopped to ask me, over and over, “Qu’est-ce que j’ai fait?”: “What did I do?” My grandmother, Denise, is 82 and in the late stages of Alzheimer’s disease, which means she can no longer form new memories. Late last summer—it’s impossible to say when, exactly—she fell and fractured a vertebra. Immediately, she forgot it had happened. Pain became the fall’s only remnant evidence. It took my family weeks, and two hospital trips, to understand why she’d stopped eating or getting out of bed. In anticipation of her second discharge from the hospital, I traveled to France to take care of her. When I arrived at the apartment where she lived alone, I was entirely unprepared for how intensely the Alzheimer’s could amplify her suffering. My grandmother’s throat rattled with every breath. She moaned in her sleep. In childlike tantrums, she kicked her legs and flailed her arms when I tried to get her out of bed to eat. She developed a cough so intense that it sounded, from a room away, like vomiting, and sometimes did turn into vomiting as her body tried to convulse the pain away. She couldn’t tell day from night, and she got lost in her own home, even in her own bedroom. Every few minutes, she resurfaced to rediscover her agony, resulting in a panic that made her even more vulnerable to its punishment. My grandmother’s pain was undeniable. And yet, somehow, it was incomprehensible to both of us. In all cases, pain management is a thorny endeavor. “To have pain is to have certainty,” the essayist Elaine Scarry wrote in her 1985 book, The Body in Pain. “To hear about pain is to have doubt.” Helping someone cope with pain requires glimpsing, through imagination alone, the invisible interior of another person’s body—and then accepting that imagined suffering as real and true. When a patient’s cognitive condition prevents reliable self-assessment, as is the case for my grandmother, our ability to see a person’s pain and treat what we see is even further limited. For caretakers of people with dementia, the riddle of their suffering becomes nearly unsolvable. Alzheimer’s disease, the most frequent cause of dementia, can undermine the entire process of conveying pain, from perception to communication. A person with Alzheimer’s might express discomfort by wandering, moaning, or refusing to eat or sleep, but the same behaviors might express loneliness, or hunger, or sadness—or they might be symptoms of the disease itself. Asked to choose which emotional expression on a chart matches their current state, a person with Alzheimer’s might, in confusion, point to the face they think they should feel. Dr. Sharon Brangman, a geriatrician at SUNY Upstate, told me about a patient who complained of frequent headaches. Only later did she realize that “headache” was the woman’s metaphor for not being able to remember. “It just adds to the complexity of taking care of people with Alzheimer’s disease,” Brangman said. “That person may not be able to communicate what’s wrong with them.” Instead of figuring out how to ease the suffering, caregivers are stuck simply trying to understand its source. And there are a lot of possibilities. In the U.S., an estimated 5.8 million people aged 65 or older have Alzheimer’s—a figure expected to balloon to 13.8 million by 2050 as the population continues to age. One in three seniors dies with dementia. Dementia doesn’t preclude any of the common sources of pain for the elderly, of course—cancer, surgeries, arthritis, osteoporosis, fibromyalgia, ulcers, injuries from falls, and on and on. It does, however, make it more difficult to identify that pain and less likely that it will be taken care of. An estimated one-third of homebound dementia patients and two-thirds of older nursing-home residents with dementia suffer through undiagnosed or unaddressed pain. “It’s a population that’s just silently suffering,” Todd Monroe, a registered nurse and neuroscientist at Ohio State University, says. “This is not going away. It’s only going to get magnified.” In addition to the five senses, nineteenth-century German academics believed in Gemeingefühl: a slate of perceivable bodily states “in the most diffuse and general sense”—fluctuating temperatures, rushing blood, lurching organs, hunger, thirst, breathlessness, and physical pressures like pain, itching, and tickling. These academics explained the mystery of chronic “pain without lesion” as a disorder of Gemeingefühl—an inability to correctly perceive internal sensations. When, in the mid-1970s, the McGill University psychologist Ron Melzack began developing a modern pain assessment still widely used today, he believed that language could ferry pain from this unknowable “borderland between soma and psyche” into the realm of treatable medicine. After collecting 102 words used by patients at a pain clinic to describe their various agonies, Melzack set out to find a framework within this list that could not only quantify the physical intensity of a person’s hurt but also assess their experience of it. “It gradually dawned on me that the words could serve as a questionnaire that would provide credible evidence of the perceived, subjective qualities of a person’s pain,” he later recalled, “and perhaps throw light on what parts of the brain were involved