|
As a young boy, Denis Vandervelde realized he faced two major obstacles to achieving distinction in the study of stamps, called philately: he was penniless, and, worse, color-blind. “A lot of the expertise in stamp collecting depends on shades and tiny variations in printings,” he told us. “So it was a daft hobby for me to have.” Instead, Vandervelde began collecting postmarks and quickly found himself absorbed in an entirely different pursuit—a kind of postal treasure hunt, documenting the elaborate bureaucracy that has emerged to manage the movement of mail around the world. His collection, assembled over nearly 50 years, boasts 3,000 items of disinfected mail: letters that have been punctured, perfumed, or otherwise purified to prevent the transmission of disease. During the coronavirus pandemic, the practice reemerged: Authorities around the world marked letters as delayed in quarantine, envelopes were stamped with fumigation notices, and parcels from suspect countries were returned to sender. By studying the traces left by disinfection—scorch marks, stains, and incisions—and the distinctive cancellations used to mark mail as treated, Vandervelde and his colleagues in the Disinfected Mail Study Circle, an international group of hobbyists and collectors, have ended up performing a forensic archaeology of quarantine through its postal paper trail. Official medical records from before the 18th century are sparse; disinfected mail inadvertently provides a time-stamped, geotagged archive of past epidemics, while its treatment establishes documentary evidence of both permanent and pop-up systems of infection control. 
We met in Islington, London, at Stampex, a biannual philatelic fair that is Europe’s largest. Vandervelde, a sprightly octogenarian, suggested that we join him after a morning’s booth-browsing as he refueled with a glass of Shiraz and a pizza at the convention center café. Over lunch, he explained that the practice of disinfecting mail was first formalized in the Adriatic, though no one knows exactly when. Certainly by the 1490s, following a century during which Venice had been scourged by a fresh outbreak of plague every decade, that city’s health authorities had decided that it might be wise to extend their sanitary precautions to letters that came from infected areas. As with many of the other practices of quarantine, including the institution of quarantine stations, known as lazarettos, other port cities were quick to follow in Venice’s footsteps. “You have to remember that the general belief at the time was that all infectious diseases were a miasma—a kind of a cloud that could attach itself to things,” explained Vandervelde. “Therefore anything could be subject to infection.” Not everything was considered equally conducive to conveying miasma, however: Soft materials, such as cloth, wool, and even fruits and vegetables, were thought to be highly susceptible, whereas hard objects, such as wood, metal, and tortoiseshell, were seen as impervious to infection. Paper sat in between these two extremes—it was seen as theoretically susceptible, but not especially likely to carry disease. “In the early days, the mail was simply put into a wooden coffin with sweet-smelling herbs and spices,” he said. “It had to be in there for at least a week, and, if it wasn’t collected in six weeks, it would be destroyed.” Later on, health commissioners in the Mediterranean adopted a process they called the spurgo, or “purge”—“a much more violent treatment with vinegar and smoke.” In all cases, the logic was that these strong odors were capable of displacing any disease-ridden bad air that might have impregnated the paper en route. Letters were sprinkled with or dipped in vinegar, which left distinctive splash marks; they were then put on a wire grate and grilled, or held over a fire with tongs, whose ghostly impressions remain visible as white lines on a browned envelope. Health officials in some locations were known for their particularly enthusiastic disinfection; correspondence that passed through Marseille frequently emerged unreadable. [Read: A revolution is sweeping the science of ancient diseases] Brittle, stained, discolored, and typically adorned with an official cachet or wax seal, the letters reassured recipients of their mail’s safety—on the outside, at least. Indeed, many Italian health authorities drew attention to the limitations of their disinfection, with a stamp that read netta fuori e sporca dentro, or “Clean Outside and Dirty Inside.” “You may well ask what on earth you were supposed to do when you received a letter like that!” Vandervelde said with a laugh. “Open it?” He told the story of a much later outbreak, when a circus entertainer from India brought smallpox to Launceston, Tasmania, in 1904. In response, the Australian postal service disinfected the city’s mail for three months, marking thousands of letters as treated. “Ninety-nine percent of recipients put those letters straight in the fire,” said Vandervelde. 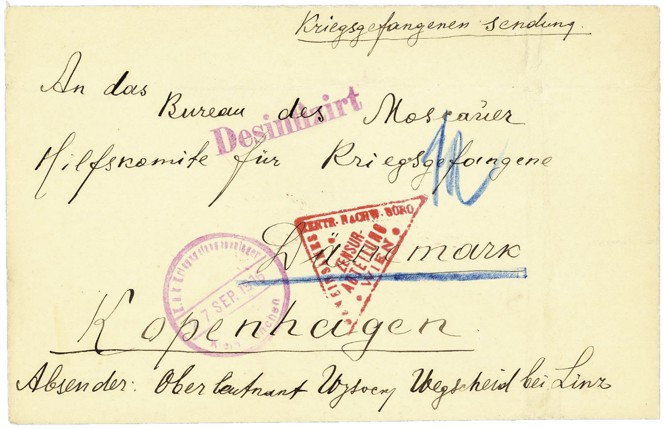
