|
Two months into the pandemic, I gave in and tried Zoom dating. After a few days of chatting on OKCupid, I found myself across the screen from a perfectly nice match. It was one hour in hell: Trapped in a two-way-hostage video, I was hyperaware of everything that was missing—the smell of her perfume, how she moved through space, seeing the way she ordered a drink. If I was going to date, it had to be in person. But for me, that requires endless considerations to make sure I’m not putting myself at risk. Restaurants were out of the question. I thought about outdoor dining, but just how safe is sitting in a sidewalk cafeteria full of strangers? In August, I met a first date in the park and we balanced canned cocktails on the grass between us, estimating for six feet. It was nice and normal enough, something one of us might have thought up even before the pandemic. But whether we were doing the right thing, I had no idea. I have complex cardiac disease, a series of intersecting heart defects and circulation issues that puts me at a far higher risk from the virus than nearly all other 27-year-olds: If I am hospitalized with COVID-19, my risk of death is somewhere between 25 percent and a coin toss. The illness robbed me of a youth spent tangled up in back seats and kissing under the bleachers, so my 20s have served as a deferred adolescence, in which I’m finding my way through casual dating for the first time. Even during a global pandemic, I can’t bear to defer that again. Everyone has to account for the risks of pandemic romance, at least in theory. Early on, local health departments recommended work-arounds to sex, such as masturbating together across a room, that amounted to comedy as much as abstinence. And as is the case whenever any kind of abstinence is preached, young people have still been dating and having sex during all of this. But the young and sick are playing a different game altogether. Many people in their 20s or 30s who live with chronic or terminal conditions experience sickness as both a permanent and transitory state: We may or may not be actively, critically ill at any given moment, but we’re still living with underlying conditions that can mark every aspect of our lives. We’re stuck between two impulses: the need to be as cautious as elderly people and the urge to act our age. The constant balancing act can make dating unbelievably difficult, especially now, but it also fundamentally changes how we think about romance: If anyone understands just how important love is, it’s us. [Read: I took the risk of dating during the pandemic. It paid off.] Many young, sick people have spent years, if not their whole life, wading in the waters of restriction. For some, close contact has always been a hazard; for others, hospitalizations burn up whatever free time might go toward dating. And even for those who are able to date, disclosing an ailment to a partner can be awkward and thorny. Some of us were just gathering momentum after years of an underdeveloped social life before the pandemic introduced a frustrating new layer of restrictions. “I have definitely had plenty of days during COVID where it’s like, Wow, did this catastrophic public-health event maybe just seal my fate as somebody who is not going to meet someone?” Callie, a 26-year-old grad student from Maryland, told me. (Callie, a heart-transplant recipient, asked to be identified by only her first name to protect her privacy.) Because of her illness, she didn’t really start casually dating until a few years ago, and she’s sharply aware that the pandemic has delayed her love life once again. She’s chosen not to date during the past year for fear of what the coronavirus might do to her. “I don’t want to add anything else to the pile of shit that is my body dysfunction,” she said. Since young, sick people have experienced restrictions before, many of us are skilled at making calculations to maintain some version of autonomy in the face of all the risk. “You grow really good at adapting and establishing new normals,” says Kendall Ciesemier, a 27-year-old liver-transplant recipient who lives in Brooklyn. During the summer, she experimented with going on dates at restaurants with outdoor seating, but her prospects never panned out. In the fall, Ciesemier got sick (not with COVID-19) and temporarily moved back in with her parents in Chicago, but over the winter, she started seeing someone new. So far, all of their encounters have been over Zoom or FaceTime because he lives in New York, but Ciesemier will soon be fully vaccinated, and so will the person she’s been not-exactly-dating for the past few months, bringing closer the possibility that they might meet in person. This is typical of life with a serious, chronic illness: Barriers can be real and frustrating, but also manageable. Emily Barker, a 28-year-old based in Los Angeles, lives with paraplegia and an inflammatory condition that requires them to take immunosuppressant drugs. “I’ve already been doing kind of COVID-safe dating, regardless of COVID,” Barker, who uses they/them pronouns, told me. They were already wearing a mask in much of their daily life before the pandemic and taking precautions like asking for a potential partner’s sexual-health tests. After recently getting out of a relationship, Barker’s dating again with even more rules: They make sure that a potential date has been quarantining and has tested negative for the virus before they meet—and ideally they’ll be vaccinated. But rather than keeping Barker from dating, these measures are easy enough for them to factor in. “I’m a huge romantic,” Barker said. “Being in a wheelchair has not stopped me from participating in relationships and sex.” Having to be more intentional about dating can sometimes serve as a perverse kind of benefit. After a few more park dates in the fall, I could tell that things were plateauing with the person I was seeing. After a month and a half, we hadn’t yet kissed, and generally tried to stay at an arm’s length whenever we saw each other. The company was nice and all, but if we weren’t going to pass that threshold, then what exactly were we doing here? We discussed the subject in circles, and I assumed the decision to kiss or have sex would feel sterile, that it might wring all romance out of the encounter. Instead, I found everything suddenly charged and exciting. Acknowledging the risks made everything we did undeniably hotter. [Read: What the pandemic has done for dating] I asked Richard Schwartz, a psychiatrist at McLean Hospital in Massachusetts who studies loneliness and social connection, what he made of the different ways people calculate risk when pandemic dating. “The central love story through all of human history is someone risking life and limb, either to find their beloved or to rejoin their beloved,” he told me. Even though “risking a virus doesn’t have a swashbuckling feeling to it,” he said, the infusion of risk still has an appeal. Many aspects of life during the pandemic have mimicked experiences already common to those living with illness, including extended periods of isolation, the failures of the medical system, and the need to reconsider how love functions in our lives. The fear and excitement of risk follow us everywhere, infusing not just dating but all daily joys with greater stakes. Surviving serious illness is often a negotiation between doing what’s necessary to stay alive and maintaining enough of yourself that the life you’re protecting is still worth living. While love and sex are essential for most people, for the ill, romance can be a way of refusing to let the mere saving of your life be the end in and of itself. Deprivation has given many of us a special understanding of the value that love contributes to life. Since my date and I escalated things, we’ve made sure to contain our risk to ourselves as much as possible. We’re mostly seeing each other inside our own apartments or sitting outside at cafés when the weather is nice enough, and we have a policy of getting tested before we go on a date and being open about our other human contact until we’re both fully vaccinated. Still, I know that all of these protocols don’t cut my risk to zero. Dating through the maze of risk is challenging, but it can also be liberating and fortifying. Even when sickness intrudes, I’m reminded that I’m still alive. from https://ift.tt/31agqMj Check out http://natthash.tumblr.com
0 Comments
It’s official: America’s vaccine-supply crunch is over. The U.S. has ordered, optioned, or procured enough doses to immunize every single member of the population more than five times over, and all adults will be eligible for the shots by May 1. In other words, after months of careful rationing and distribution snafus, we’ve finally hit a new phase of the pandemic endgame: vaccines galore. Next we must confront a more pernicious problem than one of mere logistics: There’s plenty of supply, but what about demand? The worry that significant numbers of Americans might end up refusing a safe, effective, and available COVID-19 vaccine has been salient from the start: Just a few months into the pandemic, pollsters warned that less than half of American adults were sure to take one. But as long as these vaccines were either in development or scarce, this was a hypothetical scenario. Now, at last, our hesitancy will be tested. The outlook, at the moment, is mixed. Americans’ overall acceptance of the vaccines seems to have increased in recent months, as some of those who said in 2020 that they’d wait and see have now waited, seen, and drifted into yes. When you consider all the polls together, about 60 percent of Americans are apparently planning to be immunized, if they haven’t been already. But the remainder—a roughly even split of refuseniks and the undecided—isn’t shrinking at the rate we might have hoped. More alarming are reports of a gaping, and growing, partisan divide. A poll this month from NPR, PBS NewsHour, and Marist found that 87 percent of registered Democrats had either received a vaccine or planned to get one, compared with just 56 percent of registered Republicans. Similar spreads—of 25 to 30 points—have shown up in several other surveys too, and the size of the partisan gap appears to have increased by half since the fall. Donald Trump, who has said little on this topic since leaving office, finally appealed to his supporters on Fox News last week: It’s a great and safe vaccine, he said. “I would recommend it, and I would recommend it to a lot of people that don’t want to get it—and a lot of those people voted for me, frankly.” Yes, let’s be frank: If vaccine acceptance tops out where it is right now, at less than two-thirds of American adults, then the pathway out of this pandemic could stretch and twist into the future. The virus will remain among us, if defanged for many, and harmful outbreaks could emerge as antibody levels fade. If patterns of refusal continue to develop along partisan lines, our outlook will be even worse. Because Republicans and Democrats tend to cluster in different places, even down to the level of neighborhood, a large partisan gap in vaccine uptake would likely lead to hot spots of infection. (When people who refuse a vaccine live near one another, the risk goes up.) But a better outcome also seems well within our reach. Although no one knows how much immunity would be enough to make the disease go away, Anthony Fauci has lately said, “If you want our society to get back to normal, you have to get about 70 to 85 percent of the population vaccinated.” [Read: What if we never reach herd immunity?] So the coming months will be dispositive. An undecided segment of Americans—vaccine swing voters, who now make up roughly 20 percent of all adults—have enormous power to determine how this goes. Which way will they break? A funny fact about vaccines in America is that public attitudes about them rarely change much. For all the Sturm und Drang in recent years about the spread of anti-vaxxer sentiment, and for all the worry about measles coming back, routine childhood-vaccination rates have barely shifted. For more than 20 years now, the proportion of kids younger than 3 who have received a measles-mumps-rubella, or MMR, vaccine has wavered back and forth in a slender band of 91 to 92 percent. That’s to some extent a product of our pediatric care, and public-school rules: Vaccinating children on the normal schedule remains parents’ path of least resistance, any other motivations notwithstanding. But even when the system isn’t pushing quite so hard, vaccination rates are pretty stable: The number of people who get the flu shot, for example, doesn’t change much from year to year, even as flu strains vary in their virulence. Among elderly Americans, the people most at risk of death from influenza, vaccine coverage landed somewhere between 60 and 70 percent in every single year from 1995 to 2020. I say that this is a funny fact about vaccines because one can find it equally consoling and alarming. It’s nice to know that the rise of Andrew Wakefield—whose (since retracted) research linking the MMR vaccine to autism spawned a generation of anti-vaccine activists—caused only a tiny divot in measles-vaccination rates in the U.S. It’s less reassuring that all the righteous work that followed—from anti-anti-vaccination groups on social media, from state legislators, and from many others—hasn’t done that much to move the baseline either. It’s altogether possible—maybe even likely—that Americans’ attitudes toward COVID-19 vaccines are stuck in the same molasses. It’s true that certain periodic polls in recent months have shown a shift toward more acceptance. But polls with longer trails of data, the ones that started before the fall, suggest a different story: They show a dip in vaccine confidence as the election neared, which has since leveled out. Case in point: Gallup