in producing such feelings.” [Read: Beating Alzheimer’s with brain waves] Melzack’s invention, the McGill Pain Questionnaire, or MPQ, asked patients to describe their pain using words that fell into three categories: the sensory, the affective, and the evaluative. The sensory category identifies pain’s physicality through qualities such as temperature, intensity, and magnitude. (As virtually everyone knows, pain can prickle, or shoot, or ache, or sting—and each of these sensations can be unlike any of the others.) Words within the second, affective category capture pain’s emotional impact—whether it exhausts or sickens, terrifies or tortures. The third, final, and most narrow evaluative category assesses the overall episode: Was it annoying, miserable, intense, unbearable? Within this vocabulary, language can provide “an external image of interior events,” as the essayist Scarry put it. Questionnaires like the MPQ also elevated pain from a handful of physical symptoms to an experience nested in emotion, environment, and expectation. “Pain is not one thing. There’s pain, and there’s the suffering of pain,” says Nancy Berlinger, a researcher at the Hastings Center, a nonprofit bioethics institute. “What you’re feeling, and how you feel about it.” Sadly, Alzheimer’s irreversibly robs a person of the cognition required to make this conception of pain medically useful. As the disease advances, a person loses the ability to create new memories, use language, control emotions, and critically perceive, analyze, or convey the world around and inside them. Over the past quarter century, about 30 different tools or methods have been developed to specifically assess pain in people with dementia. Unfortunately, general practitioners who take care of these patients are often not even aware of their existence. (A 2018 survey of 157 GPs in Ireland found while 98 percent of respondents agreed that dementia makes pain difficult to assess, only 10 percent were aware of any dementia-specific pain-assessment tools.) And evidence for their effectiveness often comes from studies with small sample sizes and other sources of biases, critics say. Among the dozens of options, there is no general agreement on which instrument or technique should be recommended for patients with dementia. “There’s not one single tool that’s determined to be the best,” Monroe, of Ohio State, says. “The science is just not there.” Part of the problem, experts say, is the uncertainty about how Alzheimer’s disease affects a person’s various pain-perception networks. It’s clear that the disease impacts their ability to assign meaning to pain, but it’s unclear exactly how. That has led to some cruel assumptions about people with Alzheimer’s. For decades, some caretakers—professional and otherwise—decided it wasn’t worth the hassle of treatment if the patient couldn’t perceive physical sensations or would soon forget any unpleasant episodes. “Anecdotally, I would hear that Alzheimer’s patients don’t feel pain, or they don’t feel it as much,” Monroe says. “I thought, how do you know? We don’t know they’re hurting less. What if they’re hurting more?” The body processes pain through several interconnected neural networks that help a person feel, describe, understand, and respond to pain. Preliminary research in neuroscience suggests that the major brain regions involved in pain perception and processing still function, albeit differently, in people with Alzheimer’s. In controlled lab settings, there’s no absence of brain activity in the areas related to pain, Monroe says. “If somebody thinks dementia has just messed the brain up so much they don’t feel pain, I can safely say that’s not the case.” But that doesn’t mean we understand what those differences signify for how those with Alzheimer’s feel and understand pain. We don’t even know how the disease impacts the blood-brain barrier, which could impact the effectiveness of pain medications. “To date, the limited and relatively small studies on pain perception in dementia patients have produced conflicting and even contradictory findings,” Italian researchers remarked in 2019. This inconclusiveness reflects the practical challenges to dementia brain studies: coordinating caregiver schedules, overcoming transportation issues, getting patients into claustrophobia-inducing MRI machines, and keeping them still enough for imaging. Patients with advanced dementia might not be able to reasonably understand study procedures and provide consent to be experimental subjects. In one 2019 project, five years of active recruitment led by a dedicated recruitment specialist and a full-time research assistant resulted in the successful testing of fewer than two participants, on average, per month. The result is that most of the existing clinical research has been conducted on participants who are younger, healthier, whiter, and more mobile than the overall dementia population (women and Black and Latino people are the most likely to develop dementia). Any treatments based on these studies might not work as well in patients not represented in the trials—which is to say, most people with dementia. “I don’t think we have enough answers,” Brangman told me. “And it’s not the patient’s problem. It’s our problem.” 
