|
The Trump administration mandated that hospitals no longer send their data to the CDC, and the public appears to have lost access to key data. Alexis Madrigal, staff writer and co-founder of The Atlantic’s COVID Tracking Project, joins James Hamblin and Katherine Wells on Social Distance to explain what happened and why it matters. Listen here: Subscribe to Social Distance on Apple Podcasts, Spotify, or another podcast platform to receive new episodes as soon as they’re published. What follows is an edited and condensed transcript of their conversation. Katherine Wells: We had a question from a listener that I wanted to share: WTF is going on with the CDC? Alexis Madrigal: Yeah, there has been a pretty active effort from the White House to control the information that’s going out from the federal government about the pandemic. Wells: I mean, you founded the COVID Tracking Project in response to that. Madrigal: Yeah, basically because of this problem. And now there is a new phase of this. Hospitalization data had been fed through the CDC-run system for quite some time, literally decades. And I’m sure that that system was creaky. And I’m sure that it was not purpose built for this moment. I’m sure there were issues with that data system. But it was a functional system that people knew about and knew how to use at these various hospitals all across the country. Health and Human Services, which is the umbrella organization that houses the CDC, created a new system routing around the CDC. And it may be fine. It’s just that the CDC and particularly the data that the CDC was collecting in this case was public and was out there. And you could see it and you could use this hospital and ICU capacity data. In fact, some partners of ours in the COVID Tracking Project called COVID Exit Strategy, were in fact using that exact data. And when this new HHS directive came down, that data blinked offline. That’s something that we’ve been extremely worried about at the federal level. James Hamblin: Hospitalization capacity is the most important single thing to driving public policy about opening and closing. If you had to choose just one metric, that is the point where, at least in the U.S., places have finally decided to shut down when their I.C.U.s are almost full. Madrigal: Yeah, that’s my understanding of a lot of governors’ decision-making. Hamblin: Whether or not it should be that way. All the data is important. But if there were one that the public needed to know: hey, if we don’t shut things down, you might get turned away from a hospital because our hospitals are full. That’s really important for the public to have. Madrigal: Yeah, that’s a great point, Jim. I also think people interpret these moves about where the data flows and the pipelines, in terms of taking data away from the CDC. My interpretation of what’s happening is: it’s actually about controlling the release of that information, which is different. It has less to do with hamstringing the fight against the disease and more to do with controlling the public narrative about what’s happening. That’s why these numbers are crucial to have in one place. For example, COVID Exit Strategy—which is a partnership between the former deputy CTO of the U.S. and public-health researchers—they were using it as one of their indicators of a state that’s having problems. Like you’re saying, of the indicators, [hospitalizations] is the one that indicates the problem has become very acute. To take that information out of the public realm or even just make it more difficult to access in the way that a lot of other data about this pandemic works: it’s out there ... if you’re willing to organize 300 people to collect it every day. from https://ift.tt/3jnjBIe Check out http://natthash.tumblr.com
0 Comments
There’s a fire up north, the woman says, the Kincade Fire. It flickered into existence on the nighttime horizon, a shapeless brightness billowing into the sky. Now the wind’s whipping it south toward Santa Rosa. Evacuations are under way, and she worries her home will burn. Allison Chapman listens in silence. She’s modeling for a makeup demo when the woman walks into the studio, where Allison studied after moving south a couple of years ago, at 18. She knows this woman from back home in Northern California, knows how close this woman lives to her grandparents, knows that if the fire is threatening this woman’s home, it’s threatening theirs, too. She feels the panic coming on. It begins, usually, with a quickening of the heart and a tightening of the chest. Then comes a rush of cold, which is ironic, in a way, because her fear is fire. Her mind jumps backwards first—to the flames tearing across the mountainside on a late-summer evening in 2015, to the dark smoke rising from the woods around her house, to the toy wagon wheels discovered weeks later amid the wreckage—then springs forward and explodes like a shotgun shell into a million imagined tragedies. She shivers. Only this time she doesn’t. In the four years since the Valley Fire destroyed her home, Allison has learned to suppress that feeling before it overwhelms her. She tells herself that she is okay, that her grandparents are okay, that everything is okay. Allison had occasional panic attacks even before the Valley Fire. Afterward, though, the attacks seized her daily and lasted as long as a couple of hours. Often something would trigger them—a word, a smell, a sound—but other times they came without cause. Her panic would catch her like a riptide, sudden and irresistible. When it did, her mother, Ellie, would find her curled up on the floor of her room, hyperventilating, and hold her until her breathing slowed. The next day, it would happen again. Or if not the next day, then the day after. She felt she’d lost control. She started to cut herself. She wore long sleeves to hide the scars. When the woman leaves, Allison calls her mother. (The Atlantic agreed to use pseudonyms for all family members to protect their privacy.) Allison’s grandmother is lying in a hospital bed with her lungs full of smoke, Ellie says, but she’ll recover. Her house is safe for now, though you can never be sure with fire; you’re always at the mercy of the wind. And, what’s more, this will happen again. California has long had a propensity to burn. Its record of fire begins underwater, at the bottom of forest-fringed lakes, where ancient blazes left their stories in charcoal deposits. Tens of thousands of years later, the record continues in the logbooks of the Spanish, who saw “many smokes” rising above the coastal treetops when they sailed into San Pedro Bay on a Sunday morning in October 1542. Baya de los Fumos, they christened the waters. “The Bay of Smoke.” Even by California’s standards, though, recent years have been extraordinary. Nine of the 10 most destructive fires in the state’s recorded history have occurred in the 21st century—six of them in the past four years alone. In October 2017, the Tubbs Fire destroyed more than 5,600 buildings in Napa and Sonoma Counties, making it the state’s most destructive fire on record. About a year later, the Camp Fire supplanted it, razing the town of Paradise and killing 86 people. Just last fall, the Kincade Fire torched nearly 80,000 acres. [Photos: Embers fly in California’s wind-driven wildfires] Wildfires tend to leave a common signature—the black earth and white ash, the jagged trees and bleak chimneys. Americans have come to know these well. But the physical ruin is only a part of the aftermath. According to Patricia Watson, a psychologist at the National Center for Post-Traumatic Stress Disorder, 10 to 30 percent of wildfire survivors develop diagnosable mental-health conditions, including PTSD and depression. Another 50 percent may suffer from serious subclinical effects that fade with time. Studies have found that substance abuse and domestic violence rise after natural disasters. And while most fire survivors make a full recovery, many require formal treatment. In more than 50 interviews over the past two years, I’ve heard from survivors, researchers, clinicians, and government officials about the ways in which this long-lasting psychological damage can transform lives. Many survivors described feeling fragile and less capable of managing stress for years after a fire. Some recalled looking for incinerated possessions and breaking down when they realized they would never find them. One man recounted taking his granddaughter to see the 2018 Mary Poppins movie—about a family on the brink of eviction—and crying through much of its two-hour running time. That was more than three years after he lost his home. When a whole neighborhood or town feels these effects at the same time, the result is what one psychologist and fire survivor calls “community-wide trauma.” “It’s hard not to have a little PTSD,” says Jessyca Lytle, whose home burned down in the Valley Fire. “A lot of people just see it as ‘Well, it’s the new normal. I’ve just got to learn how to deal with it.’” The trauma is sustained and amplified by a distinctive characteristic of California’s wildfires: They recur, often in quick succession. A number of the survivors I spoke with described feeling “haunted” and “disturbed” by subsequent fires. As irrational as they knew it was, they felt as though the fires were stalking them. Now there is the coronavirus pandemic, a new disaster layered atop an already many-layered mental-health crisis. And while the virus will subside with time, the fires will not. According to the most reliable predictions, they will only worsen in the coming years. A 2016 study published in the Proceedings of the National Academy of Sciences concluded that as long as there remains fuel to burn, “anthropogenic climate change will continue to chronically enhance the potential for western U.S. forest fire activity.” All the while, Watson says, it will grow harder for survivors in vulnerable areas to maintain a sense of hope. And much of California is a vulnerable area. 