had yes at 66 percent in July, which slipped down to 50 percent at the end of September, and then bounced back to 71 percent in January. That autumn fade makes sense, given what occurred in the lead-up to Election Day. Trump had promised to deliver a vaccine just in time for voting, and said that he was “rushing it” along. As that deadline neared, his administration all but went to war against the “deep state” actors at the FDA, installing hacks and hall monitors along the way. On October 7, in a televised vice-presidential debate, Kamala Harris told the nation, “If the doctors tell us that we should take [the vaccine], I’ll be the first in line … But if Donald Trump tells us that we should take it, I’m not taking it.” Naturally, Americans’ faith in any future COVID-19 vaccine went into a slide. Public-health experts warned (against the evidence, as they often do) that this loss of confidence would be long-lasting and profound. But the polling shows that it wasn’t. The dangerous “fever of distrust,” as Ezekiel Emanuel described it, didn’t last much longer than the fall foliage: By midwinter, the polling numbers had returned to roughly what they’d been. The same pattern applies to the partisan split about vaccines. The gap between Trump and Biden voters has widened in the past few months, but it may not be any bigger today than it was last summer. When the Trump administration signaled a willingness to mess with the FDA’s decision making, Democrats panicked most. As the election approached, their vaccine enthusiasm collapsed to the levels seen among Republicans. Gallup had the spread between the two groups at 37 points in July, four in September, and then 40 in January. All of which is to say that COVID-19-vaccine attitudes right now are not that far off from where they started back in 2020, and any hopeful signs of movement in the past few months could be nothing more than bounce-back from the fall. Vaccine-acceptance rates are typically stagnant, but that doesn’t mean they’re stuck in place. It’s often said that more people would get their flu shots if they only grasped the toll of the disease. The deaths caused by influenza—tens of thousands in the U.S. every year—are usually invisible, so much so that the risk is misperceived. For COVID-19, though, the cost is counted every day. When it nears a big, round number--10,000, or 100,000, or 200,000, or 400,000, or half a million—front-page headlines follow. This transparency alone might sway the vaccine-hesitant. So too could the thought of returning to a semblance of one’s former life. Get a COVID-19 vaccine, and you can hug your parents: No other vaccination has this perk. As distribution centers open up to all adults, and more people get their shots, even just the idea of getting immunized could spread through social networks as its own happy contagion, bringing up acceptance rates. “The thing that works best for getting vaccinated is that it gets normalized,” says Maya Goldenberg, a philosopher of science at the University of Guelph, in Ontario, Canada, and the author of a new book, Vaccine Hesitancy: Public Trust, Expertise, and the War on Science. “When vaccination becomes the norm, most people will do it unless they have a really strong inclination not to.” What might that mean in practice? At the moment, one-fourth of all adults have already gotten at least one dose of their vaccine. Another 35 to 40 percent say they plan to get vaccinated as soon as they can, and about 20 percent are now at maybe. Goldenberg told me that we shouldn’t think of this latter group as being truly undecided. “We know that a lot of people are saying ‘I want to get it, but I don’t want to be first in line.’ Does that count as vaccine-hesitant? I’m inclined to say no.” So even if the nevers never budge, it’s certainly possible that in the next few months, amid the vaccination saturnalia, nearly all the nation’s maybes will come around. In that case, we’ll end up with 80 percent of all adults having their vaccination cards filled out or making their appointments—right in Fauci’s sweet spot for herd immunity. Of course, another problem should be considered here: It’s one thing to say you want to get vaccinated, and another thing to do it. (SARS-CoV-2 antibodies, as the saying goes, don’t care about your feelings.) Past research shows that the pipeline from vaccine intentions to behavior can be somewhat leaky. Consider our efforts to address the previous pandemic, of the H1N1 swine flu in 2009. Then, as now, Americans varied widely in their estimations of the disease’s severity, and in how much they trusted the vaccine: A Pew Research poll conducted that October found that 64 percent of Democrats were ready to be immunized, compared with 43 percent of Republicans, and overall, half of American adults said that they planned to get the shot. By June 2010, only 27 percent said they’d actually done so. A somewhat milder attrition rate has been identified in small-scale research. Two very modest flu-shot studies, conducted at Rutgers University and among health-care workers in the Netherlands, compared vaccine intentions to behavior and found that about one-quarter of people who say they plan to be immunized fail to follow through. For the sake of argument, if we apply that rate to all the people who now say they’re yes or maybe on the COVID-19 vaccine, and then add the rest to the group of people who have gotten it already, the total coverage would come out to roughly 65 percent. That projection lands us close to where we’ve been for flu vaccines among the nation’s seniors. That makes a certain amount of sense: Daniel Salmon, the director of the Institute for Vaccine Safety at Johns Hopkins Bloomberg School of Public Health, told me that he’s seen overlapping attitudes toward flu shots and the COVID-19 vaccine, both in surveys and in community meetings. The reasons people give for being wary are the same: They’re worried about adverse effects, he said, and don’t trust the government. Salmon’s team has also found that people are much more likely to say they’ll get the COVID-19 vaccine in 2021 if they’ve had a flu shot in the past. Flu-shot rates did go up this year, at least a bit: For the 2020–21 season, coverage reached 82 percent for seniors, up by almost seven points from the year before. But even those gently boosted numbers would be dire for the COVID-19 vaccine. “We need 70 to 80 percent of people to be immune, homogeneous throughout the population,” Salmon told me. Kids younger than 16 aren’t eligible for COVID-19 vaccination (at least for now), so that means coverage must be even higher for adults in order for the country to reach that threshold. “I’m worried that we’re going to make a dent in disease transmission,” Salmon said, “but that it won’t be enough.” Soon we’ll have a surplus of injections, and then a dearth of upper arms. If the maybes don’t turn out en masse—if in the coming months they fail to make their way to yes—there won’t be any simple finish to this crisis. Without their votes for vaccination, a miserable uncertainty will linger. Deaths could reach their next round headline number. The polls are opening across America. It’s time to watch the needle. from https://ift.tt/3dcGPPl Check out http://natthash.tumblr.com Ruby Martinez was eating a banana when she noticed the nothingness. She chewed but tasted no sweetness. She sniffed but got none of the fruit’s redolent musk. “I started freaking out,” she says. She smelled a bottle of perfume. Nothing. She ate a pickle. Still nothing. That was in June. Since then, her senses of smell and taste have started to come back—but intermittently and in strange ways. There were the two weeks in the summer when all she could smell was phantom smoke. The odor was so strong that she woke up one morning startled, convinced that something in her house was on fire. Sometime later, she was able to smell her boyfriend’s cologne again—but instead of the familiar scent she had always loved, it was a sickening chemical odor. There’s also the hand soap at work, which used to smell generically fruity to her but now smells exactly, and eerily, like Burger King Whoppers. Martinez used to love Whoppers, but she can’t stand the smell of the soap. Her co-workers find her predicament weird and frankly a little funny. “I’m like, ‘I know! What the heck?’” she told me. “Why does it smell like that? Why can’t it be something good?” Despite these bizarre, lingering sensations, Martinez’s taste and smell have continued to recover. Last month, she went back to her favorite restaurant, Saltgrass, to eat her favorite food, steak, and “it was so good,” she said. Her sense of smell has further improved since then, and she can’t wait to return for another steak. Martinez, who is 23 and lives outside Houston, credits the gradual improvement to dedicated “smell training,” a once-obscure protocol that has gained new prominence with COVID-19-associated smell loss. (Martinez doesn’t know whether she had COVID-19, but she was sick right before her smell disappeared.) Many years before the emergence of the novel coronavirus, a German doctor helped develop and standardize smell training for patients who had lost the sense, typically because of head trauma or viral infections. It involves sniffing four essential oils for 20 seconds every day over several months; some proponents of smell training recommend that patients recall memories associated with each scent—remembering lemon pie while smelling lemon oil, for instance. While supposed “cures” for smell loss, such as eating a charred orange or poking your forehead while getting flicked in the back of the head, have gone viral on TikTok, smell training is the only scientifically proven intervention for this kind of smell loss. Nasal congestion and inflammation—as with common colds—often cause some loss of smell, but what happened to Martinez, and to many COVID-19 patients, is markedly different. Their noses are no longer congested nor inflamed, but they still can’t smell a thing. The exact cause is unknown. In the past year, COVID-19 has drawn much more attention to smell loss, also known as anosmia, as well as to the strange ways smell is regained. Some patients go through a period of phantosmia, in which they experience phantom smells, or parosmia, in which they experience distorted smells—like Martinez’s smoke and Whoppers. These odors are quite foul, for reasons that are poorly understood; people find it extremely distressing to drink coffee that smells of sewage or to come out of the shower smelling like trash. “It’s worse than not being able to smell,” says Pamela Dalton, a cognitive psychologist at the Monell Chemical Senses Center. In most cases, the conditions are temporary. But the process of relearning to smell is as mysterious to us as how we lose it. In the 1980s, a scientist at Monell named Charles Wysocki was studying androstenone, a pheromone found in the saliva of male pigs. (Commercially, it’s known as Boarmate.) To Wysocki, at first, the androstenone was odorless. But over time, he started noticing that he could pick out the androstenone bottles in his lab by their distinctly musky scent. Could other people learn to smell it too, he wondered? He found 20 volunteers who also could not initially detect androstenone, and after six weeks of sniffing the pheromone for three minutes, three times a day, half of them became sensitive to the molecule. This finding is in some ways intuitive; the olfactory senses of perfumers and sommeliers, after all, become more attuned to perfumes and wine with time. But it was not until 2009 that Thomas Hummel, an ear, nose, and throat doctor at the University of Dresden, tested a standardized smell-training protocol in the lab. He and his colleagues asked 40 people with anosmia to sniff four essential oils—rose, lemon, eucalyptus, and clove—twice a day for 10 seconds each. After 12 weeks, the volunteers who’d adhered to the smell training regained some of their smell; those in a control group did not. But not everyone who did the smell training improved, and those who did improve didn’t necessarily fully recover. “It’s not a wonder drug,” Hummel told me, “but it helps to increase function faster.” Smell training is less like a cure than like physical therapy for the nose. Since then, Hummel and his colleagues have tested variations of the smell-training protocol: using more complex scents, using a new set of scents every two months, and adding a picture of an object with the appropriate scent. None has much improved on the original. Many people who encounter smell training do so through a charity in the U.K. called AbScent. AbScent’s founder, Chrissi Kelly, lost her sense of smell for the first time after a viral infection in 2012. When her doctor suggested smell training, she found little useful information: The studies that existed had been written for other scientists, not patients. So Kelly began writing down her own tips, such as putting drops of the essential oils in a small jar so the scent blooms like that of wine in a wine glass. Kelly says almost any substance with a scent can theoretically be used for training—calamine lotion, hand soap. But people find that beginning with a standardized guide is helpful, so the protocol on AbScent’s website suggests using the four scents from Hummel’s study. “There’s so much anxiety associated with smell loss,” Kelly told me. “Getting it right and doing it the right way is really, really important to people.” Anosmia is associated with depression, loss of appetite, and diminished quality of life, but it’s also an invisible and underappreciated phenomenon. So Kelly started a Facebook group where people with anosmia could connect. When COVID-19 pandemic began, membership in the group took off; she could almost track the global spread of COVID-19 based on the locations of new members. Kelly eventually created another