Without reliable research to guide them, caregivers are left to rely on their patients’ visible symptoms of untreated discomfort—exclamations like “Ow” or “Ouch,” and movements like massaging, rocking, or hand-wringing. But even for people closest to the patient, these signals can be easy to misinterpret. Brangman has seen patients become agitated not because of pain or anger, but because of low blood sugar or high blood pressure. They might stop sleeping because they’re uncomfortable or cold or stop eating because they’re lonely. Rena McDaniel, a family caregiver in South Carolina, told me her mother often complained of chest pain and trouble breathing in the last five years of her life. Doctors told McDaniel it was only allergies, though allergy medicine did nothing to alleviate any discomfort. Some suggested that her mother wasn’t feeling the pain she was describing. One doctor wrote it off as a cry for attention. As it turned out, McDaniel’s mother had been suffering from breast cancer, which had, by then, metastasized throughout her body. She died less than six months after the cancer diagnosis. “We didn’t put two and two together until it was much too late,” McDaniel said. “I still feel guilty to this day for not listening to her instead of the doctors.” In my own experience, my grandmother moaned through the night even when we gave her the painkillers prescribed for her fractured vertebra. She only stopped when someone was in the room with her. It took time to understand that she wasn’t groaning in pain; she seemed to be moaning in fear. Providers’ misreading of such cues has led to the dangerous mis-prescription of antipsychotics to dementia patients whose behavioral changes are caused not by mental illness but by emotional