Allison Chapman had always been an artistic child, but not until after the Valley Fire did she turn her talents toward special-effects makeup. Before, she’d painted fantasy worlds and nature scenes—“sweet stuff,” her mother said. After the fire, she fixated on simulating blood and gore. She would paint bullet wounds on her neck, lacerations on her arms, the sickle-shaped scars of a Glasgow smile on her face. Once, she did herself up like the disemboweled Black Dahlia. Ellie began to notice Allison shaking and sweating even when she wasn’t having panic attacks. And she’d grown so pale. At first, Ellie suspected the flu, but the symptoms did not abate. Only later did she see her daughter slipping into the bathroom after meals. At the same time, Allison’s makeup art was starting to look more realistic. Ellie could swear that some of the wounds seemed to be reappearing in the same places. One day, she saw Allison cleaning makeup off her arms in the sink. As the water streamed over her skin, most of the red streaks washed away—but not all of them. The effect, Ellie said, was “mind-bending.” It can’t have helped that she was struggling with her own mental-health problems—the whole family was. Her husband, Liam, had suffered from depression for years, but after the fire, Ellie said, it was “a whole new level, almost a different creature.” Mia, who was 8 at the time of the fire, had been the fearless child; ever since, she has been nervous and jittery. Now, when Ellie makes Mia’s bed, she often finds objects hoarded beneath the mattress, everything from candy to pocketknives. In the months after the fire, 6-year-old Zoe seemed afraid that if she left the house, she might never come back. The fear was not entirely unfounded: The Chapmans spent nights in more than half a dozen homes and shelters that year. For a while, they rented a place near a mountaintop helipad in Cobb, the remote, working-class community where they used to live. When Zoe heard the drone of a helicopter overhead, she would drop to the floor and spiral into hysterics, her mother recalled, like “someone who had been in a war zone.” Ellie herself knows something of trauma: She has long suffered from PTSD and anxiety caused by physical and sexual abuse in her childhood, she told me; since the fire, her symptoms have worsened exponentially. She quit her job at a winery because being there brought her back to the day the fire started. She quit her job at a plant nursery because being around other people was too much for her. There are just so many triggers, she said. She feels “like a semiautomatic weapon.” [Read: This is not a normal mental-health disaster] In the year after the fire, many days were hard, but one stands out. Allison and Ellie don’t remember the exact date. Allison’s sisters were playing in the yard when she walked into the family’s galley-style kitchen and drew a knife from the knife drawer. Leaning against the sink, staring at the white cabinets and yellow walls, she pointed the blade at the floor and contemplated what she was about to do. She’d considered suicide before, but never this seriously. She’d never felt the weight of the knife in her hands. “I was basically ready to end it all and be done with it right there,” she told me. Then Ellie walked into the kitchen and saw her daughter slumped against the counter. Ellie took the knife, and they both began to cry. Allison’s teenage years had always been difficult. She’d struggled with bullies, with friends, with anxiety. But she’d managed. After the fire, Ellie said, “her coping mechanism was gone.” Psychologists sometimes say that trauma gets burned into the mind, like the imprint of a branding iron, and in a way it does. In truth, though, trauma is not so much a scorch mark as a flame, flaring up and dying down, inconstant. It burns in the mind. And just as some materials burn more readily than others, so too do some minds. Part of this is genetic. Another part is cognitive. But a growing body of research has also linked vulnerability with prior exposure. “When traumas accumulate over time,” says the Alaska Network on Domestic Violence and Sexual Assault, “they may be associated with more severe and complex psychological reactions.” For an alcoholic or a battered partner or a victim of sexual abuse, this means a heightened risk of serious mental-health problems. And if another disaster strikes—say, a pandemic—the risk rises higher still. [Read: I was depressed before all of this. Now what?] After a wildfire, the particular nature of the resulting trauma depends on the particular experience of the affected survivor. For some, trauma derives from the panic of a narrow escape. Studies have repeatedly linked fear for one’s life with PTSD, which is part of the reason firefighting takes such a heavy psychological toll. A 2016 International Association of Fire Fighters report found that firefighters experience PTSD at rates comparable to those of combat veterans. They are also about 40 percent more likely to take their own life than the general population. In 2017 alone, 103 firefighters died by suicide—10 more than did in the line of duty. Even for fire survivors who have been spared the imminent danger and acute fear, the weight of the loss—of homes, of communities, of memories—can be enough to induce trauma. It was for the Chapman family. The Rivas family was not spared the imminent danger and acute fear. On a windy night in October 2017, Erika Rivas’s 13-year-old son roused her from a fitful sleep about half an hour before their home burst into flames. He was whispering something about a fire. His cousins, who lived just a few houses down, were already evacuating, he said. Coffey Park, where the Rivases live, is a quiet Santa Rosa suburb whose tree-lined lanes and cul-de-sacs do not attract much traffic. But when Erika and her son looked out their front window, they saw utter gridlock. The time was 1:30 a.m. “Something’s wrong,” she told her husband. Moments later, through a back window, he saw “a meteorite-size ball of fire” crash down in the backyard. “We need to get out now!” he yelled. “Everybody, get out now!” They had no time to grab anything—not clothes, not money, not photographs. Erika didn’t even have time to put shoes on. As she rushed to the car, she heard solar panels shattering overhead, like a thousand china plates dropping all at once. Giant tumbleweeds bounded across the smoky street. By the time Erika pulled out of the driveway, the garage was on fire. In the end, the Tubbs Fire consumed 36,000 acres, 2,800 homes, and 22 human beings. One of the 2,800 homes was Erika’s. One of the 22 human beings was her neighbor. A firefighter who’d been in the area that night saw Erika’s house burn down just 15 minutes after she fled with her family. When she was allowed to return, she sifted a few relics from the rubble—her grandfather’s wedding ring; a safe full of papers torched by the sheer heat of the blaze; her grandmother’s coffee cup, which looked all right but fell apart when she tried to pick it up. Looked all right but fell apart—that was how Erika felt after the fire. “You think one day you’re fine, and then something happens,” she told me. “You see something that you remember, and you just cry.” Or you recall something that you’ve lost—she kept reaching for her spatula, she said—and you also cry. Or you cry for no reason at all. But even then—perhaps especially then—the ambient stress of the recovery process hangs in the air, and that is reason enough. After a wildfire, obstacles abound: the scramble for shelter, the competition for builders, the toil of the insurance process. Studies have shown that these ongoing personal, logistical, and financial difficulties often lead to depression. “Somebody goes through a trauma—if they’re going to then face a whole lot of continuing obstacles, then that maintains the stress,” says Joe Ruzek, a PTSD researcher at Stanford and Palo Alto Universities. “It becomes more difficult to put the trauma behind.” These long-term challenges can even elicit PTSD symptoms in survivors who do not initially manifest them. A year after Hurricane Katrina, researchers found that more than 40 percent of survivors with PTSD had not developed symptoms until after the six-month anniversary. “People have that experience of revictimization because there’s an adrenaline after the fire of, like, Okay, we’re going to get through this,” Ronit Rubinoff, the executive director of Legal Aid of Sonoma County, told me. “Then that adrenaline fades and people realize … Jesus, I am no closer to even just putting a stick in the ground.” Two years and two builders after the Tubbs Fire, the Rivases have only just moved into their new home. The process added one more stressor to what Erika says was already the worst time of her life. For years, she told me, she has regularly seen a therapist for PTSD and depression resulting from childhood trauma. But within a few weeks of the evacuation, her symptoms had grown much worse. Today, the smell of smoke can still trigger panic attacks. She cannot light a candle. And her memory has suffered. Usually it’s little things: where she left her keys or phone, for instance. But sometimes, she’ll forget long stretches of time. Once, she couldn’t remember who had taken her children to school in the months after the fire. With time, the lapses have grown only more frequent. Her therapist always says, “Maybe it will come to you,” but it never does. On a windy night this past October, while still living in a rental house, Erika sat by the TV with her family, watching the news about the Kincade Fire and thinking to herself, This is just like last time. Only this time the drama was unfolding in slow motion. She’d helped her children gather their things in case of an emergency evacuation, but she couldn’t bring herself to pack her own bags, because what are material possessions worth in a state that combusts on an annual schedule? When the evacuation order arrived a few days later, the Rivas family drove to the same restaurant where they’d eaten after the Tubbs Fire: Habit Burger. And just like that, cataclysm became custom. When it snows, we stay home and drink hot cocoa. When it burns, we evacuate and eat at Habit Burger. “I feel like this is normal right now,” Erika told me after the Kincade Fire, once she and her family had returned to their temporary home. “I don’t want this to become a normal thing in my life.” For many Californians, it already has. On Cobb Mountain, people call firefighting planes the state bird. Across the state, schools have smoke days instead of snow days. At Legal Aid of Sonoma County, which has represented many survivors of the 2017 Wine Country Fires, prospective clients were, for a time, asked to fill out a mental-health intake survey. A score of 15 or higher indicated that the client needed mental-health support. Of the 50 assessments the office reviewed in the year and a half after the fires, just one scored below a 15. 