Later, when we returned to his house to spend an afternoon marveling at the highlights of his collection, Vandervelde showed us one of the earliest known examples of internal disinfection. “It’s from Naples, where they were very fierce,” he said. “As far as I know, they were the first to slit.” The letter had been slit open at each corner with a chisel to allow the fumigant inside. This practice of slashing mail with chisels and awls, which left many letters in shreds, was later made obsolete by a device called a “rastel” (from the Latin rastellus, or “rake”), which resembles the love child of a waffle iron and a medieval torture device. Letters were placed between hinged, spiked plates, and punctured pre-fumigation—the particular pattern of holes punched through the paper, such as the offset grid used in Hamburg, Germany, or the distinctive sunburst of Mahón, Minorca, can provide disinfected-mail collectors with yet another clue as to the date or location of a letter’s treatment. The study of disinfected mail began in the 1950s. In San Francisco, a scientist named Karl F. Meyer came across an 1898 letter stamped MIT FORMALIN DESINFICIERT (“Disinfected With Formalin”). He was sufficiently intrigued to start a collection, and, in 1962, published Disinfected Mail, still the only comprehensive book on the subject. When a young Vandervelde acquired his first disinfected letters, it was thus Meyer’s book to which he turned. The next time Meyer was in London, the two of them had dinner. They became fast friends, though Meyer died just before Vandervelde founded the Disinfected Mail Study Circle in 1973. “I’ve got a letter from him saying you’ll be lucky if you get more than six members,” said Vandervelde. “We’re now 150 strong, in 25 countries, and still growing.” He estimates that at least a third of DMSC members are medical historians or doctors, a third are collectors, and another third are stamp dealers or authors who write about related subjects. (We joined the circle in 2009.) Until recently, the benefits of membership included a subscription to Pratique, the society’s newsletter. Each issue, although occasionally many months delayed because of technical difficulties involving Vandervelde’s antiquated AOL account, is filled with stories and scenes that convey the flawed reality of quarantine. At times, his research has revealed outbreaks that had otherwise been lost to history: an 1897 outbreak of plague in India that triggered disinfection measures in southern Russia and, for one day only, in New York City. (There, a paranoid postmaster decided, seemingly on his own initiative, to fumigate a bag of mail from India that had arrived on the steamship Britannic.) If the letters themselves are pieces in a puzzle, Vandervelde and his colleagues are obsessive in their desire to fill in the gaps, collecting maps and tracking down contemporary sanitary proclamations that shed light on the slightest variation in quarantine practices. In painstaking detail, for missive after missive, Vandervelde has traced how, where, and why quarantine operated in the premodern world—a largely forgotten geography of lazarettos, rastel stations, merchant ships, colonial checkpoints, health passports, and border crossings. [Read: 98 years of mail fraud] Bureaucratic processes are how a jurisdiction establishes itself: The issuing of coinage and postage stamps tends to be the first order of business for a new state. Similarly, the otherwise imaginary and invisible line around a country—its border—is typically articulated through quarantine and other health-screening practices: Disease management, by attempting to keep microbes out, defines the edges of in. Thus, when the southern provinces of the Netherlands seceded, in 1830, to form their own country, Belgium, they issued their own coins and stamps in the subsequent decades. They also introduced quarantine controls, including the disinfection of mail. “Wanting to be quite different from both the Dutch and the French, they decided that the way they would deal with mail was to open up each letter, smoke it, and then reseal it by sticking a label with an apology in French,” Vandervelde said. This label—a 3-by-2-inch rectangle of heavy cartridge paper, in a distinctive shade of gray—is Vandervelde’s white whale. Because the label was typically stuck over the fold, it was almost always ripped in half to get at the letter inside. “Consequently, there are only, as far as I know, three examples in the world of this thing complete, and two of them are almost certainly printers’ samples,” he said. [Read: What was the most important letter in history?] In addition to its rarity, one of the things that makes this Belgian disinfection label particularly significant is that 1830 also