group just for COVID-19 patients, which now has 25,000 members. Some COVID-19 patients also lose their sense of taste, as Ruby Martinez did; others lose their ability to sense mintiness or spiciness, which are chemical sensations distinct from pure smell or taste. But smell loss seems to be the most common sensory disruption associated with COVID-19. Kelly’s smell got quite good after smell training but in April, she got COVID-19, and lost her sense of smell for the second time. She’s now going through the process again. Unfortunately, she’s still experiencing terrible parosmia. “I’m of course very sad for the second loss of my sense of smell,” she said. “But I’m not giving up. I don’t think that it’s implausible that it will once again come back.” Research on how this coronavirus attacks the olfactory system is beginning to emerge. In July, a team led by Sandeep Robert Datta, a neurobiologist at Harvard, published a paper suggesting that the virus does not directly infect smell-receptor neurons in the nose. Instead, the virus is probably infecting support cells in the olfactory system, which normally help replenish the supply of smell-receptor neurons. COVID-19 infection might interrupt this replenishment, leading to sudden but usually temporary smell loss. Infection of the support cells may also help explain the parosmia that people find especially distressing. When the smell-receptor neurons do finally regenerate, they have to find their way up the nasal cavity, through tiny holes in the base of the skull, and finally to the right structures in the olfactory bulb. “That is an error-prone process,” Datta told me. Humans have only 400 distinct smell receptors, but can distinguish potentially 1 trillion different odors. That’s because a single molecule can bind to multiple smell receptors, and one recognizable scent can be made up of hundreds of different molecules that together activate a unique combination of receptors. If some receptors are missing or miswired, the brain might get a scrambled signal that results in parosmia. The miswiring normally gets sorted out after several weeks or months. “But to be honest, I think there are many things about parosmia we simply don’t understand yet that suggest that more complicated things are going on,” Datta said. For one, why are the scents associated with parosmia usually so foul? The exact smell is “impossible to describe,” Kelly said, but people almost always grasp for words that evoke disgust: sewage, rotten, putrid. In parosmia, Hummel hypothesizes that the brain is interpreting unfamiliar, scrambled signals from miswired olfactory neurons as danger. “Why should something you’ve never smelled before be pleasant?” he says. In our evolutionary history, smells like smoke or rot have often acted as warnings. Strangely enough, though, babies do not seem to have a natural aversion to bad smells. They certainly react to bad tastes or irritants, but they don’t turn their heads away from foul odors. “When they’re very young, their diapers do not disgust them,” Dalton, the psychologist at Monell Chemical Senses Center, notes. The aversion to certain smells seems to be learned over a lifetime, but once we’ve learned it, the reaction is very strong indeed. The connections among smell, emotion, and memory are apparent in our neurobiology, too. Smell-receptor neurons converge on the olfactory bulb, which then sends signals to be processed by the olfactory cortex. But the olfactory bulb is also connected to the amygdala, which is involved in emotions and memory, and the hippocampus, which is also important in memory. “When you smell something, it drives activity in all these areas, and all of these areas talk to each other,” Datta said. “The way your olfactory cortex understands odors depends at least in part on your memories of the odors.” How a particular scent is represented in the brain remains an unsolved mystery. Neurobiologists are able to quantify visual or audio cues, but mapping the relationship between smells is a lot more complicated. Certain smells are definitely related to one another—lemon and lime seem to activate overlapping sets of neurons in the brain, for instance—but scale that to billions of potentially smellable molecules, and mapping them quickly gets impossible. What’s clear is that the experience of smell is not simply what your nose detects but what your brain interprets. It is top-down as well as bottom-up. What you’re actively paying attention to—or not—will determine how you smell. We all get used to the smell of our own house. But we can also learn, as sommeliers do and the pig-hormone sniffers did, to pick out specific scents. This is why smell training is not just passive sniffing. “It’s a process that really needs to take their concentration,” says Sunthosh Kumar Sivam, Ruby Martinez’s ENT doctor at Baylor College of Medicine. After Sivam suggested smell training, Martinez’s boyfriend took her straight to Whole Foods to pick out four essential oils. They followed her doctor’s guidelines for rose and eucalyptus, but swapped lime for lemon and cinnamon for clove. When Martinez does her smell training twice a day, she thinks of her mom’s arroz con leche as she sniffs the cinnamon. She remembers how its scent used to fill the house. Fortunately, she can smell and taste it again. from https://ift.tt/3cWZ8HZ Check out http://natthash.tumblr.com Adapted from The Ten Year War: Obamacare and the Unfinished Crusade for Universal Coverage, St. Martin’s Press 2021. The Affordable Care Act, the health-care law also known as Obamacare, turns 11 years old this week. Somehow, the program has not merely survived the GOP’s decade-long assault. It’s actually getting stronger, thanks to some major upgrades tucked in the COVID-19 relief package that President Joe Biden signed into law earlier this month. The new provisions should enable millions of Americans to get insurance or save money on coverage they already purchase, bolstering the health-care law in precisely the way its architects had always hoped to do. And although the measures are temporary, Biden and his Democratic Party allies have pledged to pass more legislation making the changes permanent. The expansion measures are a remarkable achievement, all the more so because Obamacare’s very survival seemed so improbable just a few years ago, when Donald Trump won the presidency. Wiping the law off the books had become the Republicans’ defining cause, and Trump had pledged to make repeal his first priority. As the reality of his victory set in, almost everybody outside the Obama White House thought the effort would succeed, and almost everybody inside did too. One very curious exception was Jeanne Lambrew, the daughter of a doctor and a nurse from Maine who was serving as the deputy assistant to the president for health policy. As a longtime Obama adviser, going back to the 2008 transition, Lambrew was among a handful of administration officials who had been most responsible for shaping his health-care legislation and shepherding it through Congress—and then for overseeing its implementation. Almost every other top official working on the program had long since left government service for one reason or another. Lambrew had stayed, a policy sentry unwilling to leave her post. On that glum November 2016 day following the election, Lambrew decided to gather some junior staffers in her office and pass out beers, eventually taking an informal survey to see who thought Obama’s signature domestic-policy achievement would still be on the books in a year. Nobody did—except Lambrew. Yes, Republicans had already voted to repeal “Obamacare” several times. But, she knew, they had never done so with real-world consequences, because Obama’s veto had always stood in the way. They’d never had to think through what it would really mean to take insurance away from a hotel housekeeper or an office security guard on Medicaid—or to tell a working mom or dad that, yes, an insurance company could deny coverage for their son’s or daughter’s congenital heart defect. A repeal bill would likely have all of those effects. And although Republicans could try to soften the impact, every adjustment to legislation would force them to sacrifice other priorities, creating angry constituents or interest groups and, eventually, anxious lawmakers. GOP leaders wouldn’t be able to hold the different camps within their caucuses together, Lambrew believed, and the effort would fail. All of those predictions proved correct. And that wasn’t because Lambrew was lucky or just happened to be an optimist. It was because she knew firsthand what most of the Republicans didn’t: Passing big pieces of legislation is a lot harder than it looks. It demands unglamorous, grinding work to figure out the precise contours of rules, spending, and revenue necessary to accomplish your goal. It requires methodical building of alliances, endless negotiations among hostile factions, and making painful compromises on cherished ideals. Most of all, it requires seriousness of purpose—a deep belief that you are working toward some kind of better world—in order to sustain those efforts when the task seems hopeless. Democrats had that sense of mission and went through all of those exercises because they’d spent nearly a century crusading for universal coverage. It was a big reason they were able to pass their once-in-a-generation health-care legislation. Republicans didn’t undertake the same sorts of efforts. Nor did they develop a clear sense of what they were trying to achieve, except to hack away at the welfare state and destroy Obama’s legacy. Those are big reasons their legislation failed. Obamacare’s survival says a lot about the differences between the two parties nowadays, and not just on health care. It’s a sign of how different they have become, in temperament as much as ideology, and why one has shown that it’s capable of governing and the other has nearly forgotten how. Democrats were so serious about health care that they began planning what eventually became the Affordable Care Act more than a decade earlier, following the collapse of Bill Clinton’s reform attempt in the 1990s. The ensuing political backlash, which saw them lose control of both the House and Senate, had left top Democrats in no mood to revisit the issue. But reform’s champions knew that another opportunity would come, because America’s sick health-care system wouldn’t heal itself, and they were determined not to make the same mistakes again. At conferences and private dinners, on chat boards and in academic journals, officials and policy advisers obsessively analyzed what had gone wrong and why—not just in 1993 and 1994 but in the many efforts at universal coverage that had come before. They met with representatives of the health-care industry as well as employers, labor unions, and consumer advocates. Industry lobbyists had helped kill reform since Harry Truman’s day. Now they were sitting down with the champions of reform, creating a group of “strange bedfellows” committed to crafting a reform proposal they could all accept. Out of these parallel efforts, a rough consensus on substance and strategy emerged. Democrats would put forward a plan that minimized disruption of existing insurance arrangements, in order to avoid scaring people with employer coverage, and they would seek to accommodate rather than overpower the health-care industry. The proposal would err on the side of less regulation, spending, and taxes—basically, anything that sounded like “big government”—and Democrats would work to win over at least a few Republicans, because that would probably be necessary in Congress. Proof of concept came in 2006, in Massachusetts, when its Republican governor, Mitt Romney, teamed up with the Democratic state legislature to pass a plan that fit neatly into the new vision. It had the backing from a broad coalition, including insurers and progressive religious organizations. Ted Kennedy, the liberal icon and U.S. senator, played a key role, by helping secure changes in funding from Washington that made the plan possible. “My son said something … ‘When Kennedy and Romney support a piece of legislation, usually one of them hasn’t read it,’” Kennedy joked at the signing ceremony, standing at Romney’s side. Kennedy’s endorsement said a lot about the psychology of Democrats at the time. No figure in American politics was more closely associated with the cause of universal health care and, over the years, he had tried repeatedly to promote plans that looked more like the universal-coverage regimes abroad, with the government providing insurance directly in “single-payer” systems that resembled what today we call “Medicare for All.” But those proposals failed to advance in Congress, and Kennedy frequently expressed regret that, in the early 1970s, negotiations over a more private sector-oriented coverage plan with then-President Richard Nixon had broken down, in part because liberals were holding out for a better deal that never materialized. Kennedy was not alone in his belief that the champions of universal coverage would have to accept big concessions in order to pass legislation. The liberal House Democrats John Dingell, Pete Stark, and Henry Waxman, veteran crusaders for universal coverage who’d accrued vast power over their decades in Congress, were similarly willing to put up with what they considered second-, third-, and even fourth-best solutions—and they were masters of the legislative process, too. Waxman in particular was an expert at doing big things with small political openings, such as inserting seemingly minor adjustments to Medicaid into GOP legislation, expanding the program’s reach over time. “Fifty percent of the social safety net was created by Henry Waxman when no one was looking,” Tom Scully, who ran Medicare and Medicaid for the Bush administration in the early 2000s, once