distress from untreated pain. [Read: Is the leading theory about Alzheimer’s wrong?] “You have to look for other signals that they’re uncomfortable. And it’s not one set thing,” Brangman said. “It takes a lot of intuitive work and careful examination.” Given the tightening squeeze on geriatric care in the U.S., it’s not always possible for practitioners to form these kinds of close, sustained relationships with their patients. “We’re heading toward a medical emergency,” Joanne Pike, the chief program officer for the Alzheimer’s Association, said last year. In 2016, the U.S. had about one geriatrician for every 2,000 older Americans in need of their service. Less than 1 percent of registered nurses, physician assistants, and pharmacists specialize in geriatrics, according to the Alzheimer’s Association, and even fewer of them are trained to deal with the complexities of dementia. As the number of people with Alzheimer’s more than doubles by 2050, all of these caregivers, Pike warned, “are about to be under siege.” In the absence of a robust professional workforce, family members, friends, or other unpaid caregivers provide a large majority—about 83 percent—of elderly care. Among them, more than 16 million provide an estimated $244 billion worth of care for those with Alzheimer’s or other forms of dementia. Half of them have no medical experience, but they must nevertheless try to translate subtle facial expressions or unusual habits to doctors and nurses when they suspect that a person with dementia is suffering from untreated pain. “Families deal with this by themselves, and it’s wrong,” Berlinger, of the Hastings Center, says. Many of the experts I spoke with had relatives or friends who had suffered from these diseases. Berlinger’s