marks the first outbreak of cholera in Europe. The disease seems to have been endemic in the Ganges Delta region for centuries, but just four years earlier most Europeans had likely never heard of it. By 1831, cholera had reached Finland, Poland, and Austria. From there it spread to the Baltic ports, arriving in Sunderland, England, by December 1831, in New York City and Philadelphia a year later, and in Mexico and Cuba soon after that. In Russia alone, more than a quarter of a million people died of cholera. Over the next 60 years, four more deadly cholera pandemics would sweep across Europe and the world, killing more people more quickly than any other epidemic disease of the 19th century. Meanwhile, European and American attempts to prevent its spread ended up defining the systems of global governance that still shape the world today. Alison Bashford, an Australian historian, explained to us that Europe’s fear of cholera became focused, in particular, on a suspected super-spreading event—the hajj. Since medieval times, hundreds of thousands of Muslims from the Middle East and Asia had undertaken this sacred pilgrimage to Mecca every year, but their journeys—by camel caravan and by sail—took so long that any disease they might have been carrying would have revealed itself, and then burned out, en route. By the mid-1800s, the accelerated pace of travel by railway and steamship risked seeding new outbreaks on Europe’s borders. In response, Western authorities attempted to control the spread of cholera—and the movement of Muslims—by setting up quarantine camps. One of these camps was located at El Tor, a tiny port at the tip of the Sinai Peninsula, where the Suez Canal opens onto the Red Sea. It was run by Egyptians under the direction of the European powers who had organized themselves into a sanitary and quarantine board with broad authority to ensure that ships arrived in Alexandria, on the Mediterranean end of the Suez Canal, free from disease. According to Vandervelde, who has a postcard mailed from this camp in his collection, conditions at El Tor “were primitive in the extreme.” He showed us illustrations from The Graphic magazine that depicted a handful of wooden sheds built on the beach to house passengers, the distinctly spartan interior of the “Ladies’ Quarantine Shed,” and the even more austere “Cholera Tent,” for those who fell sick. Of course, every time anyone did show symptoms, the quarantine’s duration was extended, meaning that pilgrims could easily spend months waiting on the beach, subjected to intense daytime heat and freezing cold nights, as well as a persistent north wind that blew sand into every crevice. (Conjunctivitis and other eye conditions were common.) Two cisterns were available for five hours a day, to serve 300 or more people, leading one pilgrim to report “nights spent tormented by thirst.” In addition to being considered disease vectors by European authorities, the pilgrims were Muslim and thus perceived as threatening to colonial rule. Through quarantine, the edges of Europe were made visible—and could be medically enforced. As the 19th century unfolded, quarantine began to fall out of favor. Critics claimed that it was arbitrary and, for the most part, useless, even while it also exacted an enormous economic cost in terms of lost time and trade. Britain, which once conducted so little trade with the East that it hadn’t bothered to build a national quarantine station, now relied on the free flow of goods and people to maintain its global empire. At the same time, other countries did not share that view—or that economic model—and would happily subject British ships to retaliatory quarantine if they felt its sanitary precautions were not adequate. In the 1850s and ’60s, British authorities devised a combination of measures, in lieu of quarantine, that came to be known as “the English preventive system.” This multifaceted approach involved epidemiological intelligence efforts, including tracking outbreaks overseas and monitoring the health of newly arrived travelers, along with investments in public sanitation. The system was designed to catch and isolate the sick, rather than simply detain everyone at the border for mandatory observation. It worked: No major cholera outbreaks occurred in England after 1866. This neo-quarantine, pioneered by the British and eventually adopted by the rest of the world as the basis of global health, still operated by controlling mobility (of people and thus their germs). It simply replaced the physical barrier of lazarettos and cordons sanitaires with a selective, surveillance-based one—which relied on data rather than buildings. This shift, from fixing people in space with architecture to tracking their movements and contacts, required the development of novel techniques and bureaucracies with which to define and verify individual identities. Today, we know these techniques