quipped. Obama had a similar experience putting together health-care legislation in the Illinois state legislature—where, despite proclaiming his support for the idea of a single-payer system, he led the fight for coverage expansions and universal coverage by working with Republicans and courting downstate, more conservative voters. He also was a master of policy detail, and as president, when it was time to stitch together legislation from different House and Senate versions, he presided over meetings directly (highly unusual for a president) and got deep into the weeds of particular programs. Obama could do this because the concept of universal coverage fit neatly within his conception of a just society as one in which people act through government to protect themselves from harm. It helped that he had surrounded himself with policy advisers widely recognized as thought leaders in the field of health policy. That included Lambrew and Nancy-Ann DeParle, who had been in charge of Medicare and Medicaid during the Clinton administration, as well as Zeke Emanuel, a physician, bioethicist, and prolific writer on health policy. Peter Orszag, an economist serving as Obama’s budget director, had spent so much time studying ways to reengineer the delivery of health-care services that the prestigious Institute of Medicine elected him as a member. The key Democratic lawmakers had similarly deep benches of seasoned policy advisers. And as the legislative effort got under way in 2009, those advisers were in constant communication with one another and with the White House. There were daily (and sometimes twice-daily) conference calls led by DeParle or Lambrew, in order to coordinate messaging and keep the proposals from diverging too much. Those calls were not always fun, and Lambrew, during her frequent trips to Capitol Hill, usually drew the duty of listening to staff from each chamber vent about the other. But the back-and-forth meant that each committee and chamber understood the absolute limits of what the others could tolerate. Despite all of these conversations and all the preparations that came before them, the journey of the Affordable Care Act through Congress was halting and difficult, and on several occasions the whole project seemed on the verge of failure. Over the course of several months, much of it in lengthy committee hearings, leaders had agreed to a whole new series of compromises, beyond the ones they had made initially—reducing the financial assistance available to insurance buyers, for example, and nixing a “public option” that was supposed to offer a cheaper, government-run alternative, all to keep a majority coalition barely together. These compromises frustrated the champions of reform and would have serious consequences much later, because the deals limited the Affordable Care Act’s ability to make insurance affordable for everyone. But a bill got through Congress and, with the president’s signature, became law. That was no small thing, as Republicans were about to discover. The GOP assault on the Affordable Care Act began officially on March 23, 2010, the same day Obama signed the law, and it took the form of a bill sponsored by Jim DeMint, a Republican senator from South Carolina. He was among the chamber’s most conservative members, once wrote a book warning that liberals were trying to turn America into a socialist country, and frequently attacked more moderate Republicans for supporting ideas that sounded to him like “Democrat lite.” In the summer of 2009, he had riled up Tea Party activists by proclaiming that defeating health-care reform would lead to Obama’s “Waterloo.” That original DeMint bill had just 22 co-sponsors, which was still more than the total number of words in the legislation’s one-sentence text: “The Patient Protection and Affordable Care Act, and the amendments made by that Act, are repealed.” “Repeal and replace” was the party’s official motto, but this bill was all “repeal,” no “replace.” Following the 2010 midterms, and big Republican gains in Congress, DeMint filed a new version of his legislation. This time, every single GOP senator signed on as a co-sponsor. This was an indicator of how much the caucus, and party as a whole, was signaling support for the ultraconservative, anti-government worldview of DeMint. It also revealed how de rigueur a commitment to full, uncompromising repeal had become. But DeMint’s new legislation still had no replacement component. And this was a sign of things to come. Although a handful of conservative intellectuals worked on proposals and although a handful of GOP lawmakers, such as Senator Orrin Hatch of Utah and Representative Tom Price of Georgia, wrote legislation, these proposals never got sustained attention from either GOP leadership or members. Republicans had nothing like the detailed, ongoing discussions with outside advisers and interest groups that Democrats and their allies had undertaken in the years before 2009—a failing that several former Republican officials later recognized with regret. “Obviously, it is the case that there were not enough conversations about ‘replace,’” Brian Blase, a conservative health-policy expert who was a top domestic-policy adviser in the Trump White House, told me. Dean Rosen, a GOP leadership aide from the early 2000s who went on to become one of Washington’s most influential health-care strategists, said, “There was an intellectual simplicity or an intellectual laziness that for Republicans in health care passed for policy development. That bit us in the ass when it came to repeal and replace.” One reason for this laziness was a simple lack of interest. For decades, Republicans had seemed interested in health-care policy only when responding to Democratic policies required it. “Republicans do taxes and national security,” Brendan Buck, a former GOP leadership aide, quipped in an interview. “They don’t do health care.” That ambivalence extended to the GOP’s networks of advisers and advocates. The cadre of Republican intellectuals who worked on health policy would frequently observe that they had very little company, talking about a “wonk gap” with their more liberal counterparts. “There are about 30 times more people on the left that do health policy than on the right,” Blase said. Another problem was a recognition that forging a GOP consensus on replacement would have been difficult because of internal divisions. Some Republicans wanted mainly to downsize the Affordable Care Act, others to undertake a radical transformation in ways they said would create more of an open, competitive market. Still others just wanted to get rid of Obama’s law and didn’t especially care what, if anything, took its place. “The homework that hadn’t been successful was the work to coalesce around a single plan, a single set of specific legislative items that could be supported by most Republicans,” Price told me. “Clearly, looking at the history of this issue, this has always been difficult for us because there are so many different perspectives on what should be done and what ought to be the role of the federal government in health care.” The incentive structure in conservative politics didn’t help, because it rewarded the ability to generate outrage rather than the ability to deliver changes in policy. Power had been shifting more and more to the party’s most extreme and incendiary voices, whose great skill was in landing appearances on Hannity, not providing for their constituents. Never was that more apparent than in 2013, when DeMint, Senator Ted Cruz of Texas, and some House conservatives pushed Republicans into shutting down the government in an attempt to “defund” the Affordable Care Act that even many conservative Republicans understood had no chance of succeeding. The failure to grapple with the complexities of American health care and the difficult politics of enacting any kind of change didn’t really hurt Republicans until they finally got power in 2017 and, for the first time, had to back up their promises of a superior Obamacare alternative with actual policy. Their solution was to minimize public scrutiny, bypassing normal committee hearings so they could hastily write bills in the leadership offices of House Speaker Paul Ryan and, after that, Senate Majority Leader Mitch McConnell. The Republican effort involved nothing remotely like the daily conference calls that the Obama White House had convened with congressional staff. “Looking back, we should have had more coordination and communication,” Emily Murry, who in 2017 was a senior Republican health-care staffer on the Ways and Means Committee, told me. “We should have had weekly meetings, if not more, with the House, Senate, and administration.” And neither Ryan nor McConnell had much experience writing complex legislation—not even McConnell, despite his reputation as a strategic genius. He had distinguished himself though his creative and brazen efforts at obstructionism. But passing bills requires a different skill set than blocking them. Upon releasing legislation, Ryan and McConnell each found themselves in the predicament Jeanne Lambrew had foreseen, whipsawed between more moderate Republicans who thought the legislation tore down too much of the Affordable Care Act and more conservative Republicans who thought it left too much in place. Members hadn’t expected devastating Congressional Budget Office reports projecting that more than 20 million would lose insurance. They hadn’t worked out how to justify those results after so many years of promising better, cheaper health care—something their policies quite plainly did not deliver—and they had no answers for the nearly unanimous condemnations by industry and patient-advocacy groups, with whom Republicans hadn’t negotiated in advance. Trump, who thought of himself as a master negotiator, tried to play the role that Obama had. But Trump’s success in business was mostly at branding, and legislating required workmanship, not showmanship. Trump couldn’t be bothered with legislative details and betrayed no clear sense of mission, except to get a big win and erase Obama’s signature accomplishment from the history books. “He never talked policy,” Charlie Dent, a retired GOP congressman from Pennsylvania, told me later. “It was just, ‘Let’s get this thing done. Let’s get a deal here.’” Telling legislators to “get a deal here” wasn’t an especially effective tactic, and although a bill got through the House, it collapsed in the Senate when John McCain gave a dramatic thumbs-down to a scaled-back, last-gasp piece of “skinny” legislation designed simply to keep the process moving forward. The legislative debate had exposed the GOP, finally, as a party that didn’t have a plan to get more people medical care—and wasn’t especially concerned with trying to find one. The Affordable Care Act now looks as though it’s here to stay, unless the Supreme Court surprises everybody and rules in favor of a far-fetched challenge it heard back in November. And although the same handful of conservative intellectuals are working diligently on policy papers, Republican officials haven’t shown interest in developing those plans into an actionable agenda. Republicans remain focused on, and quite skilled at, delivering outrage to their supporters. They continue to show no enthusiasm for passing laws, on health care or anything else for that matter. Over the past few weeks, as Democrats passed that groundbreaking COVID-19 relief initiative, Republicans have put most of their energy into making arguments about “cancel culture.” And although Democrats are already moving on to other pieces of legislation, including plans for infrastructure, a minimum-wage increase, and immigration reform, the most concrete thing on the Republican agenda is talk of reviving a half-dozen Dr. Seuss books that the late children’s author’s estate stopped printing because they contained racist imagery. Democrats are also talking about next steps on health care—and have been for a while, actually, although they are not all saying the same things. Some want to keep building on the Affordable Care Act incrementally, as the coronavirus-relief legislation did. Others seek much more ambitious changes, up to and including the idea of wiping out existing insurance arrangements so that the government can insure everybody directly through Medicare for All. Some kind of reckoning between those two visions is inevitable. But in the meantime, policy experts and lawmakers are doing precisely what their counterparts were doing in the late 1990s and early 2000s—turning ideas into detailed proposals, with serious accounting estimates, and then writing legislation and attempting to build coalitions with outside groups. All of them remain as dedicated as ever to achieving their longtime goal of universal coverage. Of course, some experts and officials in the Democratic Party are preoccupied with other matters, such as addressing the COVID-19 crisis. It remains the No. 1 priority for the Biden administration and for Jeanne Lambrew, who is back in her home state of Maine, serving as its commissioner of Health and Human Services. Maine has fared relatively well during the pandemic, with one of the lowest per capita death rates in the country. There seems to be no single reason for Maine’s impressive performance, but a generally attentive attitude from leaders and a methodical, data-based approach to solving problems have likely helped. This work is rarely glamorous and gets little attention. But it’s essential to addressing the crisis and making sure the public sector functions properly, which is perhaps why the party that believes in government is so much better at it than the one that doesn’t. from https://ift.tt/317hfFv Check out http://natthash.tumblr.com It’s hard to know when exactly the first cases appeared. But certainly by January’s end, a slow trickle