For a moment, not long after the Valley Fire, Ellie Chapman felt a kind of freedom. No more chores, no more dishes, no more laundry: She had no household responsibilities, because she had no household to be responsible for. The shock, she says, was “absolute.” This is how it goes for many fire survivors. The panic of disaster resolves into the numbness of shock; the numbness of shock, into the pain of trauma. Cobb Mountain had not yet reopened when a family friend called to tell the Chapmans that their house was gone. They were living out of their Ford Explorer at the time—a big car but a small home—so that is where they cried. Two weeks later, when the National Guard escorted Ellie back to the property in a Humvee, to look for the pets she’d left behind, she hardly recognized what she saw. The meadow out front where the yellow-flowered mullein used to grow was stone-smooth and black, and all that remained of their home was a scorched chimney. The animals were gone. Amid the wreckage, she spotted the metal handles of her great-grandfather’s handmade rolltop desk, which she had treasured above all other possessions. Don’t take anything that doesn’t have a heartbeat, the officers told her. She left the handles in the dust. At around that time—before Allison was bingeing and purging, before she was cutting herself, before she drew the knife from the knife drawer—Ellie began in earnest to seek mental-health treatment for her family. In a nearby town, FEMA and the California Governor’s Office of Emergency Services had set up a disaster-recovery center. Ellie went from one folding table to the next, asking representatives from federal, state, and local organizations where she could find help. Over the next three years, she says, she tried more than half a dozen organizations and government agencies. At the plant nursery where she worked, she asked almost every customer for advice about where to go. Some people referred Ellie to crisis hotlines, but Liam and the girls wouldn’t talk to a stranger on the phone. What little in-person care she found came mostly in the form of group sessions, and she wasn’t going to talk about her marital problems—she had caught Liam cheating—or her daughter’s self-harming in that kind of setting. “This is a small community,” she told me. “We all kind of know each other … I didn’t want to do that.” And yet she didn’t know what to do. On the morning of May 16, 2018, she texted a friend: I tried to contact lake family services recently, to inquire about counseling, as my husband and I just separated mothers day weekend. But they rather callously offer nothing..... I can’t stop wondering if I had any luck these last two years finding ANY accessible mental health support at all, this may have been avoided. It has really just all been too much to sort out myself. We so desperately are in need of help...... I am completely lost at this point....... When you picture Northern California’s wine country, Lake County is not what comes to mind. It is among the poorest counties in California, with a median household income of just over $40,000 a year and a poverty rate just under 20 percent. It ranks among the top counties statewide in annual opioid deaths. It lags in internet and computer accessibility. And nearly 14 percent of its residents have a disability—more than twice the state average. Fire, of course, does not discriminate on the basis of race or class or ability, but that does not mean survivors bear an equal burden. A 2018 study by researchers at the University of Washington and the Nature Conservancy found that wildfires hit low-income communities harder than they do their wealthier counterparts, and it’s easy to see why. Some wealthy Californians have hired private firefighting brigades to defend their estates; many poorer families lack the financial resources to take even basic preventative measures, such as trimming trees and clearing brush. When their homes burn, their insurance is less likely to cover the costs—if they have insurance at all. In the words of Rubinoff, from Legal Aid: “Recovery is not equal.” Nor is its impact on mental health. A 2017 report by the Substance Abuse and Mental Health Services Administration concluded that less wealthy, less educated survivors are more likely to suffer from depression or post-traumatic stress in the aftermath of disasters. In communities that already lack resources, the psychological fallout can be devastating. California as a whole faces a shortage of mental-health professionals, which the governor’s office has predicted will worsen in the coming years—and that was before the pandemic. In rural areas, it is especially pronounced. Janet Coffman, a health-policy professor at UC San Francisco, says wildfires are putting “additional strain on the behavioral-health system in places that were already struggling to meet needs.” Such is the case in Lake County. According to a 2015 Medical Board of California survey, the county does not have a single psychiatrist who provides patient care for at least 20 hours a week. And while it does have psychologists, it does not have enough. In a remote community like Cobb, accessible—and escapable—only by steep mountain roads with nauseatingly sharp switchbacks, finding mental-health professionals can be especially hard. [Read: Why are there so few doctors in rural America?] Four and a half years after the Valley Fire, Ellie has given up looking for mental-health treatment. She and Liam saw a couple’s therapist for a while, but after 10 sessions they couldn’t afford to continue. On a cold, bright morning in February, as she drove down the road she’d used to evacuate years earlier, panic seized her, and everything went dark. She woke up in a parking lot with the sun in her eyes and an oxygen tube in her nose and paramedics all around her. Allison, too, still has panic attacks, but not as often as she once did. She lives with her boyfriend near Los Angeles, where she freelances as a makeup artist, mostly for student productions and commercials. Her dream is to do makeup for major horror movies. She still wears long pants and hoodies to hide her scars. A burn scar, in fire science, is the land a wildfire claims. For a long time, this was something of a misnomer. A scar recalls the wound that made it; it is a matter of memory. But fire was just the opposite: In the same way that the mind lets go of the extraneous to make way for the essential, flames erased excess foliage to make space for new growth. The forest burned, but in time it healed. Now it really does scar. The most fearsome modern wildfires don’t just burn overgrowth and excess; they incinerate entire ecosystems, and sometimes those ecosystems don’t regenerate on their own. Fire, once a natural mechanism of forgetting, has become an unnatural mechanism of remembering. Someday not long from now—maybe this summer, maybe next year, maybe the year after—a new fire will ignite near Allison or her family. She’ll smell the smoke or hear the news. And when she does, her heart will quicken, and her chest will tighten, and her mind will jump back once more to that late-summer evening in 2015, to the fire on the mountain and the smoke in the sky, and it will all begin again. from https://ift.tt/3eKBo90 Check out http://natthash.tumblr.com On this episode of the podcast Social Distance, staff writer James Hamblin and executive producer Katherine Wells discuss the perils of air travel and the best ways to prepare for it. Listen here: Subscribe to Social Distance on Apple Podcasts, Spotify, or another podcast platform to receive new episodes as soon as they’re published. What follows is an edited and condensed transcript of their conversation. Katherine Wells: We've got a question for you from an anonymous person: I am a healthy 76-year-old thinking about taking a nonstop flight from Nevada to Baltimore. I want to see my daughter and her family, including my grandkids, who have been fantastic about quarantining. I could self-isolate in their basement for the flight. I have an N-95 mask and gloves and a protective face shield. Icing on the cake—I can wear a diaper to avoid public restrooms. Should I get on that plane? James Hamblin: The answer for her, just to cut right to it, is that she should get on the plane. She shows, just in that question, a level of vigilance and attentiveness—that if everyone were that thoughtful and careful about the precautions they took—we’d all be able to travel safely. The air in the cabin of a plane is constantly turning over. A lot of new air is coming in from the outside and whatever air is recirculated is run through these high efficiency HEPA filters, the same things they use in hospitals. They're rated to catch 99.9 percent of viruses and the whole cabin's air is supposed to turn over every two to three minutes. The chance of spreading a virus widely within the cabin of a plane is next to zero as long as that system is on. And there haven't been confirmed cases of coronavirus spread on airplanes to more than one other person ever since we started having people rigorously wear masks and told sick people to definitely not travel. There have been cases where sick people have traveled internationally and people around them have not gotten sick. Wells: Okay. But you have no control over the other people on the plane and there are many well-documented examples of people not wearing masks on planes, including recently Ted Cruz. Does that change things? Hamblin: Right. There is a theoretical possibility that you get seated next to someone who has been really inconsiderate and is symptomatic and refuses to wear a mask. And I don't know what the recourse airlines have in compelling them to. But we haven't heard about violent showdowns where someone's refusing to wear a mask. It seems that people mostly have been pretty good about that. Wells: But what if she walks on the flight and it's full and the person sitting next to her either doesn't have a mask or is wearing it incorrectly? Hamblin: Yeah. That's an unfortunate situation but from what we're seeing there aren't reports of lots of transmission on planes, especially since people started taking these precautions. So, yes, it's a risk—but it's a very small risk. I think that as more and more people start to travel, there's probably going to be some interesting confrontations and maybe even legal battles about this. Wells: I'm going to tell you what I would do if I were her in that situation. I would insist to the flight attendant that I needed a different seat and say that I'm an at-risk person and I can't sit next to the person. Hamblin: Yeah, I think that would be a great move. If it's a full flight your options might be more limited. But I just have to think that there's enough collective spirit right now that it wouldn't just be the flight attendant scolding that coughing person who refuses to wear a mask it would be like the entire seven rows all around that person. [laughs] Wells: All right. Here's another question. What about public restrooms? She's going to wear a diaper to avoid public restrooms. Is that what she should do? You've told us about toilet plumes. It seems like public restrooms have the potential to be dangerous, right? Hamblin: You should not have to wear a diaper. Public restrooms are supposed to have ventilation systems that suck air out of the restroom and anything lingering in the air is not lingering long. Wells: Do airplane bathrooms have that? Hamblin: Airplane bathrooms have ventilation like the rest of the plane. One thing is that you should still wear a mask. I wouldn't assume it's safe just because you're alone. I would still wear the mask. We know that flushing a toilet has the capacity to aerosolize virus—if there was virus in the stool that was in that toilet. We don't know how much virus would have to be present in order to infect someone and airplane bathrooms are kind of weird. They don't have the same swirling water mechanisms—they just suck down. I don't believe they have specifically been studied as a contributor. Wells: So, the most important thing is: if you're going to use a public restroom, it's very important to wear the mask. Hamblin: Right. There's one important caveat to this discussion. In 1977, there was a flu outbreak on a plane. The plane was on the tarmac waiting and they turned off its ventilation system. 