father had dementia, as do some of Brangman’s relatives. Monroe’s grandmother battled breast cancer and Alzheimer’s at the end of her life. As caretakers, they felt a powerlessness they’ve tried to dismantle through research or medical care. Alison Anderson, a nurse practitioner and dementia researcher at Vanderbilt University, watched her mother struggle through early dementia as she began studying the disease. In 2017, Anderson examined existing research and found study after study suggesting that the basics of care—touch, interaction, and the presence of another human being—can help relieve pain in dementia patients. Luckily for my family, my grandmother now resides in the Alzheimer’s wing of a nursing home, where she is never alone. But when I cared for my grandmother, I found that our moments of communion kept her physical agony at bay. We rooted through boxes of old photographs together, and I distracted her with stories about how I had filled my suitcase with sesame bagels for her. I played guitar while she napped. On the worst of days, all I could do for her was lie down in bed beside her as she whimpered. More than once, we fell asleep holding hands. “Je t’aime,” she’d repeat, finally unburdened. “J’ai pas peur”: “I love you. I’m not afraid.” from https://ift.tt/3acnv4s Check out http://natthash.tumblr.com |
Authorhttp://natthash.tumblr.com Archives
April 2023
Categories |
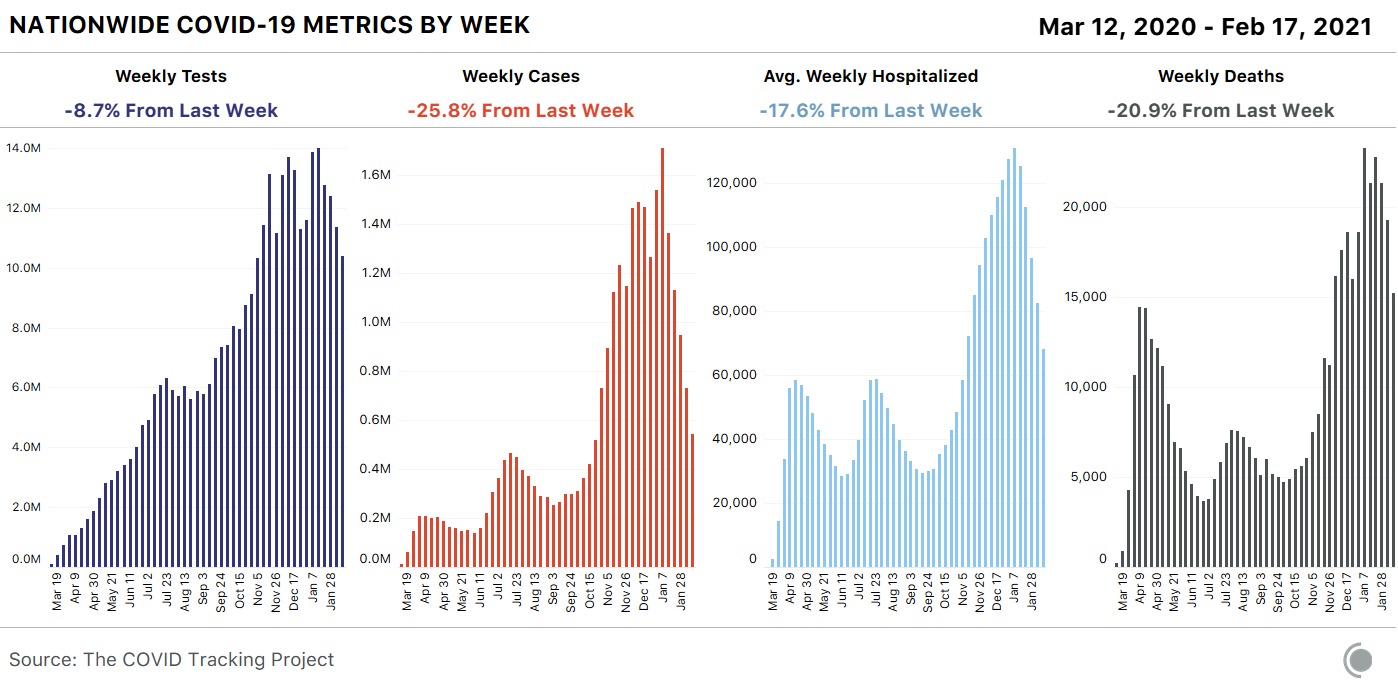
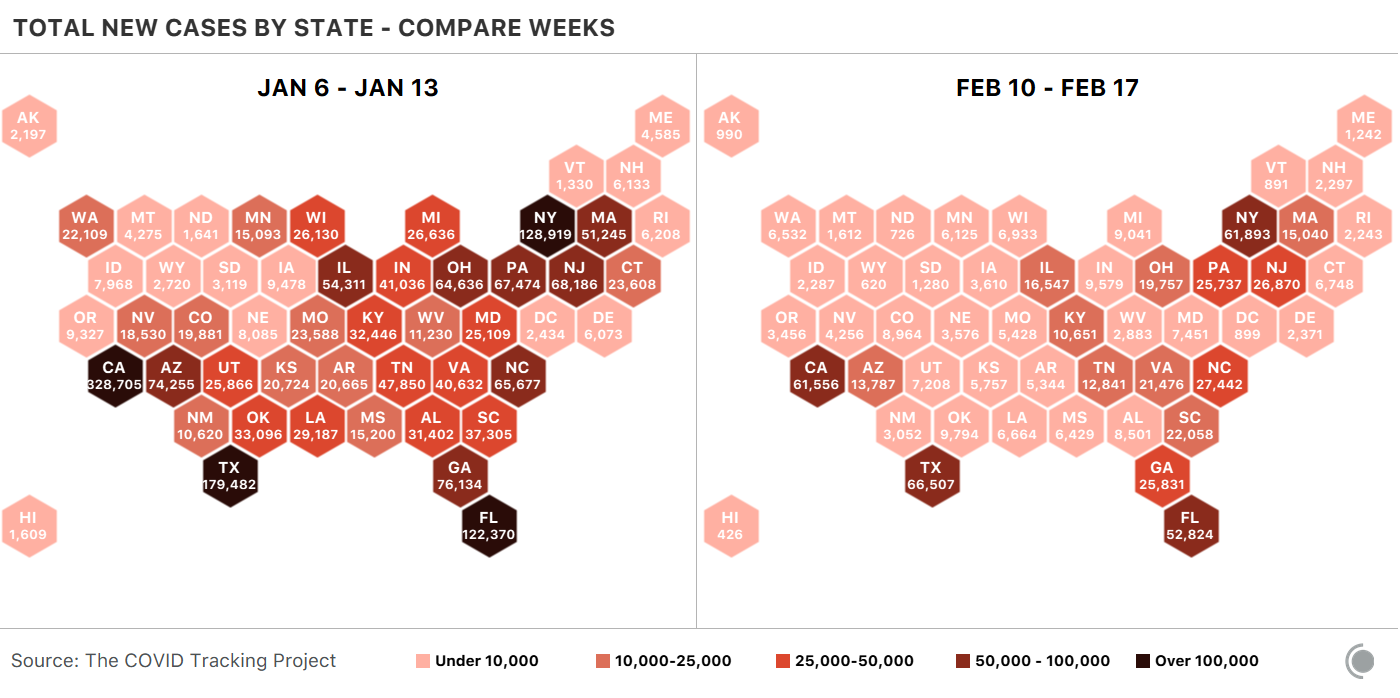
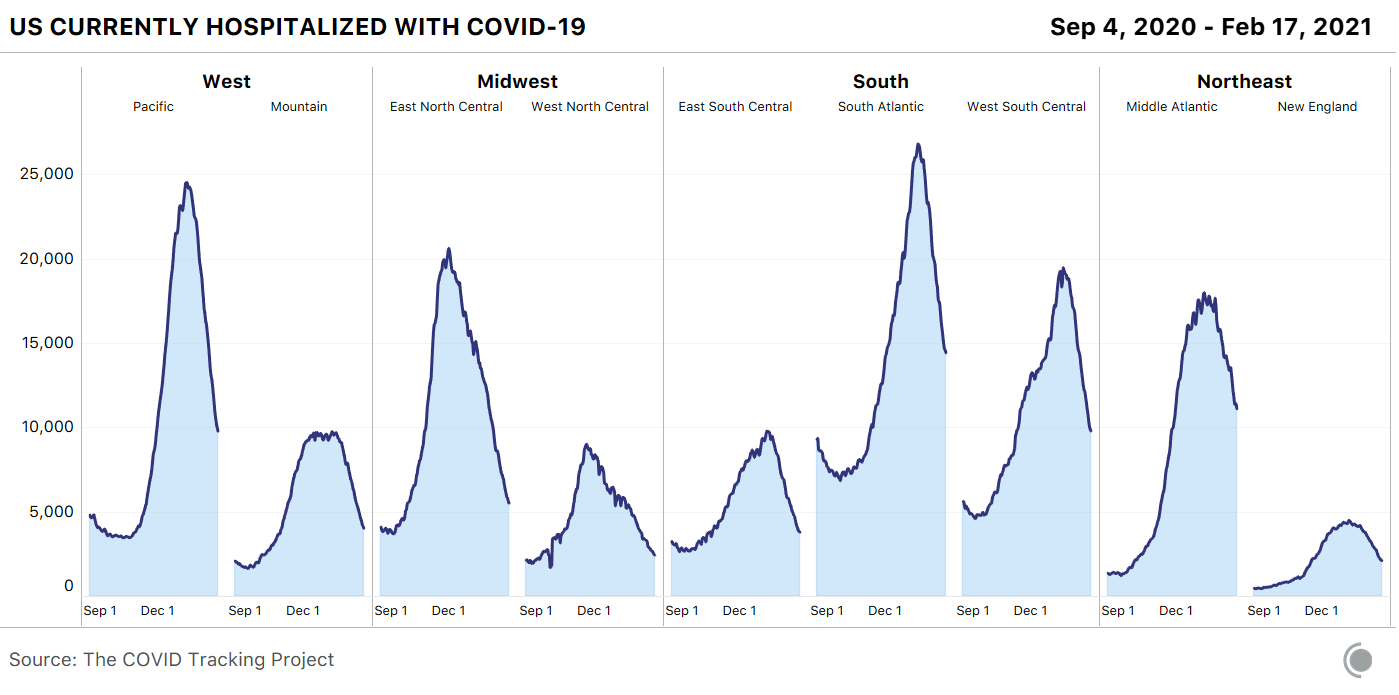
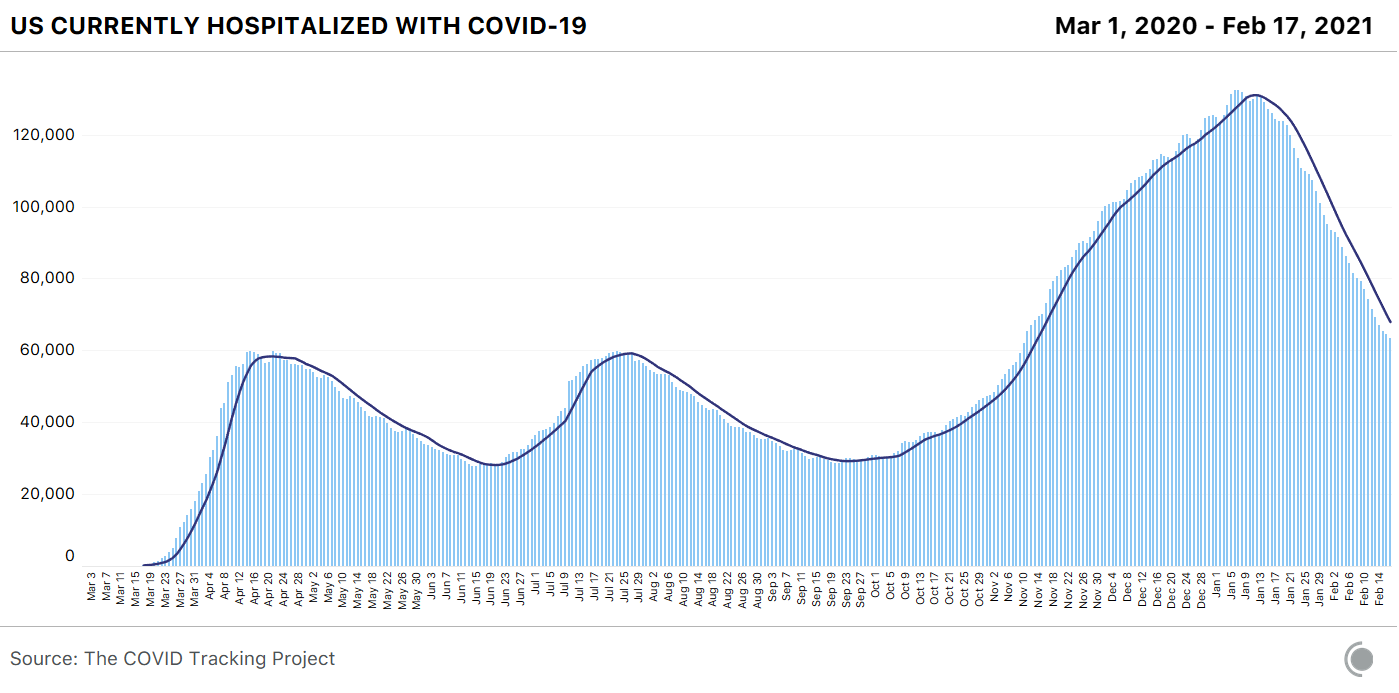
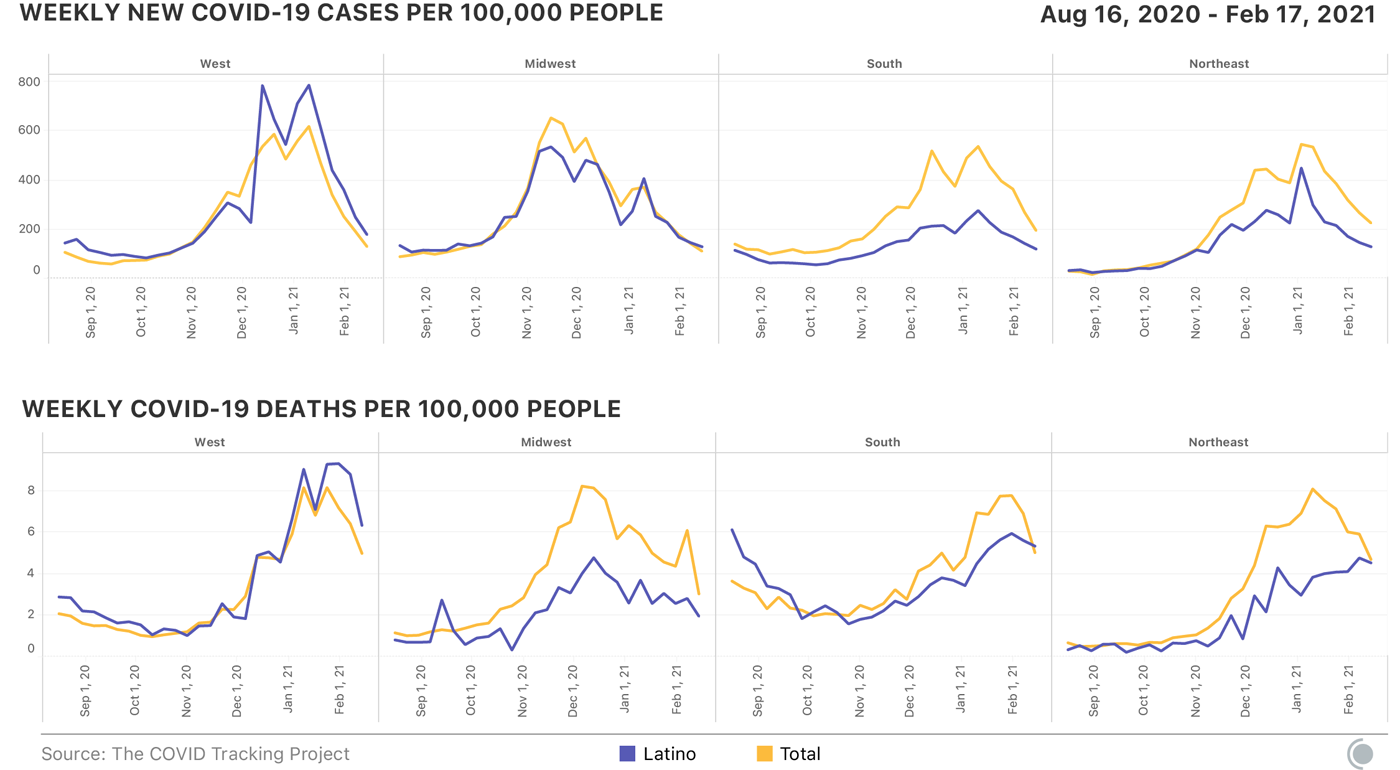
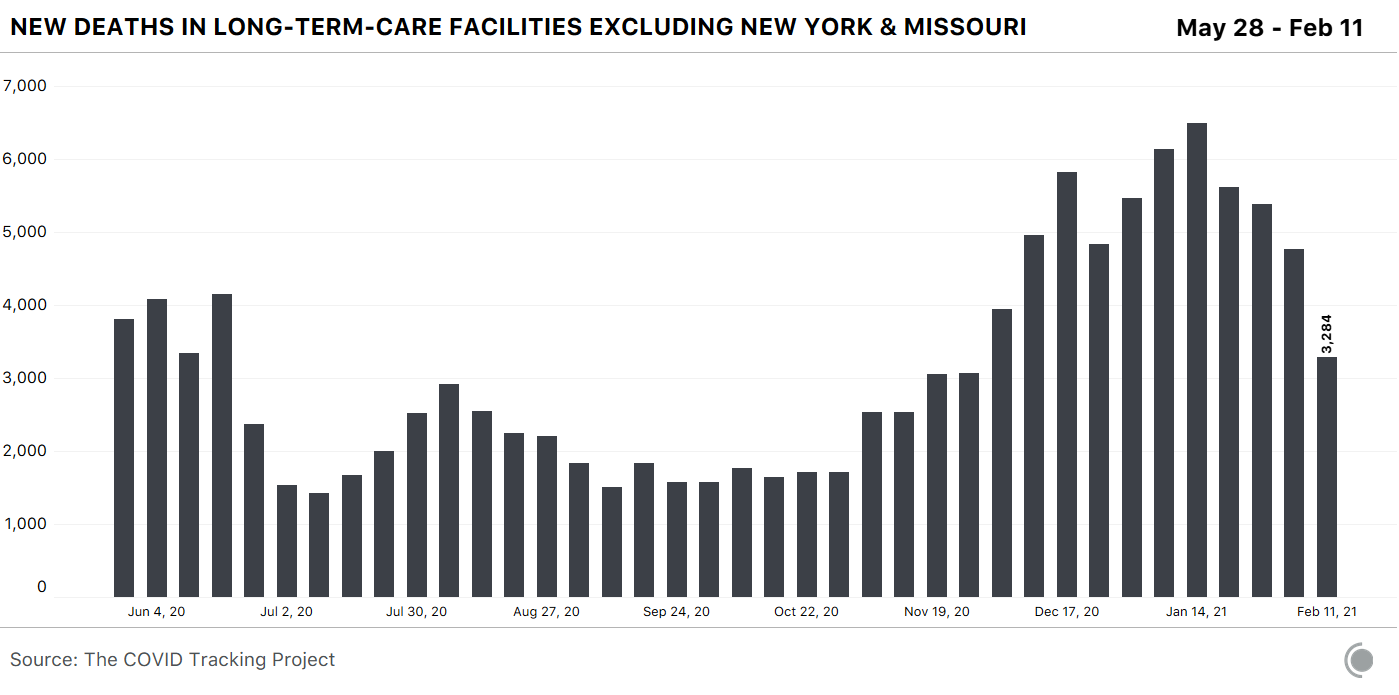
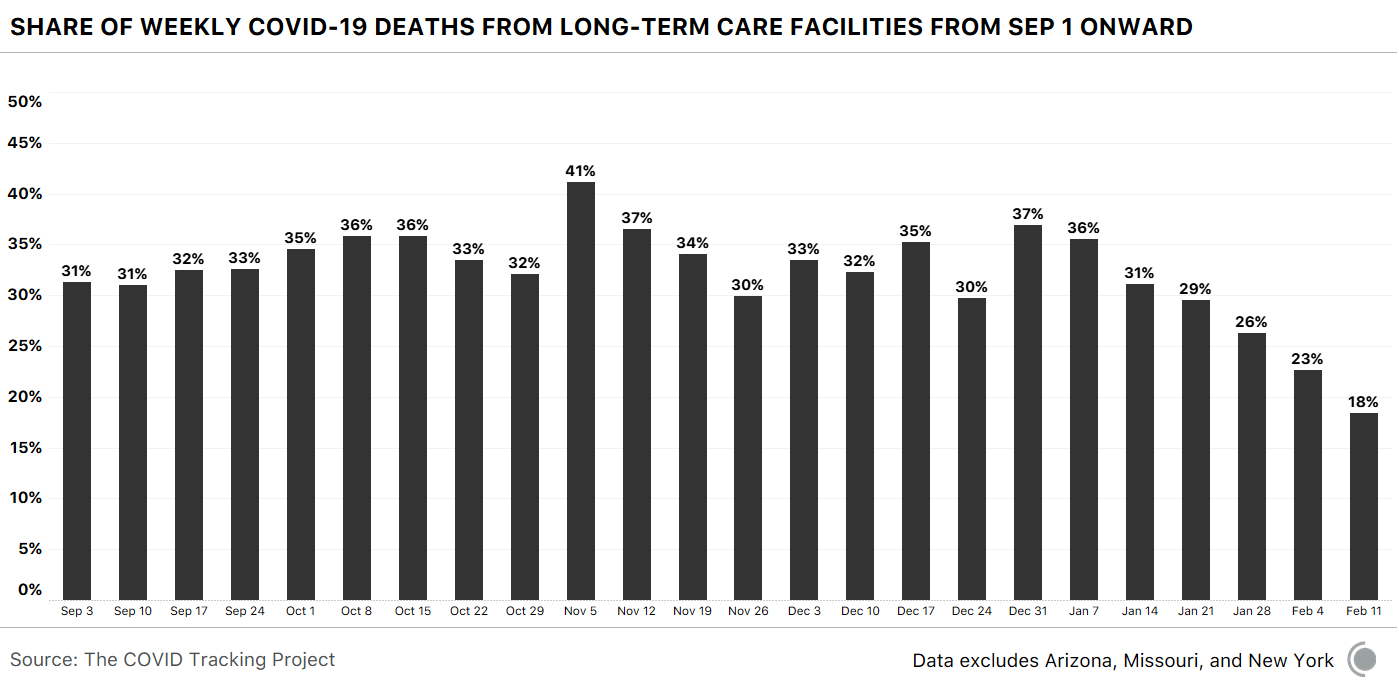
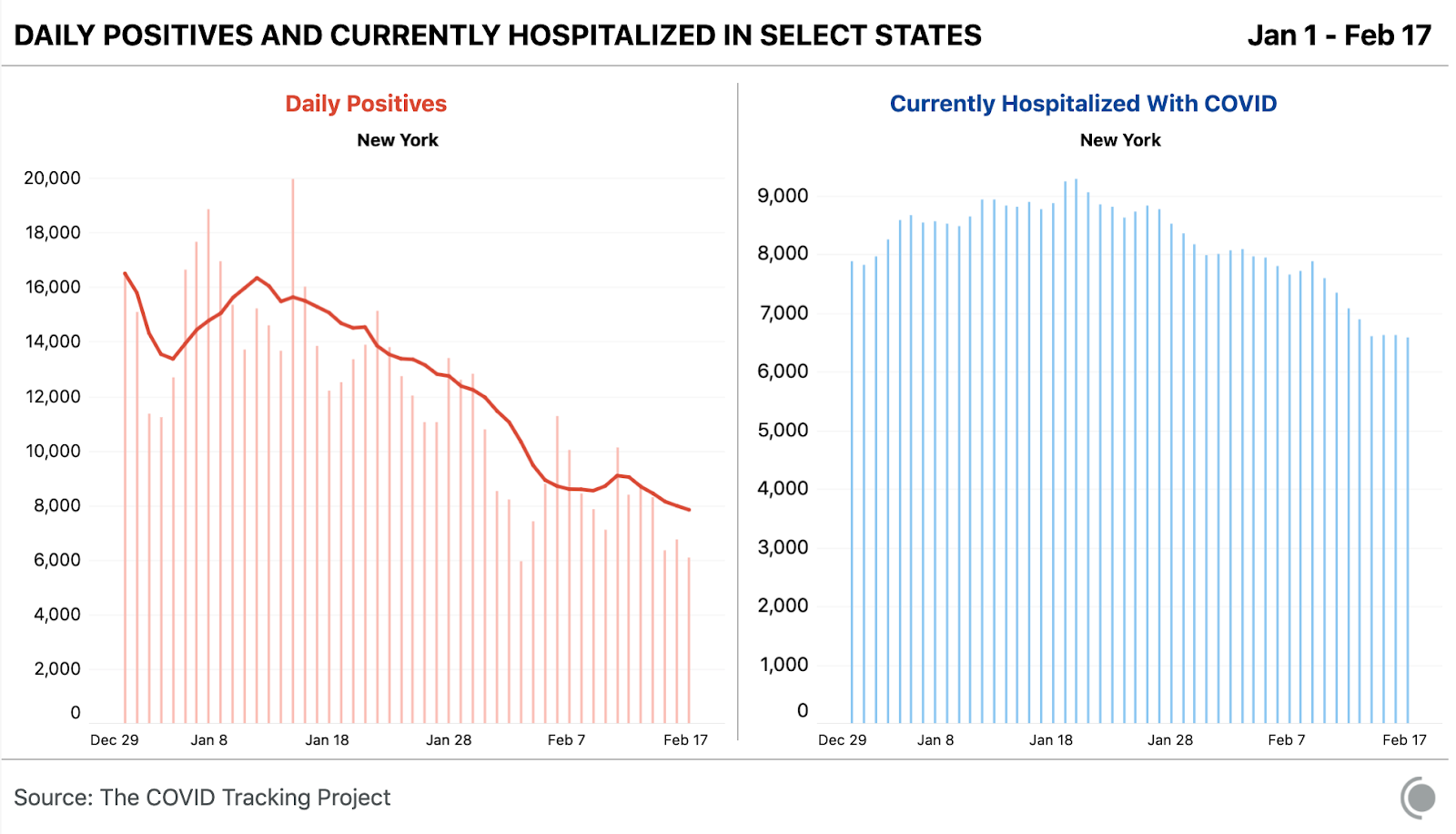
 RSS Feed
RSS Feed