and bureaucracies as the “passport” and “passport control,” but the earliest such documents were health passports. From the 1500s, local authorities would issue these formal printed documents, known in Italian as fedi di sanitá, to travelers hoping to avoid quarantine at their destination. As “a bit of a breather” between showing us his collections of quarantine letters and disinfected mail, Vandervelde allowed us to inspect some of the earliest health passports in his collection. “The reason I’ve selected these is that, until about 1700, paper was very expensive, and therefore they use very small sheets,” he said. “As time went on and paper became cheaper, the passports got bigger and bigger and bigger and ended up enormous—so these obviously are easier to show.” Like quarantine, after the 1950s, “disinfected mail more or less disappears,” Vandervelde told us. The most modern item in his collection dates to 1972, when, just as the World Health Organization was preparing to declare smallpox eradicated, a Yugoslav guest worker in Hanover, Germany, was taken to the hospital and quickly isolated, suffering with what local doctors described as “a fulminating pox.” He had been in Germany for only two weeks, but smallpox is highly contagious: Tracking down all his contacts was essential, as many of them might also be infected. There was just one problem. “He was a very handsome young man,” said Vandervelde, “and when they put his picture in the local newspaper and asked for anybody who’d seen this man to come forward, 283 girls claimed to have met him.” The authorities dutifully rounded up all 283 young women, housing them in village halls and Scout huts for a period of quarantine. Smallpox, as it happens, is one of the very few pathogens whose transmission through the mail has actually occurred—Vandervelde told us that, during the American Civil War, there were six authenticated cases of wives or girlfriends who, on receipt of a letter from their smallpox-stricken beau at the front, “kissed it or put it into her bosom and later went down with smallpox.” With their old rastels and tongs consigned to the museum, German authorities decided to disinfect any letters sent from quarantine by the girls to their friends and families by wrapping the envelopes in muslin and ironing them three times at the highest setting. Even more recently, following the 2001 anthrax attacks, the U.S. Postal Service determined that letters and parcels sent to zip codes beginning in 202, 203, 204, and 205, which serve federal-government agencies in Washington, D.C., should be treated. A company that irradiated food to extend its shelf life won the contract, and, although USPS has declined to comment, the agency’s website says that mail destined for those zip codes is still forwarded to New Jersey, where it is put on a conveyor belt and passed under a high-energy beam of ionizing radiation to kill bacteria and viruses. The letters and packages are then “aired out” for a while, before being forwarded to their destinations. The paper is left slightly faded and somewhat crispy, but sterile—and, at least sometimes, stamped as such. “Those cachets typically go for about $25,” Vandervelde said. “I think even that’s overpriced for something that recent.” In the early days of the coronavirus pandemic, as public-health authorities resorted to the medieval technology of quarantine, they also wondered whether they ought to resurrect mail disinfection. Early studies indicated that the virus could survive for 24 hours on cardboard surfaces, perhaps longer on paper, although we now know that most infections are transmitted by aerosols. Nevertheless, in February 2020, China’s central bank began quarantining the country’s cash, collecting banknotes from Hubei, the worst-hit province, then baking them at a high temperature or bathing them in ultraviolet rays. The newly laundered cash was then kept in isolation for seven to 14 days before being rereleased. A few weeks later, the U.S. Federal Reserve began quarantining dollar bills repatriated from Asia, holding them for seven to 10 days before allowing them to reenter the domestic financial system. As the pandemic dragged on, pushback began against the introduction of health-based QR codes as a means of restricting individual movement, as well as the promise, or threat, of international vaccine passports. Such anxieties do, in fact, have historical justification: As our tour of disinfected mail with Denis Vandervelde had shown, the temporary infrastructure and controls on mobility put in place during an outbreak can harden into permanent borders, bureaucracy, and, too often, inequities. The world around us is structured by the ghosts of quarantines past. This post was excerpted from Until Proven Safe: The History and Future of Quarantine. from https://ift.tt/3Bpg8BZ Check out http://natthash.tumblr.com
0 Comments