36 out of 54 people on the plane got the flu. Wells: How long were they sitting on the plane? Hamblin: Four-and-a-half hours. This was not a brief turning off of the system. This is not a reason to have your heart stop if they turn it off briefly. But it should not be practice that they are turning off the ventilation system and having people sit together right now and maybe they shouldn't ever do that. So there's that. And the other issue is deplaning and boarding where they tend to turn the air off. And some airlines are thinking of creative ways to try to make that process more efficient so you're not sitting there for 20 minutes after the plane has landed. Wells: I know that your answer to the original question is, she should get on the plane. But everything you're telling me—if it were me—I'd be like, I'm not getting on that plane. Hamblin: It's a calculated risk and if you're 76 and you want to go see your family and the other alternative is waiting two years? That changes the equation. Wells: It sounds like what you're describing is the kind of calculation that is always going to be very individual and that we have to build this muscle for risk calculation if we're going to live this way for the next few months or even years. Hamblin: Exactly. And we can all collectively lower risk if we try to limit things like travel to instances when we really feel we need to. from https://ift.tt/2B4RtbC Check out http://natthash.tumblr.com Absent a treatment or vaccine, the coronavirus won’t stop spreading until we reach herd immunity. On this episode of the podcast Social Distance, James Hamblin details what we know and don’t know about how to get there. Listen here: Subscribe to Social Distance on Apple Podcasts, Spotify, or another podcast platform to receive new episodes as soon as they’re published. What follows is an edited and condensed transcript of their conversation. Katherine Wells: Hey Jim, what have you been thinking about? James Hamblin: Something I don’t know much about, which is complex mathematics—specifically chaos theory. Wells: Why have you been looking into chaos theory? Hamblin: I’m trying to understand why there is so much variation in what we’re seeing with COVID-19 and, I guess, how this all ends. Wells: My understanding from our conversations is that, at first, we thought there was going to be a vaccine and we were going to have to hang tight until that. Now it seems like we don’t really have a way to suppress the virus—we failed at a coordinated national strategy to keep things in check until we have a vaccine. My understanding is that where this is headed in the U.S. is herd immunity. Is that right? Hamblin: Yeah, but what do you know about what herd immunity is? Wells: Herd immunity is the idea that enough people in a particular community get the virus and develop antibodies. With antibodies, we assume they are immune for some period of time—although we haven’t totally proven that, but it’s a widespread assumption. If enough people become immune, then people who are not immune are very unlikely to get the virus. The rate of transmission goes down because there are fewer people who can possibly get it. It’s not like everyone in a community has to get it. I think I’ve heard 40 percent to 70 percent of people need to get antibodies in order to slow the spread enough that the virus might die out or be at a really, really low level. Is that correct? Hamblin: Well, mostly. And that’s how I would have described the term before I started looking into it more. Back in February, I wrote an article called “You’re Likely to Get the Coronavirus.” In it, Marc Lipsitch, who’s a really smart and well-respected epidemiologist at Harvard, said the number was somewhere between 40 percent and 70 percent. Back then, the U.S. had like five cases and he was making a qualitative point. He was basically saying, Listen, this is going to spread really widely. It’s probably much further spread than we know about. He has since changed the estimate a little bit. He now puts it at 20 percent to 60 percent. Wells: That is a wide range. Hamblin: Yeah, that’s what I said, and the range matters. If you have a case-fatality rate of 1 percent, which is about where we are, that’s a difference of, like, 30 million people globally. Wells: Thirty million deaths? Hamblin: Yeah. Wells: Got it. So whether we get to herd immunity at 20 percent or 60 percent is a hugely consequential thing. Hamblin: Exactly. Wells: I think I understand the basic premise, but I don’t understand how 20 percent could be possible. Hamblin: It doesn’t immediately make sense that it could be so low, just from a biological and medical perspective, which is why it gets into these complex mathematical phenomena. I think it clicked for me when I talked to Gabriella Gomez. Gabriella is a mathematician who has collaborated with Lipsitch in the past and she’s currently leading this international coalition of researchers to try to model where this pandemic is headed. She said she’s very confident that the threshold for herd immunity seems to be 10 percent to 20 percent. Wells: Ten percent to 20 percent?! Hamblin: That’s based on models of multiple countries in Europe, so it’s not necessarily extrapolatable—and again, I should say that no one else that I spoke with thinks it’s that low. But everyone agrees that it’s theoretically within the realm of possibility. Her theory is that a lot of other models are underestimating the idea of heterogeneity. Wells: What does that mean? Hamblin: She thinks that this is not a model where we really see predictable outcomes. You might have a sick person go onto a plane and infect dozens of others, and you might have a sick person and fly and create no more cases. Those events start to seem sort of random. Wells: And why would that be? Do we have theories? Hamblin: We don’t know. These are things we’ll find out later. But one of the researchers mentioned that it could be something like the density of people’s nose hairs. Wells: The case for nose hairs. [Laughs] Hamblin: That’s just one of many variables. There are at least some physiological differences that will make one person more likely to become infected and have the virus thrive and spread within them. Wells: Right. Does that mean there’s some percentage of people that just aren’t susceptible for some reason? Hamblin: No, everyone is susceptible. But even a small variation in how susceptible you are to a given exposure makes broader prediction difficult. And that’s just one thing that makes prediction difficult. You also have these super-spreaders, who are shedding a ton, while some people might be shedding very little. Some people come in contact with tons of other people, and some people totally isolate. Once you start trying to make models about what the level of herd immunity would be, you have to factor in all these variables that are different than if you were just vaccinating everyone. Wells: Is this what chaos theory helps explain? Hamblin: Well, chaos theory comes into play when you’re looking at these outcomes that don’t seem possible. Mathematicians like Gomez try to find order and make predictions within that system even when things seem random. The field of chaos theory grew out of findings from applying mathematics to try to predict weather, which is very complicated. It should be really predictable, but it’s extremely difficult to predict because a slight change in one circumstance has huge downstream effects. Wells: Is that like “A butterfly flaps its wings and a year later there’s a tsunami”? Hamblin: Exactly. It is called the butterfly effect. Whenever someone made a decision to get on the first international flight, that wasn’t just one act. It had massive consequences. And when effects of single actions compound like that, and also when you have these many variables for potential outcomes, models vary really dramatically. That’s not to explain exactly why 20 percent is right, but it explains why it’s possible. Wells: This is so frustrating because it’s like there could be an extremely hopeful thing but no guarantees so we can’t really do anything about it. Hamblin: I think this is helpful—it’s information about how this is working. And I actually think it is actionable, because it tells us that we have the capacity to change this threshold. It depends, in large part, on us. There is a sort of fatalism in advocating, Oh, just let it run wild because we’re going to hit the same number of deaths no matter what. Wells: Not that we don’t want to protect the most vulnerable people, but it did seem as though the number of deaths was essentially going to be the same whether it went fast or slow. Hamblin: Yeah, but herd immunity is effectively like social distancing. It means you’re taking people out of the equation. It means that when you’re in a crowded restaurant where 80 percent of people are immune, then, functionally, only 20 percent of the people are in the restaurant. Wells: If we can find ways to live this way until there is a vaccine, then the vaccine becomes quite relevant again. Hamblin: Right. I think it will vary from place to place, but if we keep social-distancing measures in place, we won’t see a big spike. It’s not 100 percent, but it seems unlikely. I guess if there’s a main takeaway, it’s that herd immunity is not this magical number. Herd immunity is a concept and we create it in different ways. It’s a concept that reminds us we’re all in this together and you are effectively serving as a number in the immune group when you behave responsibly. from https://ift.tt/3jarVuO Check out http://natthash.tumblr.com Over 40 percent of all coronavirus deaths in America have been linked to nursing homes. How did it happen, and how bad could it get? Staff writer Olga Khazan joins James Hamblin and Katherine Wells on Social Distance to explain. Listen here: Subscribe to Social Distance on Apple Podcasts, Spotify, or another podcast platform to receive new episodes as soon as they’re published. What follows is an edited and condensed transcript of their conversation. Katherine Wells: You've been reporting and talking to people who are working in nursing homes and living in nursing homes. What are you hearing? Olga Khazan: Coronavirus has been getting into nursing homes. And the second you have one infection—especially early on in the pandemic—it was basically spreading like wildfire, and inevitably leading to deaths because as we know, older people are more susceptible to dying from the virus. A lot of the people who have been talking about reopening have said: Well, let's reopen the economy and then let's just protect the vulnerable. That's usually how it's phrased, which often means nursing homes. But they have completely not been protected. By no definition of being protected. When you have 40 percent of all deaths in nursing homes, that shows you that something is going terribly, terribly wrong. James Hamblin: Was it inevitable that nursing homes would be hit really hard? Khazan: Actually, no. I talked to a few examples of nursing homes in other countries. In Hong Kong, there were no nursing-home deaths or even cases, basically because they were freaked out by SARS. They had a really bad SARS outbreak in Hong Kong in 2003. That caused them to come up with this new plan for nursing homes in case of an outbreak like this. They stocked up on masks. They isolated nursing-home residents in special hospital wards instead of in the nursing homes. They had government-trained infectious-control officers stationed inside the nursing homes. They really took it seriously, and it worked. Starting in January of this year, they set this plan in motion and it prevented nursing-home deaths. And I think, hearing the Hong Kong example, people might think, well, you have to have a different government in order to do that but there was an example in Baltimore. The Maryland Baptist Aged Home did something similar and also prevented any coronavirus deaths. Hamblin: How did they do that? Khazan: They basically stopped family visits in early February, which is pretty early. They stopped having the residents do community meals. They stopped having lots of foot traffic into the nursing home—vendors and delivery drivers, people like that. They brought in extra cleaning. They started screening their staff really intensively for their temperature and their symptoms and what they've been doing outside of work. Hamblin: It seems like the resources that you would need to do that grow exponentially as the outbreak is bigger and bigger in a community. It might be possible if you've got the virus relatively contained in a certain city to keep your nursing homes safe. But if there's this huge outbreak all around, it's going to be really hard to keep people in the nursing homes safe. Khazan: Yeah, that's what experts told me. Essentially, if you have a big outbreak outside the nursing home, there's a really high chance you're