of post-vaccination infections had begun in the United States. They arose in the West, making headlines in Oregon; they sprouted in the Midwest and the South. Some of the latest reports have come out of Florida, Texas, and Hawaii. These breakthrough cases—discovered in people more than two weeks after they received their final COVID-19 shot—will continue to grow in number, everywhere. And that’s absolutely no cause for concern. Breakthrough infections, which occur when fully vaccinated people are infected by the pathogen that their shots were designed to protect against, are an entirely expected part of any vaccination process. They’re the data points that keep vaccines from reaching 100 percent efficacy in trials; they’re simple proof that no inoculation is a perfect preventative. And so far, the ones found after COVID-19 vaccination seem to be unextraordinary. Since mid-December, when the rollout of the newly authorized vaccines began, nearly 40 million Americans have received the jabs they need for full immunization. A vanishingly small percentage of those people have gone on to test positive for the coronavirus. The post-shot sicknesses documented so far seem to be mostly mild, reaffirming the idea that inoculations are powerful weapons against serious disease, hospitalization, and death. This smattering of cases is a hazy portent of our future: Coronavirus infections will continue to occur, even as the masses join the ranks of the inoculated. The goal of vaccination isn’t eradication, but a détente in which humans and viruses coexist, with the risk of disease at a tolerable low. When breakthrough cases do arise, it’s not always clear why. The trio of vaccines now circulating in the United States were all designed around the original coronavirus variant, and seem to be a bit less effective against some newer versions of the virus. These troublesome variants have yet to render any of our current vaccines obsolete. But “the more variants there are, the more concern you have for breakthrough cases,” Saad Omer, a vaccine expert at Yale, told me. The circumstances of exposure to any version of the coronavirus will also make a difference. If vaccinated people are spending time with groups of unvaccinated people in places where the virus is running rampant, that still raises their chance of getting sick. Large doses of the virus can overwhelm the sturdiest of immune defenses, if given the chance. The human side of the equation matters, too. Immunity is not a monolith, and the degree of defense roused by an infection or a vaccine will differ from person to person, even identical twins. Some people might have underlying conditions that hamstring their immune system’s response to vaccination; others might simply, by chance, churn out fewer or less potent antibodies and T cells that can nip a coronavirus infection in the bud. [Read: You’re not fully vaccinated on the day of your last dose] The effects of vaccination are best considered along a spectrum, says Ali Ellebedy, an immunologist at Washington University in St. Louis. An ideal response to vaccination might create an arsenal of immune molecules and cells that can instantaneously squelch the virus, leaving no time for symptoms to appear. But sometimes that front line of fighters is relatively sparse. Should the virus make it through, “it becomes a race [against] time,” Ellebedy told me. The pathogen rushes to copy itself, and the immune system recruits more defenders. The longer the tussle drags on, the more likely the disease is to manifest. The range of vaccine responses “isn’t a variation of two- to threefold; it’s thousands,” Ellebedy told me. “Being vaccinated doesn’t mean you are immune. It means you have a better chance of protection.” For these reasons and more, Viviana Simon, a virologist at the Icahn School of Medicine at Mount Sinai, in New York, dislikes the term breakthrough case, which evokes a barrier walling humans off from disease. “It’s very misleading,” she told me. “It’s like the virus ‘punches’ through our defenses.” Vaccination is actually more like a single variable in a dynamic playing field—a layer of protection, like an umbrella, that might guard better in some situations than others. It could keep a lucky traveler relatively dry in a light drizzle, but in a windy maelstrom that’s whipping heavy droplets every which way, another person might be overwhelmed. And under many circumstances, vaccines are still best paired with safeguards such as masks and distancing—just as rain boots and jackets would help buffer someone in a storm. [Read: People are keeping their vaccines secret] In some ways, the shots’ staggering success in trials—where breakthrough cases were also observed, causing appropriately minimal stir—may have papered over the inevitability of post-vaccination infections in more natural settings. “The vaccines exceeded expectations,” Luciana Borio, a former acting chief scientist at the FDA, told me. Now, as we exit what Borio calls the “honeymoon phase” of our relationship with the jabs, we need to temper our enthusiasm with the right amount of realism, especially as more data on the shots’ strength and longevity accumulate. Even excellent vaccines aren’t foolproof, and they shouldn’t be criticized when they’re not. “We can’t expect it’s going to be perfect, on day one, always,” Borio said. Breakthrough cases also include asymptomatic infections, according to the CDC's current definition—which is different from the criteria on which the vaccines were originally judged. In clinical trials, the three vaccines cleared for emergency use in the United States were evaluated for their ability to prevent symptomatic cases of COVID-19, which they each do to a remarkably high extent. The Moderna and Pfizer-BioNTech jabs reduce, on a population scale, the risk of disease by about 95 percent; Johnson & Johnson’s clocked in at 72 percent among Americans. The numbers for asymptomatic infections are still crystallizing, but they’re likely to be lower. Purging a virus before sickness sets in is a higher bar for the immune system to clear. “The trick is to distinguish between infection and disease,” Simon told me. “Whenever someone tests positive, the real question is, are they sick, and how sick are they? That’s a big difference.” Efficacy, a figure specific to clinical trials, also doesn’t always translate perfectly to the messiness of the real world, where there’s immense variability in how, when, where, by whom, and to whom shots are administered. The vaccine’s performance under these conditions is tracked by a separate measure, called effectiveness. Studies rigorously examining vaccine effectiveness are challenging, but early data suggest that the Pfizer-BioNTech and Moderna shots are living up to their initial hype. [Read: The second COVID-19 vaccine is a rude reawakening for immune cells] The number of post-vaccination infections is also contingent on “the ongoing transmission situation,” Omer told me. “It depends on how much people are mixing.” A vaccine with a recorded efficacy of 95 percent, for example, doesn’t give everyone who’s vaccinated a 5 percent chance of getting sick. Not all of those people will even encounter the virus. The key is how vaccination changes the outcome for those who are meaningfully exposed: Among 100 individuals who might have fallen ill without the vaccine, just five symptomatic cases might appear. A team at the CDC is tracking breakthroughs and will soon start reporting case counts, as well as any patterns related to where, or in whom, these infections are occurring, Martha Sharan, a CDC spokesperson, told me. Details like those matter. They can help experts figure out why post-vaccination infections happen, and how they might be stopped. “The reassuring part is, these cases will not go unnoticed,” Omer told me. Most of the time, vaccines are far more likely to offer some help than none. Serious disease, hospitalization, and even death will still occur, as will less well-studied outcomes, such as the long-term symptoms that often arise from less severe disease. But should post-vaccination infections climb to unexpectedly high rates, backup plans will quickly kick into gear. Some shot recipients might get second or third shots to bolster their immune response; others might be administered a tweaked vaccine recipe to account for a new viral variant. There’s something a touch counterintuitive about breakthrough cases: The more people we vaccinate, the more such cases there will be, in absolute numbers. But the rate at which they appear will also decline, as rising levels of population immunity cut the conduits that the virus needs to travel. People with lackluster responses to vaccines—as well as those who can’t get their jabs—will receive protection from the many millions in whom the shots did work. In a crowd of people holding umbrellas, even those who are empty-handed will stay more dry. from https://ift.tt/3tGurh3 Check out http://natthash.tumblr.com The number of people hospitalized with a confirmed case of COVID-19 in the United States has been plummeting since early January. Until about three weeks ago, hospitalizations in Michigan were following the same pattern: More people with COVID-19 were leaving the hospital than were being admitted. But in the past few weeks, data from the CDC and the Department of Health and Human Services have shown that hospitalizations have risen by 45 percent from the state’s recent low on February 25. According to federal data, among U.S. metropolitan areas with more than 1 million people, the Detroit area now ranks fourth in hospital admissions—and first in a metric that combines increases in test positivity and cases. Throughout the fall and winter, we saw a clear pattern—cases would rise, then hospitalizations about a week later, and finally, two weeks after that, deaths would follow. Nursing homes and other long-term-care facilities reported particularly heavy death tolls. If Michigan were to continue that pattern, we would expect hospitalizations to keep rising, and then more deaths. But as a spring surge takes hold in Michigan, two new factors--variants of concern and rising vaccination levels—mean that we don’t yet know how this new rise in cases and hospitalizations will play out. The vaccination of people 65 and older and of nursing-home residents should blunt the death toll of a rise in cases. But according to state data, Michigan has administered first doses to 61 percent of its residents aged 65–74, and 62 percent of residents 75 and older. Detroit’s figures are much lower: The city has given first doses to only 43 percent of those aged 65–74 and 39 percent of people 75 and older. For comparison, the CDC reports that 66 percent of the U.S. population aged 65 and up has received at least one dose of vaccine. The numbers are even worse for Black people in Michigan: Statewide, just 28 percent of Black residents 65 and older are known to have received at least one dose of vaccine. Overall, Michigan has administered first doses to only about a quarter of its total population, and that number falls to 15 percent in Detroit. The reality of vaccinations in nursing homes remains difficult to understand. The CDC reports that about 182,000 people in nursing homes and other long-term-care facilities have been vaccinated in Michigan through the Federal Pharmacy Partnership, but doesn’t separate resident and staff doses at the state level, making it impossible to derive a percentage of facility residents who have been immunized. According to the Michigan Department of Health and Human Services, COVID-19 cases and deaths in the state’s long-term-care facilities have declined substantially through February and March, and we can hope that this decline holds even as cases and outbreaks emerge around these facilities. As Michigan’s numbers go back up, the obvious next question is to what degree variants of concern are playing a role in this localized surge. Genomic surveillance remains limited in the United States, but from the numbers we do have, it seems as though the variant known as B.1.1.7, first identified in the U.K., is quite widespread in Michigan. In fact, according to the CDC’s tracking, the state of Michigan has the second-most confirmed cases of B.1.1.7 after Florida, despite having less than half the number of residents. Although Michigan’s numbers indisputably show a resurgence of COVID-19, there are troubling signs in other parts of the country. Federal data show that per-capita hospitalizations in the New York area have remained among the highest in the nation. Unlike many other areas of the country, where hospitalizations have fallen close to pre-surge levels, in New York and New Jersey hospitalizations have plateaued for weeks, according to federal data. We are not yet seeing huge upticks, but it’s not a good sign that as many people are being admitted to hospitals as are leaving them. In months past, we might have been able to make educated guesses about what might happen next as the situation worsens in Detroit: We would expect to see cases and hospitalizations increase statewide and also rise elsewhere in the region, as when the Dakotas and Wisconsin acted as sentinels for the deadly third surge of cases over the winter. We would also have seen deaths soar several weeks after cases rose, especially within nursing homes. But Michigan’s surge arrives in a national landscape altered by new viral variants and more than 100 million immune systems strengthened by vaccination. We anticipate that state and federal vaccination efforts will increase in and around Detroit—and across the country—fast enough to prevent a regional or national reversal of our hard-won progress. What the numbers incontrovertibly show, however, is that we’re not going to see COVID-19 immediately disappear. As public-health experts have suggested for months, there will be continuing