The summer wasn’t meant to be like this. By April, Greene County, in southwestern Missouri, seemed to be past the worst of the pandemic. Intensive-care units that once overflowed had emptied. Vaccinations were rising. Health-care workers who had been fighting the coronavirus for months felt relieved—perhaps even hopeful. Then, in late May, cases started ticking up again. By July, the surge was so pronounced that “it took the wind out of everyone,” Erik Frederick, the chief administrative officer of Mercy Hospital Springfield, told me. “How did we end up back here again?” The hospital is now busier than at any previous point during the pandemic. In just five weeks, it took in as many COVID-19 patients as it did over five months last year. Ten minutes away, another big hospital, Cox Medical Center South, has been inundated just as quickly. “We only get beds available when someone dies, which happens several times a day,” Terrence Coulter, the critical-care medical director at CoxHealth, told me. Last week, Katie Towns, the acting director of the Springfield–Greene County Health Department, was concerned that the county’s daily cases were topping 250. On Wednesday, the daily count hit 405. This dramatic surge is the work of the super-contagious Delta variant, which now accounts for 95 percent of Greene County’s new cases, according to Towns. It is spreading easily because people have ditched their masks, crowded into indoor spaces, resumed travel, and resisted vaccinations. Just 40 percent of people in Greene County are fully vaccinated. In some nearby counties, less than 20 percent of people are. [Read: The three simple rules that underscore the danger of Delta] Many experts have argued that, even with Delta, the United States is unlikely to revisit the horrors of last winter. Even now, the country’s hospitalizations are one-seventh as high as they were in mid-January. But national optimism glosses over local reality. For many communities, this year will be worse than last. Springfield’s health-care workers and public-health specialists are experiencing the same ordeals they thought they had left behind. “But it feels worse this time because we’ve seen it before,” Amelia Montgomery, a nurse at CoxHealth, told me. “Walking back into the COVID ICU was demoralizing.” Those ICUs are also filling with younger patients, in their 20s, 30s, and 40s, including many with no underlying health problems. In part, that’s because elderly people have been more likely to get vaccinated, leaving Delta with a younger pool of vulnerable hosts. While experts are still uncertain if Delta is deadlier than the original coronavirus, every physician and nurse in Missouri whom I spoke with told me that the 30- and 40-something COVID-19 patients they’re now seeing are much sicker than those they saw last year. “That age group did get COVID before, but they didn’t usually end up in the ICU like they are now,” Jonathan Brown, a respiratory therapist at Mercy, told me. Nurses are watching families navigate end-of-life decisions for young people who have no advance directives or other legal documents in place. Almost every COVID-19 patient in Springfield’s hospitals is unvaccinated, and the dozen or so exceptions are all either elderly or immunocompromised people. The vaccines are working as intended, but the number of people who have refused to get their shots is crushing morale. Vaccines were meant to be the end of the pandemic. If people don’t get them, the actual end will look more like Springfield’s present: a succession of COVID-19 waves that will break unevenly across the country until everyone has either been vaccinated or infected. “You hear post-pandemic a lot,” Frederick said. “We’re clearly not post-pandemic. New York threw a ticker-tape parade for its health-care heroes, and ours are knee-deep in COVID.” [Read: The end of the pandemic is now in sight] That they are in this position despite the wide availability of vaccines turns difficult days into unbearable ones. As bad as the winter surge was, Springfield’s health-care workers shared a common purpose of serving their community, Steve Edwards, the president and CEO of CoxHealth, told me. But now they’re “putting themselves in harm’s way for people who’ve chosen not to protect themselves,” he said. While there were always ways of preventing COVID-19 infections, Missourians could have almost entirely prevented this surge through vaccination—but didn’t. “My sense of hope is dwindling,” Tracy Hill, a nurse at Mercy, told me. “I’m losing a little bit of faith in mankind. But you can’t just not go to work.” When Springfield’s hospitals saw the first pandemic wave hitting the coasts, they could steel themselves. This time, with Delta thrashing Missouri fast and first, they haven’t had time to summon sufficient reinforcements. Between them, Mercy and Cox South have recruited about 300 traveling nurses, respiratory therapists, and