going to have an outbreak inside the nursing home. Workers will leave work and go to the grocery store. They brush up against someone who has it. They bring it back into the home. When you don't have masks, when you don't have tests ... A lot of experts believe that asymptomatic staffers essentially brought the virus into nursing homes and were never tested, and it kind of spread silently for a while earlier this spring. The Centers for Medicare and Medicaid Services (CMS) is the agency that regulates nursing homes, and it could have stepped in and given them masks, for example. Guidance from CMS—even on when to use masks—came really late in the game. Hospitals were prioritized and they got priority for the stockpile of masks. But nursing homes weren't. They were competing against large hospitals and states trying to get extra PPE supplies, paying tons of money for masks that were not actually effective or that were in some cases defective in various ways. In early June, data showed that 250 nursing homes had no masks left and 800 more were a week away from running out. The federal government left it up to individual nursing homes to protect their residents. And what these nursing homes are saying is: We don't have the money to do that. We're not trained to do this. We don't have a stockpile of masks. And we don't have access to tests. That's where it all broke down. from https://ift.tt/2B7Wcti Check out http://natthash.tumblr.com Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. There is no mystery in the number of Americans dying from COVID-19. Despite political leaders trivializing the pandemic, deaths are rising again: The seven-day average for deaths per day has now jumped by more than 200 since July 6, according to data compiled by the COVID Tracking Project at The Atlantic. By our count, states reported 855 deaths today, in line with the recent elevated numbers in mid-July. The deaths are not happening in unpredictable places. Rather, people are dying at higher rates where there are lots of COVID-19 cases and hospitalizations: in Florida, Arizona, Texas, and California, as well as a host of smaller southern states that all rushed to open up. The deaths are also not happening in an unpredictable amount of time after the new outbreaks emerged. Simply look at the curves yourself. Cases began to rise on June 16; a week later, hospitalizations began to rise. Two weeks after that—21 days after cases rose—states began to report more deaths. That’s the exact number of days that the Centers for Disease Control and Prevention has estimated from the onset of symptoms to the reporting of a death. 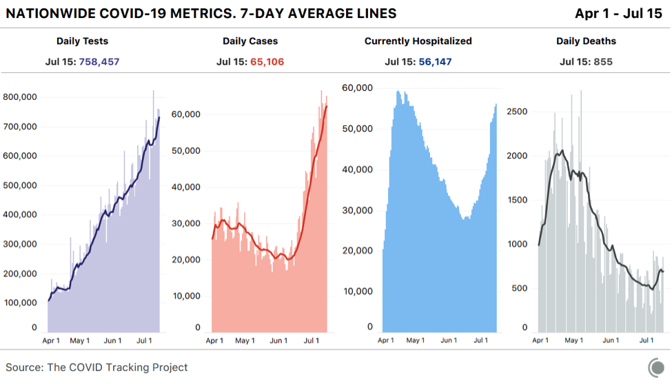
Many people who don’t want COVID-19 to be the terrible crisis that it is have clung to the idea that more cases won’t mean more deaths. Some Americans have been perplexed by a downward trend of national deaths, even as cases exploded in the Sun Belt region. But given the policy choices that state and federal officials have made, the virus has done exactly what public-health experts expected. When states reopened in late April and May with plenty of infected people within their borders, cases began to grow. COVID-19 is highly transmissible, makes a large subset of people who catch it seriously ill, and kills many more people than the flu or any other infectious disease circulating in the country. The likelihood that more cases of COVID-19 would mean that more people would die from the disease has always been very high. Even at the low point for deaths in the U.S., roughly 500 people died each day, on average. Now, with the national death numbers rising once again, there’s simply no argument that America can sustain coronavirus outbreaks while somehow escaping fatalities. America’s deadly summer coronavirus surge is undeniable. And it was predictable this whole time by looking honestly at the data. In the United States, the rising severity of the current moment was obscured for several weeks by the downward drift of cases, hospitalizations, and deaths resulting from the spring outbreak in northeastern states. Even though deaths have been rising in the hardest-hit states of the Sun Belt surge, falling deaths in the Northeast disguised the trend. 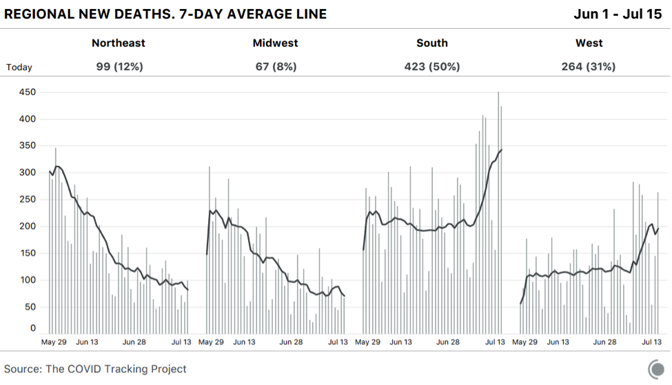
It is true that the proportion of infections in younger people increased in June and July compared with March and April. And young people have a much lower risk of dying than people in their 60s and older. But, at least in Florida, where the best age data are available, early evidence suggests that the virus is already spreading to older people. Additionally, analysis of CDC data by The New York Times has found that younger Black and Latino people have a much higher risk of dying from COVID-19 than white people the same age. According to the racial data compiled by the COVID Tracking Project in concert with the Boston University Center for Antiracist Research, Latinos in Arizona, California, Florida, and Texas are 1.3 to 1.6 times more likely to be infected than their proportion of the population would suggest. It is telling that despite outbreaks all over Texas in recent weeks, the border region has been leading the state in deaths per capita. Even with cases surging, if hospitalizations were not rising, that might suggest that this outbreak might be less deadly than the spring’s. But hospitalization data maintained by the COVID Tracking Project suggested otherwise as early as June 23. On that date, hospitalizations began to tick up across the South and West, and they have not stopped. It’s possible we’ll match the national peak number of hospitalizations from the spring outbreak over the next week. 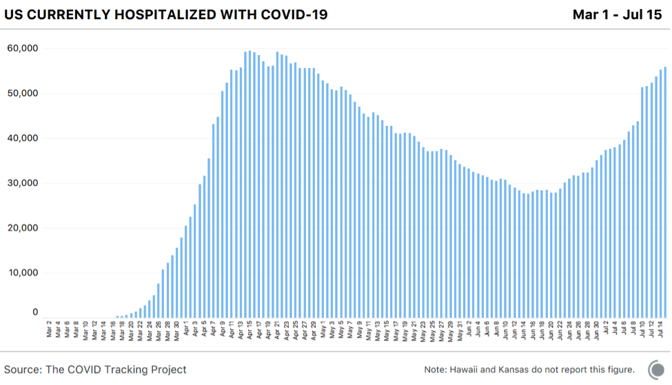
Even if better knowledge of the disease and new treatments have improved outcomes by 25 or even 50 percent, so many people are now in the hospital that some of them will almost certainly die. There was always a logical, simple explanation for why cases and hospitalizations rose through the end of June while deaths did not: It takes a while for people to die of COVID-19 and for those deaths to be reported to authorities. So why has there been so much confusion about the COVID-19 death toll? The second surge is inconvenient for the Trump administration and the Republican governors who followed its lead, as well as for Mike Pence, the head of the coronavirus task force, who declared victory in a spectacularly incorrect Wall Street Journal op-ed titled, “There Isn’t a Coronavirus ‘Second Wave.’” “Cases have stabilized over the past two weeks, with the daily average case rate across the U.S. dropping to 20,000—down from 30,000 in April and 25,000 in May,” Pence wrote. In the month since Pence made this assertion, the seven-day average of cases has tripled. Several individual states have reported more than 10,000 cases in a day, and Florida alone reported 15,000 cases, more than any state had before, on an absolute or per capita basis. 
But there’s another reason for some of the confusion about the severity of the outbreak right now. And that’s the perceived speed at which the outbreak initially landed on American shores and started killing people. The lack of testing let the virus run free in February and much of March. As my colleague Robinson Meyer and I put it at the time, “Without testing, there was only one way to know the severity of the outbreak: counting the dead.” And that is how we figured out how bad the outbreak was. Thousands began dying in the greater New York City area and a few other cities around the country in early April. The seven-day average for new cases peaked on April 10, followed by the peak of the seven-day average for daily deaths just 11 days later. Everything seemed to happen at once: lots of cases, lots of hospitalizations, lots of deaths. But some of this is also the compression of memory. Most of us remember the deaths in March beginning as quickly as the cases, especially given the testing debacle. That’s not exactly what happened, however. The nation did, in fact, see cases rise weeks before the death toll shot up. There was a time in March when we had detected more than 100 cases for each death we recorded. This is a crucial metric because it gets at the perceived gap between cases and deaths. And it tells us that we did see a lag between rising cases and deaths back in the spring. During the slow-decline phase in May, the case-to-deaths ratio fell to about 20. Then, this summer, the case-to-death ratio began to rise in early June. On July 6, the ratio hit 100 again, just like in the spring. But as in spring, this was not a good sign, but rather the leading indicator that a new round of outbreaks was taking hold in the country. And, indeed, a week ago, this ratio began to fall as deaths ramped up. 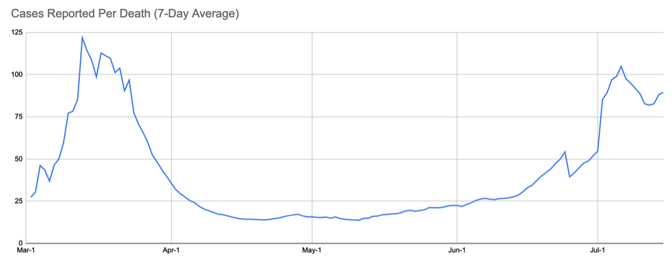
The U.S. came most of the way down the curve from the dark days of April, and now we’re watching the surge happen again. The testing delays, the emergency-room-nurse stories, the refrigerated morgue trucks—the first time as a tragedy, the second time as an even greater tragedy. One must ask, without really wanting to know the answer, How bad could this round get? By the absolute or per capita numbers, the U.S. stands out as nearly the only country besides Iran that had a large spring outbreak, began to suppress the virus, and then simply let the virus come back. No other country in the world has attempted what the U.S. appears to be stumbling into. Right now, many, many communities have huge numbers of infections. When other countries reached this kind of takeoff point for viral spread, they took drastic measures. Although a few states like California are rolling back reopening, most American states are adamant about opening into the teeth of the outbreak. And this level of outbreak will not stay neatly within a governor’s political boundaries. There’s no way to win this state by state, and yet that’s exactly what we’re attempting. From the look of the map, the South and West—regions with a combined 200 million people—are in trouble. 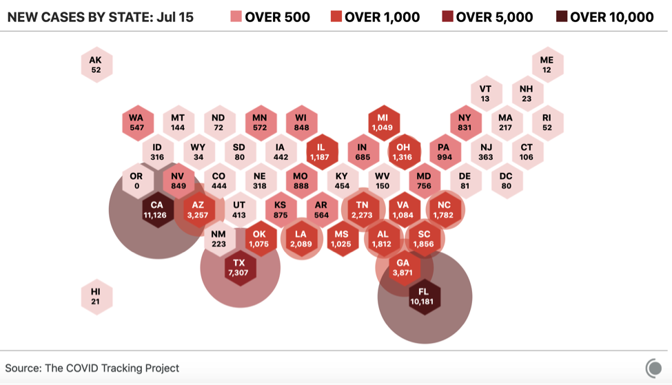
The regional variation of the American outbreak is crucial to understanding both what happened and what’s going to happen next. Nationwide, the U.S. deaths per million tally—a hair under 400—is in the top ten globally. But look just at the Northeast’s 56 million people, and the death rate is more than double the national average: 1,100 deaths per million. By contrast, the South and West—where SARS-CoV-2 is burning through the population—are much more populous than the Northeast. If those areas continue to see cases grow, they could see as many deaths per million as the Northeast did but multiplied by a larger number of people. At 1,100 deaths per million, the South and West would see 180,000 more deaths. Even at half the Northeast’s number, that’s another 69,000 Americans. In truth, the fan of possibilities is probably wider. Looking at individual states, there was tremendous variation from low-death states like New Hampshire (288 deaths per million), to extremely high-death states like New Jersey (1,750 deaths per million), and a bunch in between, like Massachusetts (1,20892); Washington, D.C. (805); and Pennsylvania (539). 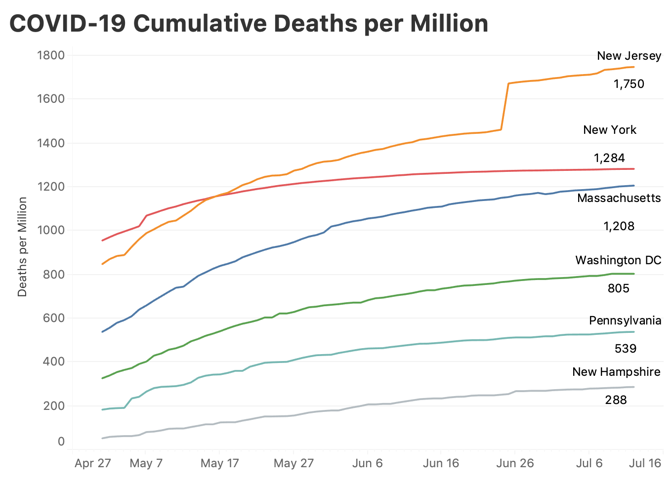
It’s possible that the summer-outbreak states could follow the lower death trajectory traced by Pennsylvania or Washington, D.C. Right now, only Arizona, at 307 deaths per million has crossed even the lowest line above, New Hampshire; there is a lot of room for things to get worse, even if they do not come close to equaling the horrors of the spring. New York City is and probably will remain the worst-case scenario. New York City has lost 23,353 lives. That’s 0.28 percent of the city’s population. If, as some antibody-prevalence surveys suggest, 20 percent of New Yorkers were infected, that’s an infection-fatality rate of more than 1.3 percent, which exceeds what the CDC or anyone else is planning for. To put it in the same terms discussed here, New York City saw 2,780 deaths per million people. A similar scenario across the South and West would kill over 550,000 more Americans in just a few months, moving the country to 680,000 dead. It is unthinkable, and yet, 130,000 deaths—the current national death toll—was once unthinkable, too. That’s still not the worst-case scenario for a truly uncontained outbreak, in which serious measures are not taken. For months, most public-health officials have argued that the infection-fatality rate—the number of people who die from all infections, detected and undetected, symptomatic and asymptomatic—was somewhere between 0.5 and 1 percent. The CDC’s latest estimates in its planning scenarios range from 0.5 to 0.8 percent. Take that lower number and imagine that roughly 40 percent of the country becomes infected. That’s 800,000 lives lost. The point in laying out these scenarios is not that we’ll reach 300,000 or 800,000 American COVID-19 deaths. That still seems unlikely. But anyone who thinks we can just ride out the storm has perhaps not engaged with the reality of the problem. As the former CDC director Tom Frieden has said, “COVID is not going to stop on its own. The virus will continue to spread until we stop it.” The lack of containment by American authorities has resulted in not only lost lives, but also lost businesses, savings accounts, school years, dreams, public trust, friendships. The country cannot get back to normal with a highly transmissible, deadly virus spreading in our communities. There will be no way to just “live with it.” There will only be dying from it for the unlucky, and barely surviving it for the rest of us. from https://ift.tt/2DEkpIm Check out http://natthash.tumblr.com