outbreaks this spring--likely as a result of B.1.1.7 becoming the dominant virus. Now the question is how bad they’ll get and how far they’ll spread. Alexis C. Madrigal, Dave Luo, Peter Walker, Erin Kissane, Jessica Malaty Rivera, and Conor Kelly contributed to this article. from https://ift.tt/3s1Y6kk Check out http://natthash.tumblr.com This has been a year of terrible loss. People have lost loved ones to the pandemic. Many have gotten sick, and some are still suffering. Children have lost a year of school. Millions have lost a steady paycheck. Some have lost small businesses that they’d built for decades. Almost all of us have lost hugs and visits and travel and the joy of gathering together at a favorite restaurant and more. And yet, this year has also taught us much. Strange as it may sound, the coronavirus pandemic has delivered blessings, and it does not diminish our ongoing suffering to acknowledge them. In fact, recognizing them increases the chance that our society may emerge from this ordeal more capable, more agile, and more prepared for the future. Here are three ways the world has changed for the better during this awful year. 1. We Now Know How to Code for Our VaccinesPerhaps the development that will have the most profound implications for future generations is the incredible advances in synthetic messenger RNA (mRNA) biotechnologies. We got our vaccines very fast—the previous record for vaccine development was four years, and that was set in the 1960s. This time, we developed multiple good COVID-19 vaccines in less than a year. Luck bought us some of that speed. For example, the HIV retrovirus is notoriously difficult to vaccinate against, and we still don’t have a vaccine for it. COVID-19 was much more susceptible, and billions of dollars in public money and a global sense of urgency pushed things along. Tragedy also sped things up: Because the pandemic was raging—more cases to test against—it was easier to get results from vaccine trials. But amid all this came historic developments. The new mRNA technology, on which several vaccines—notably Pfizer-BioNTech’s and Moderna’s—are based, is an epochal scientific and technical breakthrough. We are now coding for vaccines, and thanks to advances in science and industrial production, we can mass produce them and figure out how to deliver them into our cells in a matter of months. This is all new. Neither Moderna nor BioNTech had a single approved product on the market before 2020. Each company essentially designed its vaccine on a computer over a weekend in January 2020—BioNTech’s took just a few hours, really. Both companies had vaccine candidates designed at least four weeks before the first confirmed U.S. COVID-19 fatality was announced, and Moderna was producing vaccine batches to be used for its trials more than a month before the World Health Organization declared a pandemic. In 2021, the companies together aim to produce billions of stunningly efficacious vaccine doses, [Read: How science beat the virus] We know the principle behind vaccination: Once our immune system encounters a virus, it can learn how to fight it and remember how to do it the next time. Vaccines give our immune system the practice it needs, but it’s deliberately structured as an unfair fight. Until now, most of our current vaccines have been either weakened or completely deactivated viruses or, more recently, protein subunits: just a few fragments from the virus, called antigens. We’ve achieved extraordinary levels of effectiveness and safety with these techniques, but they still have downsides. In 1955, a botched batch of weakened polio vaccine killed 10 children and caused paralysis in hundreds. We’ve since made sure to never repeat that tragic failure, but producing vaccines from the actual pathogen still means handling the virus in the manufacturing process. The newer subunit vaccines hold a lot of promise, but come with their own challenges. Identifying the right subunit (or antigen) can be difficult, and these vaccines tend to produce weaker immune responses. Plus, it’s not like antigens are hanging out on a supermarket shelf. We grow them in cell systems like yeast or in E. coli--essentially highjacking their genetics to produce the antigens we want, and then harvesting the yield. It works, but it’s slower than the mRNA process. The mRNA vaccines work differently. For these, scientists look at the genetic sequence of a virus, identify a crucial part—such as the spike protein, which it uses as a key to bind onto cells’ receptors in order to unlock and enter them—produce instructions to make just that part, and then send those instructions into our cells. After all, that’s what a virus does: It takes over our cells’ machinery to make more of itself. Except in this case, we instruct our cells to make only the spike portion to give our immune system practice with something that cannot infect us—the rest of the virus isn’t there! Until this year, that was the dream behind the synthetic mRNA technologies: a dream with few, scattered adherents, uphill battles, and nothing to show for it but promise. This year, it became a reality. Our cells have a remarkable kind of software—wetware—that uses the instructions in the DNA in our cells’ nuclei to produce proteins. If you imagine the assembled proteins as a Lego structure, the DNA is like the instruction booklet. But someone has to look at those instructions and put the blocks together in the right way. In the cell, a key part of this process is the messenger RNA: a short-lived, single-strand molecule that carries the instructions from the DNA in the nucleus to the protein-making factory outside it. In 2020, we figured out how to make messenger RNA with precision, by programming the exact code we wanted, producing it at scale (a printing press for messenger RNA!), and figuring out a way to inject it into people so the fragile mRNA makes it into our cells. The first step was pure programming: Uğur Şahin, the CEO of BioNTech, sat at his computer and entered the genetic code of the spike protein of the mysterious virus that had emerged in Wuhan. Moderna employees had done the same thing the weekend after the genomic sequence was released on January 10. The Moderna vaccine candidate was called mRNA-1273 because it encoded all of the 1,273 amino acids in the SARS-CoV-2 spike protein—the code was so small that it could all be represented with little less than half the number of characters that fit on a single-spaced page. The rest of the process relied on key scientific and industrial innovations that are quite recent. Messenger RNA are fragile—they disintegrate easily, as they are supposed to. The lipid nanoparticles we envelop them in to use as delivery systems were approved only in 2018. Plus, the viral spike protein is a notorious shape-shifter. It takes one form before it fuses with our cells and another one afterward. The latter, postfusion form did not work well at all for developing vaccines, and scientists only recently figured out how to stabilize a virus’ spike in its prefusion form. [Read: The second COVID-19 shot is a rude awakening for immune cells] Now that this process is in place, a host of possibilities have opened up. We may soon have vaccines for many other diseases that have eluded our grasp. Efforts are already under way, for example, for an mRNA vaccine for malaria—a parasite that each year kills hundreds of thousands of people, mostly children, and is notoriously hard to vaccinate against. We may also finally get a new set of tools to better fight cancer. (Both Moderna and BioNTech were working on cancer treatments before pivoting to coronavirus vaccines.) The challenge with cancer is that it is our own cells gone awry. It is really difficult to find a way to kill just a patient’s cancer cells thoroughly without also killing healthy cells—and thus the patient. But synthetic mRNA can be encoded with only the specific mutation in one patient’s cancer cells—and if the cancer cells further mutate, those can be targeted as well. This may allow us, finally, to transition from a broadcast-only model of medicine, wherein drugs are meant to be identical for everyone in a particular group, to targeted, individualized therapies. Plus, these technologies are suitable for small-scale but cheap-enough production: a development that can help us treat rare diseases that afflict only a few thousand people each year, and are thus usually ignored by mass-market-oriented medical technologies. It’s also no coincidence that these two mRNA vaccines were the fastest to market. They can be manufactured rapidly and, crucially, updated blazingly fast. Şahin, the BioNTech CEO, estimates that six weeks is enough time for the company to start producing new boosters for whenever a new COVID-19 variant emerges. Pfizer and Moderna are both already working on boosters that better target the new variants we’ve seen so far, and the FDA has said it can approve these tweaks quickly. 2. We Actually Learned How to Use Our Digital InfrastructureThe internet, widespread digital connectivity, our many apps—it's easy to forget how new most of this is. Zoom, the ubiquitous video service that became synonymous with pandemic work, and that so many of us are understandably a little sick of, is less than 10 years old. Same with the kind of broadband access that allowed billions to stream entertainment at home and keep in touch with family members and colleagues. Internet connectivity is far from perfect or equally distributed, but it has gotten faster and more expansive over the past decade; without it, the pandemic would have been much more miserable and costly. Technology also showed how we could make our society function better in normal times. Consider, for example, the advent of telehealth during the pandemic. Last summer, while a few hours away from home, I developed the same debilitating neck pain that I had experienced once before, about five years ago, on a different trip. It was instantly recognizable: sharp, relentless pain that radiated from where my neck joined my left shoulder; even a slight movement felt as if an army of tiny, poisonous spears were hitting that area. [Read: What a doctor learns from watching you on video chat] The previous time, I was told nothing could be done before I could see my doctor in person, many days later. Not so now: My doctor and I connected immediately through a new patient portal, which had a videochat option that had become available because of the pandemic. I described the problem and demonstrated my limited range of motion. He signed off by saying he’d send a prescription for oral corticosteroids to a nearby pharmacy. Just an hour later, and less than a full day after the onset of my symptoms, I was sitting in my car in the pharmacy’s parking lot, staring at the box of medicine in wonder. Previously, I had suffered through severe pain for multiple days, to the degree that I had started hallucinating from lack of sleep. This time, relief was right there in my hand. According to the CDC, telehealth visits increased by 50 percent in the first quarter of 2020, compared with the same period in 2019. Such visits are clearly not appropriate for every condition, but when warranted, they can make it much easier for people to access medical help without worrying about transportation, child care, or excessive time away from work. Remote access to medical help has long been a request from people with disabilities and people in rural areas, for whom traveling to clinics can be an extra burden. Work, too, has been transformed. Suddenly, hundreds of millions of people around the world had to figure out how to get things done without going into the office. It turns out that for many white-collar jobs, this is not just possible; it comes with a variety of upsides. Commutes, to take one example, are unhealthy—they waste time and potentially increase our sedentary time, which is associated with many adverse health outcomes, and perhaps worst of all, driving is among the most dangerous activities we undertake each day. The competition to try to avoid long commutes distorts property values and can worsen inequality, as those with money pay extra to live near centers of work, while other residents can no longer afford to live there. Unsurprisingly, many of my luckier friends—those able to work from home and who did not suffer directly from COVID-19—have been whispering about how much better their lives have gotten without commutes and with more flexibility. Many events have become a lot more inclusive too. Throughout the past year, I’ve been able to attend conferences and talks I’d otherwise have no chance to participate in without extensive time and travel costs. I’ve also given talks during which I’ve interacted with folks from around the world, who might never have been in that “room” otherwise. And I’ve noticed that a broader range of experts can appear on TV, now that we’ve normalized calling in from one’s home office, living room, or even bedroom. In a world divided by visas, income inequalities, time constraints, and opportunity, why didn’t we just incorporate videoconferencing into more of our events before? Why didn’t we take questions from the audience not in the room? We should keep doing that after the pandemic as well. I certainly miss some of the serendipitous conversations that conferences and other in-person events provided: not just during the talks, but in the corridors, or at breakfast before a panel. And it’s true, such events are a form of livelihood for many, and I’m not advocating for eliminating that income. It’s also not that we should never go back to the office, nor ignore all the issues that can stem from working outside of the office—especially the threat to work-life balance. Being in the same office also allows for conversations that go beyond strict work discussions, and the connections