other specialists, which is still less than they need. The hospitals’ health-care workers have adequate PPE and most are vaccinated. But in the ICUs and in COVID-19 wards, respiratory therapists still must constantly adjust ventilators, entire teams must regularly flip patients onto their belly and back again, and nurses spend long shifts drenched in sweat as they repeatedly don and doff protective gear. In previous phases of the pandemic, both hospitals took in patients from other counties and states. “Now we’re blasting outward,” Coulter said. “We’re already saturating the surrounding hospitals.” Meanwhile, the hospitals’ own staff members are exhausted beyond telling. After the winter surge, they spent months catching up on record numbers of postponed surgeries and other procedures. Now they’re facing their sharpest COVID-19 surge yet on top of those backlogged patients, many of whom are sicker than usual because their health care had to be deferred. Even with hundreds of new patients with lung cancer, asthma, and other respiratory diseases waiting for care in outpatient settings, Coulter still has to cancel his clinics because “I have to be in the hospital all the time,” he said. [Read: What it really means to cancel elective surgery] Many health-care workers have had enough. Some who took on extra shifts during past surges can’t bring themselves to do so again. Some have moved to less stressful positions that don’t involve treating COVID-19. Others are holding the line, but only just. “You can’t pour from an empty cup, but with every shift it feels like my co-workers and I are empty,” Montgomery said. “We are still trying to fill each other up and keep going.” The grueling slog is harder now because it feels so needless, and because many patients don’t realize their mistake until it’s too late. On Tuesday, Hill spoke with an elderly man who had just been admitted and was very sick. “He said, ‘I’m embarrassed that I’m here,’” she told me. “He wanted to talk about the vaccine, and in the back of my mind I’m thinking, You have a very high likelihood of not leaving the hospital.” Other patients remain defiant. “We had someone spit in a nurse’s eye because she told him he had COVID and he didn’t believe her,” Edwards said. Some health-care workers are starting to resent their patients—an emotion that feels taboo. “You’re just angry,” Coulter said, “and you feel guilty for getting angry, because they’re sick and dying.” Others are indignant on behalf of loved ones who don’t already have access to the vaccines. “I’m a mom of a 1-year-old and a 4-year-old, and the daughter of family members in Zimbabwe and South Africa who can’t get vaccinated yet,” says Matifadza Hlatshwayo Davis, who works at a Veterans Affairs hospital in St. Louis. “I’m frustrated, angry, and sad.” [Read: ‘No one is listening to us’] “I don’t think people get that once you become sick enough to be hospitalized with COVID, the medications and treatments that we have are, quite frankly, not very good,” says Howard Jarvis, the medical director of Cox South’s emergency department. Drugs such as dexamethasone offer only incremental benefits. Monoclonal antibodies are effective only during the disease’s earliest stages. Doctors can give every recommended medication, and patients still have a high chance of dying. The goal should be to stop people from getting sick in the first place. 
But Missouri Governor Mike Parson never issued a statewide mask mandate, and the state’s biggest cities—Kansas City, St. Louis, Springfield, and Columbia—ended their local orders in May, after the CDC said that vaccinated people no longer needed to wear masks indoors. In June, Parson signed a law that limits local governments’ ability to enact public-health restrictions. And even before the pandemic, Missouri ranked 41st out of all the states in terms of public-health funding. “We started in a hole and we’re trying to catch up,” Towns, the director of the Springfield–Greene County Health Department, told me. Her team flattened last year’s curve through testing, contact tracing, and quarantining, but “Delta has just decimated our ability to respond,” Kendra Findley, the department’s administrator for community health and epidemiology, told me. The variant is spreading too quickly for the department to keep up with every new case, and more people are refusing to cooperate with contact tracers than at this time last year. The CDC has sent a “surge team” to help, but it’s just two people: an epidemiologist, who is helping analyze data on Delta’s spread, and a communications person. And like Springfield’s hospitals, the health department was already overwhelmed with work that had been put off for a year. “Suddenly, I feel like there aren’t enough hours in the day,” Findley said. Early last year, Findley stuck a note on her whiteboard with the number of people who died in the 1918 flu pandemic: 