Dear Dr. Hamblin, I’m a healthy 76-year-old thinking about taking a nonstop flight from Las Vegas to Baltimore. I want to see my daughter and her family, including my grandkids, who have been fantastic about quarantining. I could self-isolate in their basement. For the flight, I have an N95 mask and gloves, and I could get a protective face shield. And as icing on the cake, I can wear a diaper to avoid public restrooms. Should I get on that plane? Anonymous I think you should feel confident about getting on that plane. The measures you’re taking should keep you safe. But more than anything else, the thoughtfulness you show in the planning here suggests you’ll do everything vigilantly. Our safety in confined indoor spaces like airplanes depends on the collective efforts of individuals, and you’re clearly not the type to just wear a mask around your chin or performatively wash your hands only if people are looking. That said, I don’t think you need to wear a diaper. Every airport bathroom in the United States should have functional exhaust fans that expel any lingering, potentially infectious toilet plume after you flush. If you’re wearing a mask, the ordeal should be a low-risk proposition. The same goes for the flight itself: An airplane toilet shouldn’t aerosolize the virus any more than a typical toilet. But the surfaces in airplane bathrooms could very possibly be coated in the virus, because every part of the tiny room is touched regularly by many people. I’d operate under the same assumption in any bathroom right now, and wash my hands accordingly. [Read: Air travel is going to be very bad, for a very long time] What makes flying especially risky, at least theoretically, is the air on the flight. A plane involves many people in an enclosed space for prolonged periods. Mucus membranes in your nasal passages dry out on a plane, making them more prone to being colonized by a virus. But the air on a flight should be as safe as or safer than other enclosed spaces where people are spending prolonged periods together. Unlike many homes or offices, the air in a plane is constantly turning over, with outside air sucked into the cabin and old air pushed out. Any air that is recirculated is supposed to be run through a HEPA filter that can catch almost any virus. The ventilation is probably not as good as if all the windows on the plane were open, but, well, that would cause it to crash and everyone inside to suffocate. Still, it’s better than sitting in a car with the air-conditioning going, recirculating air while everyone inside sits in the stew. The air on planes can be an issue when their ventilation system is shut off, even temporarily, such as when they’re stuck on a tarmac for one of those always-unclear reasons. This situation is credited with one well-known influenza outbreak, in which 38 of 54 people on a plane were infected after sitting on a tarmac for three hours without air circulation. No such instances of cabinwide spread have been reported with the coronavirus, though there have been isolated reports of transmission, mostly to a single nearby passenger. The worst reported incident was in early March, when Vietnam’s health ministry linked a dozen cases to a long flight from London to Hanoi. To be safe, planes shouldn’t sit idle with their ventilation system off for long. If yours is doing that, demand that it be turned back on. The air system is also typically turned off during boarding and deplaning, leading some airlines to get creative about new boarding patterns that minimize how long it takes. If a more efficient boarding process were always possible, I wish they’d done it a long time ago. In any case, I wouldn’t rush to be the first person to board the plane. It may also help to turn on the personal fan above your head. At least, it can’t hurt. That air should be filtered, and on the off chance that someone sitting very close to you has the virus and is spreading it around, this fan might help dilute it and shoo away anything hanging in the air near you. Overall, the air in a plane’s cabin should completely turn over every three minutes. When that sort of ventilation system is combined with people correctly wearing high-quality masks, and declining to travel if they are at all symptomatic or have had contact with people who are sick, the risk of an outbreak on a plane should be close to zero. The main concern with air travel, then, is less about spreading the virus on the plane than about people spreading the virus once they arrive. The specific concern is transporting the virus from a hot spot to a place that has things under control, especially in the United States, where coronavirus cases are surging in most but not all states. Your plan to isolate for two weeks upon arrival is a good one. New York, Connecticut, and some other states are already requiring incoming travelers to do this; it should become standard policy. Self-isolating can be difficult to do, especially when you’re visiting family, but it’s very important. I think you could safely hang out in the backyard or on the porch, at a distance. It doesn’t need to be a hostage situation in which your relatives lower food down the stairs using a pulley system. [Read: I just flew. It was worse than I thought it would be.] That brings me back to the precautions you plan on taking. Unlike in many other countries, the U.S. currently has no restrictions on domestic travel. If you wanted to, you could start gallivanting around the country without anyone stopping you, even if you feel ill. But just because you can fly doesn’t mean you should. Staying safe while traveling is going to come down to basic conscientiousness. If everyone had the vigilance you show here, we’d be in a lot better place—as a country and as a world. Before all of this, I used to wish people “safe travels” in a way that was kind of meaningless. Now it’s more of an earnest injunction to be mindful of not only your safety, but also the safety of everyone around you. Act as though you are contagious, even though you should be traveling only when you’re confident that you’re not. Safe travels. “Paging Dr. Hamblin” is for informational purposes only, does not constitute medical advice, and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. By submitting a letter, you are agreeing to let The Atlantic use it—in part or in full—and we may edit it for length and/or clarity. from https://ift.tt/2Ce4oZq Check out http://natthash.tumblr.com 
Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. Seven years ago, the White House was bracing itself for not one pandemic, but two. In the spring of 2013, several people in China fell sick with a new and lethal strain of H7N9 bird flu, while an outbreak of MERS—a disease caused by a coronavirus—had spread from Saudi Arabia to several other countries. “We were dealing with the potential for both of those things to become a pandemic,” says Beth Cameron, who was on the National Security Council at the time. Neither did, thankfully, but we shouldn’t mistake historical luck for future security. Viruses aren’t sporting. They will not refrain from kicking you just because another virus has already knocked you to the floor. And pandemics are capricious. Despite a lot of research, “we haven’t found a way to predict when a new one will arrive,” says Nídia Trovão, a virologist at the National Institutes of Health. As new diseases emerge at a quickening pace, the only certainty is that pandemics are inevitable. So it is only a matter of time before two emerge at once. “We have to prepare for a pandemic to happen at any time, and ‘any time’ can be when we’re already dealing with one pandemic,” Cameron told me. I first worried about the possibility of a double pandemic in March. Four months ago, it felt needlessly alarmist to fret about two rare events happening simultaneously. But since then, federal fecklessness and rushed reopenings have wasted the benefits of months of social distancing. About 60,000 new cases of COVID-19 are being confirmed every day, and death rates are rising. My worry from March feels less far-fetched. If America could underperform so badly against one rapidly spreading virus, how would it fare against two? COVID-19 has made clear what happens when even powerful, wealthy countries are inadequately prepared for rare but ruinous events. Months into the pandemic, international alliances are strained, resources are diminished, and experts are demoralized. The longer this fiasco drags on, the more vulnerable America becomes to further disasters: inbound hurricanes, wildfires, and many other viruses that lie in wait. SARS-CoV-2, the coronavirus that causes COVID-19, is just one of many coronaviruses that exist in bats and other wild animals. Several strains of influenza with pandemic potential are lurking in pigs and poultry, and some have repeatedly infected farmers over the past decade. Wild mammals harbor an estimated 40,000 unknown viruses, a quarter of which could conceivably jump into humans. Changing climate and shrinking habitats have brought those viruses into closer contact with people and livestock, while crowded cities and air travel hasten their spread. “If another pandemic happens, it will follow the same path the first one took, carved out by the world we created,” says Jessica Metcalf, an infectious-disease ecologist at Princeton. Certain traits increase a pathogen’s pandemic potential. Those that spread via bodily fluids (Ebola), contaminated food and water (norovirus), or insect bites (Zika) are slower to spread around the world. By contrast, respiratory viruses like flu, which spread through coughs, sneezes, and exhalations, could conceivably travel fast enough to overlap with COVID-19. [Read: How the pandemic will end] Many countries are on high alert for such viruses, primed by their COVID-19 ordeal in the same way that East Asian countries were primed at the start of this pandemic by their previous run-ins with SARS and MERS. But waning global solidarity is a problem. “Our international laws are based on a bargain that countries will rapidly notify each other [about emerging diseases] and, in exchange, they’ll have protection against the economic impacts of sharing that info,” says Alexandra Phelan of Georgetown University, who works on legal and policy issues related to infectious diseases. That compact was violated during COVID-19, after China suppressed information about the outbreak and other countries quickly implemented travel bans. The U.S. is now on the receiving end of many such bans. Having failed to lead the best-prepared nation in the world against one pandemic, Donald Trump has made it more vulnerable to another. He has, for example, frayed international bonds further by trying to pull the U.S. out of the World Health Organization. Whether he has the legal authority to do so is still unclear, but even if the threat is empty, “some of the effects will be immediate,” says Loyce Pace, the president of the Global Health Council. U.S. officials and experts will start disengaging from international institutions, and that might encourage other nations to follow suit. This won’t just harm the WHO at the time when it is most needed, but will also further diminish America’s already damaged international standing. A country that has badly mishandled its own outbreak, that has bought up the world’s stock of important drugs, and that has petulantly withdrawn from global alliances is less likely to receive warnings or support if a new crisis emerges. 