they foster. We might never be able to fully replicate those positives digitally, but we should still provide some remote access to those who would otherwise be completely left out. 3. We’ve Unleashed the True Spirit of Peer Review and Open ScienceOn January 10, 2020, an Australian virologist, Edward Holmes, published a modest tweet: “All, an initial genome sequence of the coronavirus associated with the Wuhan outbreak is now available at Virological.org here.” A microbiologist responded with “And so it begins!” and added a GIF of planes taking off. And so it did indeed begin: a remarkable year of open, rapid, collaborative, dynamic—and, yes, messy—scientific activity, which included ways of collaborating that would have been unthinkable even a few decades ago. Holmes was announcing that a scientist in China, Zhang Yongzhen, had rushed to sequence the genome of the mystery virus from Wuhan—his team had worked practically nonstop, completing the sequencing a mere 40 hours after a virus sample had arrived in a box of dry ice at his Shanghai office. Without waiting for approval or official permission, Zhang also promptly shared the result with a consortium of researchers in Australia, giving them the go-ahead to post it online in an open depository. [Read: The coronavirus is evolving before our eyes] Peer review—review by one’s fellow scientists—remains the cornerstone of the scientific process, and rightly so: Good science happens when members of a community dedicated to advancing our knowledge can examine findings, replicate results, test theories, and challenge one another. However, peer review as a formal process—as it happens right now—is different from the idea and spirit of peer view. We have “peer reviewed” scientific journals in which scientists can publish their findings. But in a hard-to-believe-but-true twist, many of those journals—especially the highly prestigious ones that can help a scientist’s career—are privately owned by for-profit companies, even though the peer reviews are done for free, on a volunteer basis, on articles that are submitted by scientists who also don’t get paid by the journals. Worse, after they go through the formal process at these for-profit journals, these papers are then put behind paywalls, meaning these companies then charge outrageous sums to academic libraries in universities—whose scientists have freely contributed the paper and the peer review. The companies block the general public from accessing them too, unless they also pay for them. These companies will even charge scientists for the privilege of making these papers “open access”—again, papers written by the very scientists who receive no financial benefit from charging the public! It’s little wonder that these companies remain highly profitable while many academics are up in arms over this terrible process that impedes the dissemination of science! Unfortunately, scientists—especially those who are early in their career—feel compelled to keep participating in this system, because getting published is the coin of the realm for hiring, promotions, and prestige. Well, no more. When the pandemic hit, it simply wasn’t tenable to keep playing the old, slow, closed game, and the scientific community let loose. Peer review—the real thing, not just the formal version locked up by for-profit companies—broke out of its constraints. A good deal of the research community started publishing its findings as “preprints”—basically, papers before they get approved by formal publications—placing them in nonprofit scientific depositories that had no paywalls. The preprints were then fiercely and openly debated—often on social media, which is not necessarily the ideal place for it, but that’s what we had. Sometimes, the release of data was even faster: Some of the most important initial data about the immune response to the worrisome U.K. variant came from a Twitter thread by a tired but generous researcher in Texas. It showed true scientific spirit: The researcher’s lab was eschewing the prestige of being first to publish results in a manuscript by allowing others to get to work as fast as possible. The papers often also went through the formal peer review as well, eventually getting published in a journal, but the pandemic has forced many of these companies to drop their paywalls—besides, the preprints on which the final papers are based remain available to everyone. Working together, too, has expanded in ways that were hard to imagine without the new digital tools that allow for rapid sharing and collaboration, and also the sense of urgency that broke through disciplinary silos. For example, in early 2020, after I started writing about the necessity of wearing a mask, it became clear that we also needed detailed scientific articles looking at the science of the efficacy of masks for dampening community transmission. The questions the topic touched on involved many disciplines, including infectious diseases, aerosol science, and sociology. So I teamed up with a group of scientists, doctors, researchers, and data analysts across the globe to co-write an academic paper, and from start to finish, it was like nothing I had done before. A lot of scientific work involves international teams, but this time we had assembled practically on the fly: the co-authors lived in cities as varied as Cape Town, South Africa; Beijing, China; Chapel Hill, North Carolina (me!); Stanford, California; and Oxford, England. We would eventually publish in the most highly cited scientific outlet in the world, the Proceedings of the National Academy of Sciences of the United States of America, which is more than 100 years old. Most of the tools we used, however—shared editing of scientific papers, videochat and other forms of meetings—weren’t widely available or as easy to use even just a few years ago. Like many others, we didn’t wait for formal peer review to end before sharing our findings. We quickly put our paper onto a preprint server so that it could receive both open peer review from the scientific community and questions and comments from other relevant stakeholders, including policy makers and even ordinary people trying to puzzle through a confusing time. And feedback came in quickly: We received thoughtful and lengthy emails and Twitter corrections and comments, which were extremely useful—as well as much less useful contributions, which sometimes involved random people getting mad at us. I started categorizing the feedback on the sections I’d worked on, as did many of my collaborators. Even before the first round of formal peer reviews were in, we used that feedback to generate a new, stronger version, which we added to the preprint server. We then got our initial round of formal peer review—which we also found quite useful. We updated the paper again, resubmitted the new version to PNAS, and waited for a second round of peer review (which took many months, but was also very useful). Finally, about a year later: acceptance and formal publication. [Read: Why aren’t we wearing better masks?] I have to admit, the final published paper looks great on my CV, but our preprint had already been downloaded more than any other paper on that server. It has been cited hundreds of times, including in the highest-ranked medical and scientific journals in the world; contributed to the global scientific discourse; and played a crucial role in the adoption of mask mandates. We even had a celebratory happy hour—chatting about our lives; challenges; and new, shared friendship. This process of open peer review is fast, dynamic, and, admittedly, messy; it’s not without its downsides. Too many sensationalist headlines have resulted from journalists rushing to write about not yet sufficiently evaluated preprints, without waiting for the process of open review and feedback to do its work. This can be confusing to the broader public. However, the explosion of preprints is sometimes portrayed as the downfall of formal peer review. It’s the opposite. No process that allows more insight into how the sausage gets made can avoid a glimpse of its less tasteful elements, but what we need to change is how we relate to science, not try to go back to the stilted, slow pre-pandemic world. We should embrace the extraordinary and robust process of open science and more peer review, as well as its dynamism, even as we establish new guardrails to contain its energy. The pandemic happened at a moment of convergence for medical and digital technology and social dynamics, which revealed enormous positive potential for people. Nothing will erase the losses we experienced. But this awful year has nudged us toward dramatic improvements in human life, thanks to new biotechnologies, greater experience with the positive aspects of digital connectivity, and a more dynamic scientific process. Still, let’s never do it again. from https://ift.tt/3tyBurV Check out http://natthash.tumblr.com It was unimaginable. A respiratory virus turned global pandemic disrupted every facet of our world. This was something public-health officials had been planning for. Yet most leaders seemed totally unprepared for its onslaught. A year later, half a million Americans have died. Where do we go from here? The Atlantic will explore the year that was, the power of the vaccines to stop the spread of the coronavirus, and the potential return to normalcy. The event will feature deputy editor Ross Andersen and staff writers Derek Thompson, Katherine J. Wu, and Sarah Zhang. from https://ift.tt/3bTpXgY Check out http://natthash.tumblr.com I’ve spent the pandemic taking daily walks around my neighborhood, along what are now overly familiar blocks. I try to vary my route, but I can tell you which patches of sidewalk are most treacherous, which houses have the most stylish doors, and where the yippiest dogs reside. Last week, a text interrupted this routine, with a link to schedule my first vaccination appointment. For a second, I thought it was spam. But I stopped, and clicked, and very shortly had snagged an appointment, for just a few days later. The prospect of vaccination shocked my COVID-19 life out of its constrained yet predictable rhythm. I work from home; I wear pants without buttons; I spend Friday nights watching a movie or doing laundry and Saturday nights Zooming with friends. This little world is equal parts dull and intense; everyone I know is sad, exhausted, antsy, and resigned. I can’t wait to leave these confines behind, and yet this world is mine. The people who populate it care about me—they are happy to hear from me, even when I have nothing to say except how hard everything is. The dangers are monumental, but I mostly choose when I confront them. It’s both suffocating and a sanctuary. In the same way that not everything about “normal” life should return, not everyone is ready to rush headlong into a world reopened. Making sense of this nebulous non-time will take a while (though efforts are already under way). The continuing losses—of life and livelihood, of routines and community, of trust in the future—are so immense and terrifying that they sometimes seem incomprehensible. Yet the emotional healing required for post-COVID-19 life are things a vaccine alone can’t provide. And despite the tragedy and horror, not every aspect of the pandemic has been terrible. With distance and reflection, those of us who were able to hunker down during the pandemic may even come to cherish the shelter of COVID-19 life. In the mid-1980s, a futurist named Faith Popcorn became famous for inventing the idea of “cocooning.” “We are trying to control everything,” she told the New York Times reporter William Geist in 1986, “to protect ourselves from a harsh and unpredictable world.” The signs of cocooning were everywhere, in wholesome television series such as The Cosby Show and the renewed popularity of frozen dinners such as Lean Cuisines, in the explosion of VCR sales and the uptick in gun ownership. Emerging from the drug-addled, sexually revolutionized 1970s and early ’80s, cocooning captured a cultural retrenchment and a desire for everything to feel homier and safer. Cocooning caught on, so much so that Merriam-Webster added the term to its dictionary in 1986. Understood as an emergent trend, cocooning rendered disparate cultural shifts into part of the same story—linking couch potatoes to Jane Fonda workout videos to the surge in ’50s nostalgia. Corporations as varied as Domino’s Pizza and Kmart used cocooning to rethink their strategies. As Popcorn wrote in her best-selling 1991 book, The Popcorn Report, “Cocooning is about insulation and avoidance, peace and protection, coziness and control—a sort of hyper-nesting.” [Read: Why Americans have turned to nesting] Popcorn had been talking up cocooning for years before it hit the zeitgeist. And once it did, she kept on talking: Cocooning would reign in the aughts, she predicted; cocooning was a trend to watch in 2006, according to her consultancy, BrainReserve; the financial cutbacks of the Great Recession would instigate a trend of “uber-cocooning.” No surprise, then, that BrainReserve calls the pandemic’s closed-off, sanitary existence “deep cocooning.” Such constancy warrants skepticism, but in this case, cocooning does accurately describe what the pandemic has wrought. With the outside world disrupted and inaccessible, many people have been all but forced to retreat into a protective shell. As Popcorn anticipated in the ’80s, people fear the outside world and are careful about who and what they allow past their barricades. Stimulation happens inside; screens provide a controllable window onto the world. For some, the cocoon has a softness to it, with anxious hours occupied with home improvement, baking, and crafting. And just like the cocoons of yore, COVID cocoons are rife with nostalgia, especially as inhabitants binge on old episodes of The Sopranos