50 million worldwide and 675,000 in the U.S. “It was for perspective: We will not get here. You can manage this,” she told me. “I looked at it the other day and I think we’re going to get there. And I feel like a large segment of the population doesn’t care.” The 1918 flu pandemic took Missouri by surprise too, says Carolyn Orbann, an anthropologist at the University of Missouri who studies that disaster. While much of the world felt the brunt of the pandemic in October 1918, Missouri had irregular waves with a bigger peak in February 1920. So when COVID-19 hit, Orbann predicted that the state might have a similarly drawn-out experience. Missouri has a widely dispersed population, divided starkly between urban and rural places, and few highways—a recipe for distinct and geographically disparate microcultures. That perhaps explains why new pathogens move erratically through the state, creating unpredictable surges and, in some pockets, a false sense of security. Last year, “many communities may have gone through their lockdown period without registering a single case and wondered, What did we do that for?” Orbann told me. She also suspects that Missourians in 1918 might have had a “better overhead view of the course of the pandemic in their communities than the average citizen has now.” Back then, the state’s local papers published lists of people who were sick, so even those who didn’t know anyone with the flu could see that folks around them were dying. “It made the pandemic seem more local,” Orbann said. “Now, with fewer hometown newspapers and restrictions on sharing patient information, that kind of knowledge is restricted to people working in health care.” Montgomery, the CoxHealth nurse, feels that disparity whenever she leaves the hospital. “I work in the ICU, where it’s like a war zone, and I go out in public and everything’s normal,” she said. “You see death and suffering, and then you walk into the grocery store and get resistance. It feels like we’re being ostracized by our community.” If anything, people in the state have become more entrenched in their beliefs and disbeliefs than they were last year, Davis, the St. Louis–based doctor, told me. They might believe that COVID-19 has been overblown, that young people won’t be harmed, or that the vaccines were developed too quickly to be safe. But above all else, “what I predominantly get is, ‘I don’t want to talk to you about that; let’s move on,’” Davis said. [Derek Thompson: Millions are saying no to vaccines: What are they thinking?] People take the pandemic seriously when they can see it around them. During past surges in other parts of the U.S., curves flattened once people saw their loved ones falling ill, or once their community became the unwanted focus of national media coverage. The same feedback loop might be starting to occur in Missouri. The major Route 66 Festival has been canceled. More people are making vaccine appointments at both Cox South and Mercy. In Springfield, the public-health professionals I talked with felt that they had made successful efforts to address barriers to vaccine access, and that vaccine hesitancy was the driving force of low vaccination rates. Improving those rates is now a matter of engendering trust as quickly as possible. Springfield’s firefighters are highly trusted, so the city set up vaccine clinics in local fire stations. Community-health advocates are going door-to-door to talk with their neighbors about vaccines. The Springfield News-Leader is set to publish a full page of photos of well-known Springfieldians who are advocating for vaccination. Several local pastors have agreed to preach about vaccines from their pulpits and set up vaccination events in their churches. One such event, held at James River Church on Monday, vaccinated 156 people. “Once we got down to the group of hesitant people, we’d be happy if we had 20 people show up to a clinic,” says Cora Scott, Springfield’s director of public information and civic engagement. “To have 156 people show up in one church in one day is phenomenal.” But building trust is slow, and Delta is moving fast. Even if the still-unvaccinated 55 percent of Missourians all got their first shots tomorrow, it would still take a month to administer the second ones, and two weeks more for full immunity to develop. As current trends show, Delta can do a lot in six weeks. Still, “if we can get our vaccination levels to where some of the East Coast states have got to, I’ll feel a lot better going into the fall,” Frederick, Mercy’s chief administrative officer, said. “If we plateau again, my fear is that we will see the twindemic of flu and COVID.” In the meantime, southwest Missouri is now a cautionary tale of what Delta can do to a largely unvaccinated community that has lowered its guard. None of Missouri’s 114 counties has vaccinated more than 50 percent of its population, and 75 haven’t yet