There is an optimistic scenario if a second virus begins to spread: The new pathogen finds it harder to move around an alert world, is rapidly detected wherever it arrives, and fizzles out because cautious citizens have their guard up. As long as people stay vigilant against the current pandemic—keeping their distance, wearing masks, avoiding indoor crowds—they should theoretically be guarded against a second respiratory virus. It used to be common for measles and pertussis to interfere with each other, so that if one spiked, the other would subside. That might be because kids who got one disease would stay home, reducing their risk of the other. “It’s nothing to do with a vaccine or the immune system,” says Sarah Cobey, an immunologist at the University of Chicago. “It’s just people being careful.” The same tests that are being used to diagnose COVID-19 could also be tweaked to cover the new pathogen. One company is already developing a fast “multiplex” test that could look for four respiratory viruses—the new coronavirus, two types of flu, and respiratory syncytial virus (RSV)—in a single nasal swab. And if the new pathogen is a flu strain, existing vaccines could be tweaked to protect against it. That would still take several months, but the existence of a seasonal flu vaccine offers an invaluable head start. [Read: We don’t even have a COVID-19 vaccine, and the conspiracies are here] This future is easier to imagine in countries like South Korea, New Zealand, and Germany, which have successfully controlled COVID-19. It seems less likely in nations like the U.S., Brazil, Russia, and India, which are stretched and struggling. In such places, COVID-19 would effectively cloak the spread of any new respiratory virus with similar symptoms, which “could have a chance to take off before we realized it had,” Cameron said. A new virus would also be harder to spot because “all the resources we would normally use to detect potential viruses of concern have been redirected for COVID-19,” says Lauren Sauer, who works on disaster preparedness at Johns Hopkins Medicine. She means everything from physical equipment like swabs and storage tubes, to health-care workers who administer and process tests, to public-health experts who analyze the data or conduct contact tracing. These are either running out or burning out. A second respiratory virus would further tax the same resources that the U.S. has already failed to adequately marshal for COVID-19. Hospitals would also struggle. In many states, emergency rooms and intensive-care units are filling up. A second virus wouldn’t need to be that severe to push them beyond their capacity, deplete the shrinking supply of protective equipment, or create a logistical nightmare. “Say we had pandemic flu and COVID at the same time,” Sauer told me. “You have two groups of people who need to be sorted and separated,” lest those with only one virus infect those who have only the other. Doctors and nurses would face complicated protocols about whom they could treat, having already run on fumes for months. “People are spent,” Pace, the Global Health Council president, told me. “We are very resilient, but we have our limits.” A second virus would be especially devastating if it targeted a different slice of the populace than COVID-19. Unlike SARS-CoV-2, many respiratory viruses disproportionately affect children, and the 1918 flu pandemic was especially deadly for adults ages 20 to 40. “Something that decimates children or young people is a different ballgame,” says Zeynep Tufekci, a sociologist at the University of North Carolina and an Atlantic contributor. “It’d be economically devastating, and you’d no longer have an age group that’s protected.” The current debate about opening schools would be completely off the table. “In such a case, 1 plus 1 isn’t 2, but 10,” she adds. It’s certainly possible for people to contract multiple respiratory viruses at once, and in early spring, some adults were indeed infected with both flu and SARS-CoV-2. But it’s hard to predict what happens when two severe pathogens hit the same person. Viruses reproduce by co-opting their host’s cells, and two of them might obstruct each other by competing for the same cellular machinery. It’s also possible that one would trigger a generic immune response, like inflammation, that would make it harder for the second to take hold. Then again, it’s also possible that two severe diseases would compound each other. “The knotty heart of all these problems is the immune system,” Metcalf told me, which is so complicated that trying to understand it, much less predict it, “is just miserable.” [Read: Why the pandemic is so confusing] Untangling those knots is especially hard in the midst of a pandemic. Currently, the scientific community is hell-bent on studying COVID-19, but basic questions remain unanswered. Why do some people get sick and others do not? What’s the full range of symptoms? Why do some people infect many while many infect no one? “Look at the energy it’s taking,” says Nahid Bhadelia, an infectious-disease physician at Boston University, “and the level of uncertainty” that just one new virus creates. Scientists, much like the health-care and public-health communities, are neither infinite nor indefatigable. A second virus would more than double their burden because they would have to analyze the diseases individually, as well as any interactions between them. Mysteries would linger. Uncertainty would deepen. The vortex of confusion in which we have swirled for months would spin faster. Already, a single pandemic has pushed people toward baseless theories about deliberately engineered viruses. Such conspiracies will burn even brighter if a second improbable event occurs. 
On July 6, several reports noted that a case of bubonic plague had been detected in Inner Mongolia, a region of northern China. That should have been considered neither odd nor alarming. Plague is endemic among the region’s rodents, as it is among those of the southwestern United States. A handful of Americans come down with plague every year. The disease is treatable with antibiotics. And yet, the plague story was widely read. “Really, 2020?” wrote many a Twitter user. (Yesterday, a squirrel tested positive for plague in Colorado, prompting another wave of headlines.) The threats that draw the most attention are not necessarily the most dangerous ones. While Americans freaked out in May about so-called murder hornets, the worst locust outbreak in 70 years devastated croplands in East Africa and South Asia. While a single case of plague in China made headlines, the Democratic Republic of the Congo was being dog-piled by dangerous viruses: The nation just beat a two-year Ebola outbreak in its war-ravaged east, only to face another Ebola assault on its western flank, along with COVID-19 and the world’s largest measles outbreak. The DRC and many other countries are already living through what is functionally identical to a double pandemic—several infectious disasters, overlaying one another. The U.S. is barrelling toward the same situation. Even without a second pandemic, regular seasonal flu strains are inbound. “I’m pretty worried,” Sauer told me. The same demographic of younger adults that accounts for many of America’s surging COVID-19 cases would also drive a bad flu season. And the people who would normally prepare hospitals for such an eventuality have no time to do so. “The idea that someone could conduct a drill in the midst of all of this is not realistic,” Sauer said. “All the people with preparedness jobs have turned into COVID responders. Things are getting dropped.” [Read: The pandemic experts are not okay] As a result, the flu vaccine could be less effective. Flu viruses change constantly, and must be carefully monitored to make sure that this season’s vaccine is a decent match for currently circulating strains. It’s hard to do that with COVID-19 sapping time and energy, which “will hamper our ability to gauge and respond to what’s happening in the middle of this flu season,” says Emily Martin, who studies respiratory viruses at the University of Michigan. “It’ll also affect the vaccine of 2021.” Other known and preventable diseases will also run amok if the current pandemic continues unabated. The Centers for Disease Control and Prevention reported that in Michigan, the proportion of five-month-olds who are up-to-date on their vaccines fell from 68 percent in May 2019 to 50 percent in May 2020. Childhood vaccinations have also declined in many other states as doctor offices closed or parents canceled appointments. Global programs that fight HIV, malaria, and tuberculosis are being disrupted as workers are reassigned to fighting COVID-19, supplies run out, and labs are inundated. Vaccination programs were suspended in many countries, leading to rises in measles, cholera, and diphtheria. If such initiatives are paused too long, the world could lose decades of ground against polio—a disease that was almost eradicated. “We’ve been very close to the end of polio for a very long time, and we’re not far away from the scenario where it comes roaring back,” Pace said. “When two or more diseases cluster, interact, and are driven by some bigger phenomenon,” they are known as “syndemics,” says Emily Mendenhall, a medical anthropologist at Georgetown University. COVID-19, for example, disproportionately affects people with heart disease and diabetes, but all of these illnesses are affected by inequity. America’s legacy of systemic racism means that Black people are more likely to live in poor neighborhoods, to have less access to nutritious food and good health-care, and to work in low-wage “essential” jobs that must continue even in a pandemic. These factors make Black people more prone to both chronic illness and COVID-19, which then exacerbate each other. The syndemic concept is important because it reminds us that diseases are not just the work of viruses and other pathogens. They are also influenced by every aspect of a society, from cultural values that affect whom it cares for and ignores, to political choices that determine how it responds when challenged. To truly prepare for pandemics, whether one or two or five, the U.S. needs more than biomedical advances like vaccines and drugs. “We need to plug all the holes,” Tufekci told me. That would mean investing in long-neglected public-health systems to ensure universal access to health care, and to dismantle racist policies that have foisted the burden of disease onto marginalized communities. “Apparently the world needed to hear this, but humanity can’t leave infectious diseases behind,” Tufekci added. “We’re going to have to live with them. We’re more pandemic-friendly as a planet.” 