or listen to decades-old music. Mel Ripp, a writer in Madison, Wisconsin, told me about going through her favorite albums from her youth because “nostalgia and my memories of being a kid seem like the one thing I can control.” The familiar is armor against a scary, unknown world. Rather than think of Popcorn like a broken clock that’s right twice a day, it’s more charitable to say she identified a deep cultural impulse that has transformed the relationship between the individual and the public. The ’80s cocoons never fully opened. The pandemic accelerated a metamorphosis of the home that’s been decades in the making. Even as states reopen their economies, practices such as working from home, video first dates, DIY dye jobs, and nonstop online shopping will not completely vanish. They’ll stay because they are more convenient and cheaper than their in-person alternatives. And they’ll stay because they’re good enough and the pandemic has changed us. We’ve become both stronger and weaker, more accepting and less tolerant, more resilient but also more wary. West Chester University hosts a digital archive that includes interviews of survivors of the 1918 influenza pandemic. The interviews were done in the 1980s with people who were children during the outbreak. Listening to them recently, what I found most striking is that their tone isn’t exactly sadness. Two women reminisce about how their neighborhood had so many unburied bodies that the smell “would knock you right down through the alley.” Another woman recalls the neighborliness of her father, who once carried the corpse of a teenage boy to the cemetery, so folks could gather and pray. The stories are horrible. But the survivors’ voices? Candid. Tough. Purposeful. These are decades-old memories, cathartic not despite their difficulty, but because of it. Tahneer Oksman, an associate English professor at Marymount Manhattan College who studies memory and grief, explains that “thinking you can come out of something horrific—there’s a kind of euphoria that comes from that.” As one of the thousands of “COVIDivorcées,” I can relate. When I tell people that my 13-year marriage ended during the pandemic, the most common reaction is pity. But having one’s life turned upside down isn’t nearly so bad when the entire world is suspended. As twisted as it sounds, the pandemic has protected me—from judgment, from feeling like I should put myself “out there” again, and from having to dine or go to the movies alone. [Read: There’s no real reason to eat three meals a day] I’ve heard similar things from some new moms who had extra weeks and months with their newborns, and who feel both good and bad anxiety when contemplating bringing that child fully into the world. My friends with toddlers desperately need alone time and sleep, but have also told me how much they appreciate never having to dress up for anyone or be anywhere. Rory James, a comedian in Los Angeles, explained to me, “I don’t miss being in crowds. And in the future, I would pay more to eat at a restaurant that only operates at 25 percent capacity.” I’m a college professor, and during a recent remote class, several students voiced reluctance about attending courses in person next fall, because they fear their irresponsible classmates and have acclimated to taking classes from their bedroom. Human beings are an adaptable species, and Americans are both pugnaciously optimistic and hyperbolic. The combination of these characteristics is a paradox: People find a silver lining around even the stormiest clouds while also believing firmly that the sky is falling. Apart from appreciating COVID cocoons, many people have determined that the “old normal” may not be worth it. That might involve seeing the benefits of working less, traveling less, and buying less. Or it might mean feeling incapable or unwilling to move at the pace that pre-pandemic life required. Fond memories of the pandemic, whenever they come, may be driven less by an affection for today’s hardships and more by fear and stress over tomorrow’s demands. “I’m not functioning with the mental quickness I’m used to,” wrote Jessica Grose recently in The New York Times, referring to the burnout of trying to work and parent during the pandemic. Others worry that their mental acuity might not ever return. Of course, those who cocoon depend on people who don’t cocoon—those who are now called “essential workers,” and include the precariously employed, the food-insecure, and the working poor. Futuristic predictions that equate cocooning with refuge tend to ignore that being able to work from home and have groceries delivered is a privilege that is reinforced by the cocoons themselves. The pandemic has in many ways frayed the social contract, heightened divisions, and compounded inequities. At the same time, this era has underscored how interconnected every human life is to every other, and how the deep, structural inequities that plague American society have incalculable costs for everyone, even the most privileged. It is from this turbulent point that dramatic, systemic change—around issues such as police brutality, racism, poverty, climate change, disability rights, and so much more—might spring. Someday, this time might be considered as transformational as the late 1960s. If right now is indeed a revolution, that means, quite simply, we can’t just go back to the way things were. Just like there was no road map during the pandemic for working parents with school-age children, or single people navigating social distancing, or seniors in nursing homes, there is no instruction manual for how to live in a reopened world. That world is both familiar and foreign. Opening quickly will have opportunities and costs that aren’t yet apparent. Once the new new normal begins, aspects of the old new normal might not look so bad. from https://ift.tt/30TJhEl Check out http://natthash.tumblr.com For much of 2020, the world pinned its collective post-pandemic plans to a single, glimmering end point: the arrival of an effective COVID-19 vaccine. The resounding refrain of “when I’m vaccinated” has long conjured images of people shedding their masks, hugging their friends, and returning to a semblance of normalcy. And now some vaccinated people are doing exactly that. In recent weeks, I’ve heard dozens of stories from friends, family members, and co-workers about vaccinees who are immediately dropping their guards after their shots, in some cases discarding their masks and congregating with others. Deepta Bhattacharya, an immunologist at the University of Arizona, told me that one of his colleagues—another biologist—went out to a celebratory dinner right after getting a dose at a 24-hour clinic. But immunity to the coronavirus doesn’t just magically manifest the day someone gets a shot. The CDC does not grant membership to the “fully vaccinated” club until at least two weeks after the final dose in a vaccine regimen—a time that roughly corresponds to when most people are thought to acquire enough immunity to defend against a symptomatic case of COVID-19. Only then, the agency announced last week, can vaccinees start to carefully change their behavior, mingling maskless in small groups indoors, visiting the unvaccinated on a limited basis, and skipping postexposure quarantines. The jab itself “is momentous,” said Bhattacharya, who shared photos of his own injections on Twitter in hopes of swaying hesitant peers. But each injection is merely a precursor of what’s to come. “Ultimately, the real momentous ‘occasion’ is what happens gradually after the [final] shot,” he said. This is true of all vaccines: Their protective effects take several days or weeks to kick in. It’s the reason we get our flu shots in the fall, well before the height of respiratory-virus season, and it’s why health officials often recommend that vaccines required for travel, such as those that ward off yellow fever, be administered about a month or more in advance. Vaccination, and the defenses it affords, is less a singular event than a series of steps on a shifting landscape. [Read: The next phase of vaccination will be even harder.] From the standpoint of protection, not a whole lot happens on day one of a vaccination regimen—which makes concern about infections detected around the time of vaccination unwarranted. In late December and January, social-media platforms were swarmed by a flurry of nervous headlines and sound bites documenting positive test results in recently injected health-care workers and politicians. But cases like these are entirely expected. The shot simply delivers a package of study materials to the body; immune cells must then internalize the information about the infectious invader, a complex process that unfolds over days or weeks. Shortly after the vaccine is administered, these cells embark on a crash course in the coronavirus. Fast-acting immune cells inspect the shot’s contents, then ferry the intel back to their specialized colleagues: B cells, the immune cells that make antibodies, and T cells, which can annihilate virus-infected cells, learn to zero in on the pathogen with laser-sharp precision. The body also works hard to ensure that only the best B cell and T cell fighters are recruited to the cause. Some of these cells will even compete with one another, eliminating the weaker or less discerning fighters. “They need to be able to recognize when they should respond, and when they should leave well enough alone,” Bhattacharya said. “That takes some time.” In this light, a SARS-CoV-2 infection that occurs before the body has had time to respond to a vaccine is about as surprising as students failing an end-term exam because they haven’t finished the reading assignments. (Some asymptomatic infections are also expected with the currently cleared vaccines, which are expected to be better at protecting against symptomatic disease.) Vaccine-induced protection also endures and evolves as the pathogen-memorizing pupils of the immune system crunch through their lessons. There’s nothing particularly special about day 14; antibody levels ramp up gradually after a shot or series of shots is delivered, Padmini Pillai, an immunologist at MIT, told me. But data collected during the vaccine makers’ clinical trials indicate that after two weeks, the body reaches a “threshold of protection,” Pillai said. (It’s worth mentioning here that the Pfizer-BioNTech and Moderna vaccines require boosters three or four weeks after the initial injection; the Johnson & Johnson jab, which contains very different ingredients, seems to be memorable enough as a single shot.) [Read: The second COVID-19 shot is a rude awakening for immune cells.] Although plenty of people have documented their shots on camera, vaccinees aren’t taking many selfies at the two-week mark: The end of a waiting period is a pretty dull milestone, especially compared with the photogenic pizzaz of the injection itself, which comes complete with a needle-tipped syringe filled with lifesaving liquid. The day on which people are cleared to alter their behavior is, by contrast, devoid of “salient, concrete cues,” says Gretchen Chapman, a psychologist at Carnegie Mellon University who studies human behavior and vaccines. “Two weeks later, nothing happens; there’s no event,” she told me. “It’s not like your arm turns purple to tell you, It’s time.” Considering the nation’s sputtering rollout and the many logistical problems that have stymied delivery, getting any shot at all is worthy of celebration. But there’s a gentle deception tucked into fixating on the moment a vaccine enters an arm: It runs the risk of conflating the time of injection with the time of protection. Clearer messaging about the vaccine timeline might help, says Alison Buttenheim, a behavioral scientist at the University of Pennsylvania who studies vaccines. Receiving the second shot in a two-dose vaccine regimen, for example, counts as series completion, Buttenheim told me. That’s not the same thing as what the CDC, in its new guidelines, means by “fully vaccinated.” And yet, many news outlets and public-health authorities, including the CDC’s own vaccination tracker, are putting people in the “fully vaccinated” count as soon as they receive their second shot of the Moderna or Pfizer vaccine, or their one-and-done dose of Johnson & Johnson. (The agency acknowledges in a footnote at the bottom of its tracker that it is using fully vaccinated in two different ways.) To distinguish injection from protection, vaccination cards could include the dates of not just the shots themselves, but the end of the recommended waiting period. Both Chapman and Buttenheim pointed out that some health departments and vaccine makers once distributed refrigerator magnets to the young recipients of HPV shots, which are delivered in multidose regimens over several months. To keep parents and their kids from forgetting their next appointment, the magnets lit up when it was time to return for a booster. If something similar were handed out at COVID-19 vaccination sites to denote when people reach the protection threshold, “wouldn’t that be nifty?” Chapman said. Perhaps people should take a second or third vaccine selfie, commemorating their immune status after their cells are better prepared to fight off the virus. These photos wouldn’t be as flashy. But they might help paint a more realistic portrait of what vaccination actually is—not a discrete moment, but a gradual unfurling on scales large and small. Immunity builds iteratively, not instantaneously, in people; it accumulates slowly, over time, in populations. The vaccines are here. After a difficult year of waiting, we all just have to wait a little longer. from https://ift.tt/3lqeNTX Check out http://natthash.tumblr.com |
Authorhttp://natthash.tumblr.com Archives
April 2023
Categories |
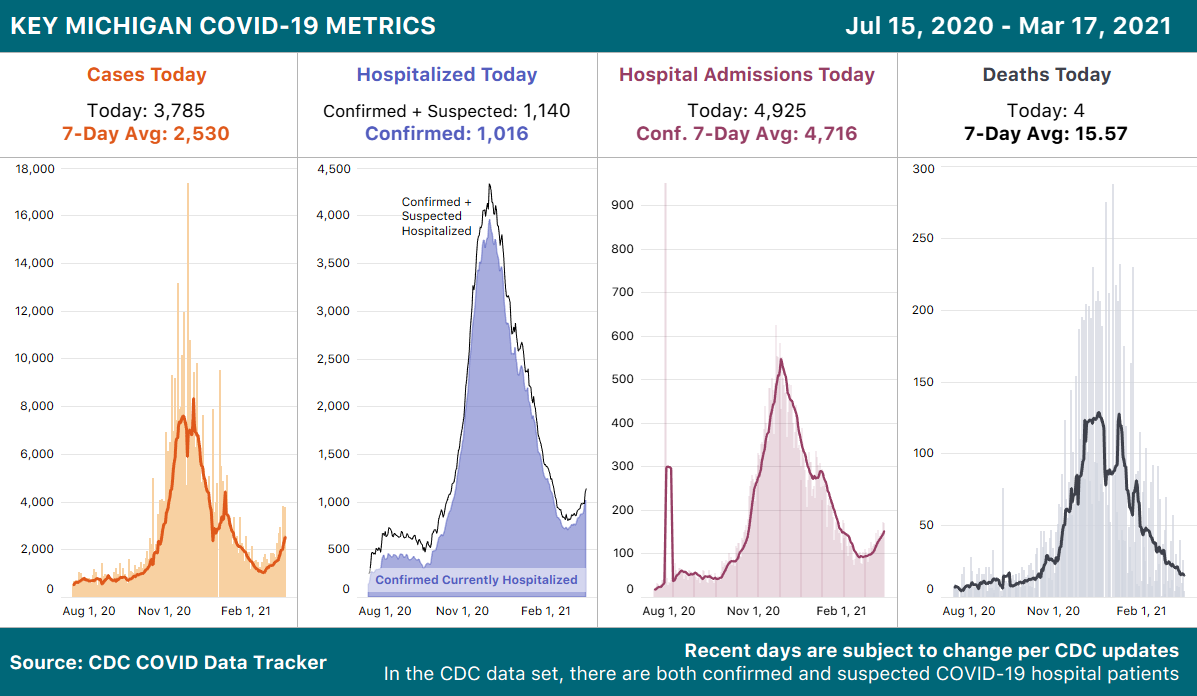
 RSS Feed
RSS Feed