from https://ift.tt/3h2e4VH Check out http://natthash.tumblr.com What does the surge in coronavirus cases in the South and West mean for the country’s chances of ending the pandemic? Staff writer Alexis Madrigal joins the podcast Social Distance to discuss. Listen here: Subscribe to Social Distance on Apple Podcasts, Spotify, or another podcast platform to receive new episodes as soon as they’re published. What follows is an edited and condensed transcript of their conversation. Katherine Wells: Alexis, you have a really good handle on the latest coronavirus data. What are you seeing? Alexis Madrigal: There's a lot happening. Let's go through the four metrics that we track really closely: the tests, the cases, the current hospitalizations, and the deaths. With tests, things have been scaling up. We do many times more tests than we did back in the spring, but it's not localized in quite the same way. In the spring, the Northeast was where the bulk of the outbreak was. Now you need a lot more testing and I think we're starting to bump up against the limits of the current generation of testing that we have here in the U.S. We're hearing about supply-chain shortages, in particular pipette tips. Wells: There's a pipette-tip shortage? Madrigal: Yeah, it's kind of a necessary part of doing the laboratory work of a diagnostic test. There are a lot of parts to it—swabs can run out, there can just not be enough machines which you need to do the test. You need the chemicals that go into the test. You need the swabs that go into people's noses. And apparently, you need the pipette tips to go over your pipette. This is a real problem. All of the big labs like Quest and LabCorp are putting out advisories that their turnaround times are growing. For people who are going into a hospital, perhaps they can get tests more quickly, at least for now. But for people who are just getting tested at a drive-thru location or elsewhere, turnaround times are four, five, six, seven, eight days, which, of course, is what happened back in March and April. So, we're kind of back where we were. And the real problem is that if you want to use testing to get people to stay in their homes, if they may have COVID-19, you need fast turnaround times in order to be able to use testing for that kind of mitigation. James Hamblin: Yeah, because at that point, you're kind of through the contagious phase. Madrigal: Yeah. We now have hit this point particularly in the hotspots for the outbreak: Arizona, Florida, Texas, Louisiana, Georgia, South Carolina. Testing gets overrun when there's a surge like this. People thought they had enough testing capacity and they clearly did not. And infections are growing across basically the entire southern part of the United States and places that really hadn't been hit very hard in the first round. I think a really good example is Texas. We have hospitalization numbers for them going back to April. They were basically between like 1,000 and 2,000 people hospitalized from the beginning of April all the way to about June 8. They finally broke 2,000 on June 10. They broke 3,000 on June 19. They broke 4,000 on June 23. They broke 5,000 on June 27th. And now they're up to over 9,000 less than a month later and it doesn't really seem like there's a real end point to it right now. I don't know what that means for these southern states. When we saw stuff like this happening in the Northeast–the governors, Republican and Democrat alike—they all took pretty similar actions. They locked everything down and took intense measures. That's just not what happened in Texas and Arizona and Florida and still isn’t happening. We’re really in a different kind of situation right now. Hamblin: Yeah, I totally agree on the point that when you have this many cases—testing becomes less of an issue because you just need to lock down. That's the only effective way to stop it when you're at that level of spread. Do you think that the shortage of testing means that we're really not seeing the full scope of things in any of the states they're being hit hardest right now? Madrigal: I think that's been a meta-point all along. The data that strikes me as the highest quality is the hospitalization data. You look at the cases or tests, and it's not as clean. One thing that we've been digging into over the last few weeks is that cases are going way up, hospitalizations are going way up, but deaths have continued to drift downwards. If you look at Arizona, Florida and Texas, which have been kind of the leading edge of the Sunbelt surge, what you see is that deaths are clearly rising in Arizona, Florida and Texas since about the first week of June. And then if you look at the other states, they've been falling. What you have in the death data is the same thing that we actually saw in the case data for a long time during that false plateau. We had falling cases in the Northeast and in places that weren't having major outbreaks. And then we had rising cases which were sort of drowned out by what was happening in the Northeast. And what we saw with cases is eventually the Northeast bottoms out. When the Northeast bottoms out and these other states have continued to rise, you do see the numbers then start to trend upwards. We saw that happen first with cases and we saw it with hospitalizations. And, sadly, there's kind of only one thing to really expect with the death data. Hamblin: I'm wondering if these national averages are useful or should we be talking less about national numbers and more about just the local picture? Madrigal: The national numbers do matter for things like the supply chains. That said, this is an infectious disease. The big question for New Yorkers and everybody else in the Northeast and the Midwest is: Do we really think that this will be contained to the South and West if it continues going like this? Wells: Is there any stopping this? Madrigal: Well, what needs to happen hasn't changed for months. I think we need to get people to be taking a lot of precautions and reducing the risk of getting infected and spreading infection. But I also think we need people to live sustainably— where they might imagine being able to live like this for a year because we have no path to suppression right now. from https://ift.tt/3j5Uiu2 Check out http://natthash.tumblr.com Everything is canceled. Unemployment is at Great Depression levels. Over 130,000 Americans are dead. So why is the stock market doing so well? Staff writer Derek Thompson joins James Hamblin and Katherine Wells on the podcast Social Distance to explain why Wall Street seems divorced from reality. Listen here: Subscribe to Social Distance on Apple Podcasts, Spotify, or another podcast platform to receive new episodes as soon as they’re published. What follows is an edited and condensed transcript of their conversation. Katherine Wells: I'm going to read you this headline from last week: “U.S. stocks cap best quarter in two decades.” I feel like there's something missing here. Derek Thompson: Yeah, the stock market is super confusing right now. One way to think about this is that the stock market is not a reflection of the economy today. It is an indicator of what investors think will happen in the next five to 10 years. The easiest way to explain the gap in optimism that's opened up between basically everything that isn't the stock market and the stock market is the fact that a lot of investors looking at the sharp recovery that a couple economic statistics have made since the bottom hit in mid-March has made them optimistic about the fact that we might not recover 100 percent from this pandemic and this economic crisis in the next six or nine months, but they're seeing things that make us think that in the next year or two years, things are basically going to be where they were in January and February 2020. Let's think about three different categories: housing, cars, and big internet stocks. Houses and cars are really important to think about because they're the most expensive purchases that people tend to make. And then internet stocks are important because they have been driving stock-market growth for the last few years. All of those look like they could pretty much recover or are already basically at higher levels than they were in January and February. First, the housing market is doing bizarrely fine. New home sales are higher than they were a year ago. Mortgage applications are higher than they were in late February. Home-construction projects based on some online marketplaces are higher than they were in January and February. In previous recessions—certainly the Great Recession—housing was just destroyed. And in this recession, housing is actually doing totally fine. Then, you look at something like cars. Right after houses, cars are the most expensive thing that people tend to buy in their life. And there's every reason to think that the car economy is going to be pretty much fine as well. You have a lot of Americans that look like they're going to move to the suburbs because people are going to be a little bit freaked out to live in crowded areas. And what do you need in the suburbs? Well, you need cars. There's every possibility that you could have an auto recovery that is pretty much fine after the next year. And then finally, you have internet stocks and they're doing sensationally. I mean, the plague economy has basically shut down face-to-face interactions for large parts of the population, which means that if you do anything, you have to go online. Microsoft, Apple, Amazon, Google, Facebook, Cisco, Adobe—practically all of them have seen gains this year and the gains of those large tech companies have essentially driven the stock market recovery. James Hamblin: Do you know what percentage of Americans have money in the stock market, apart from 401(k)? Thompson: I don't know apart from a 401(k)—because I do think for a lot of people, that's the most important way that they're invested—but stock market wealth is highly unequally held. Something like 90 percent of stock market wealth is held by, I think, the top 8 or 9 percent of Americans. Hamblin: I think I maybe understand a little bit more: Some companies are doing well enough that overall the average of the stock market doesn't look that bad. In fact, it looks really good because it's recovering from that big crash in March. But certainly some things have taken big hits and overall, money maybe just moved to sectors that are more in line with what's needed in pandemic life. Thompson: I think that's a great summary. Hamblin: In the past, or in an alternate universe where more people held stocks, and they were suddenly feeling widespread economic insecurity, they might sell their stocks. They might feel they need money now, so they cash out of the stock market. And then the stock market could crash because people needed liquid money right now because they just lost their job. But when you have so much of the stock market controlled by super wealthy people who are going to groan and be upset when the stock market goes down, but don't really need that money to live, they're just going to kind of hang in there and move it around. And that creates a sort of stability for the stock market that might not have been there in the past. Thompson: I think it's a pretty good summary. Because the stock market tends to be determined by higher income people's wealth, it is essentially a reflection of what higher income Americans think about the future of corporate America. And the fact that the stock market's doing pretty well right now tells you that a lot of higher income Americans and the institutions and funds that they represent are optimistic about the fact that, even though the economy right now looks really shitty, there's a lot of big publicly traded companies about which they're really optimistic. Most of these companies are tech companies: Microsoft, Apple, Amazon, Google. They're really optimistic about these companies getting bigger and bigger. And as a result, rich people's optimism about big companies seems to us like everybody's optimism about the entire economy. But those are two different things. I think that rather than see the stock market as some plutocratic grade of the entire economy, you should see it as just one part of a very complex system that is the economy. When you see that restaurant sales are up, that says something important about restaurant sales. When you see that hotel bookings are down, that's something really important about hotels. When you see that the stock market is up and you see that it's up mostly because investments into large tech companies are soaring, that says something really important. It tells you that lots of institutions and rich investors see the digital economy basically shooting forward ten years to 2030 in terms of its power and its revenue and, correspondingly its profit. So rather than say, oh, this is anomalous, it's divergent, we should ignore it, I think we should pay close attention to it. It's telling us something important about the economy, even if that important thing doesn't feel nice to think about. from https://ift.tt/3fqintD Check out http://natthash.tumblr.com |
Authorhttp://natthash.tumblr.com Archives
April 2023
Categories |
 RSS Feed
RSS Feed