managed more than 30 percent. Many such communities exist around the U.S. “There’s very few secrets about this disease, because the answer is always somewhere else,” Edwards said. “I think we’re a harbinger of what other states can expect.” from https://ift.tt/2URGqvY Check out http://natthash.tumblr.com The byzantine world of pharmaceutical regulation has recently broken into the public consciousness, causing a bit of a panic. Aducanumab—the first new Alzheimer’s treatment in nearly two decades—was approved by the Food and Drug Administration on June 7 despite scant evidence of benefit, and against the nearly unanimous advice of the agency’s expert advisers. Op-eds called the decision, which could trigger billions of dollars in new government spending, a “false hope,” “bad medicine,” and “a new low.” (FDA officials have said that their decision was based on “rigorous science,” and that it reflects the willingness of people with Alzheimer’s and their families’ to accept a treatment that might help, despite “some degree of uncertainty.”) On Thursday, the FDA tried to clarify that the drug should be used only for patients with mild dementia; the next day, amid concerns about inappropriate interactions between the drugmaker and FDA officials, Acting Commissioner Janet Woodcock called for her own agency to be investigated. This isn’t the first—or fifth—run of bad press the agency has received, but one gets the sense from recent coverage that some crucial threshold has now been crossed, that the rising floodwaters of ineptitude have finally yielded a catastrophe. But even if this blunder’s inner workings are more public than those of the past, there’s little reason to believe we’ll see systemic change at the FDA. The long-standing and gradual erosion of the agency’s scientific standards makes me think instead of the eroding coastlines and thawing icebergs associated with climate change. For decades now, alarmed scientists have been crying out for action as things have gotten worse and worse. And for decades now, little has been done. The FDA’s standards began to slide in the late 1980s and early ’90s. AIDS activists, desperate to slow a devastating and mysterious illness, had pushed for the creation of new pathways for approving treatments more quickly—and, effectively, on thinner evidence. A new program in 1992 allowed for “accelerated approval” on the basis of surrogate markers, which are indirect measures of a drug’s benefit, assessed via laboratory or imaging tests, that stand in for more meaningful outcomes such as life expectancy. But the implementation of these accelerated processes was criticized by some scientists and patients, even at the time. In 1994, for example, The New York Times cited skeptics who worried that “no one can tell if the drugs work.” Eight months later, the AIDS activist organization ACT UP San Francisco called Anthony Fauci a “pill-pushing pimp” for supporting CD4 immune-cell counts and viral loads as surrogate markers. They were completely invalid, the activists wrote, and nothing more than “a marketing exec’s wet dream.” [Read: Before Occupy: How AIDS activists seized control of the FDA in 1988] That early change in standards worked out for the best. We now know that CD4 counts and viral load are excellent markers of HIV/AIDS status, and the types of HIV drugs that were being questioned at the time—reverse-transcriptase inhibitors and protease inhibitors—did turn out to be effective. Newer versions still form the backbone of lifesaving, multidrug regimens. In fact, their success has been used to wave off criticism of the FDA’s declining standards for years. But that level of success is not at all the norm. Most treatments in medicine will prove only modestly effective and come with real risks. The use of regulatory shortcuts has grown more common anyway. In 1992, about 40 percent of all drugs qualified for at least one of the FDA’s expedited programs for approval. By 2018, that rate had doubled. Use of surrogate endpoints has now become routine—60 percent of approvals in recent years have relied on them. The repeated protests of agency critics along the way have done nothing to slow the trend. In May 2000, for example, the government approved the use of saline breast implants despite safety concerns. “This decision really sets the FDA standard of safety at a new low,” the health-policy expert Diana Zuckerman said at the time. More than 20 years later, she continues to decry the agency’s still-declining standards: The aducanumab approval “sets a very dangerous precedent that could harm patients’ health,” she said recently. (Acting Commissioner Woodcock has disputed the idea that evidence standards are declining; in her view, “we know far more now about a drug when it is approved than in the past.”) Indeed, public controversies over drug approvals have only proliferated. In 2015, the FDA approved flibanserin, a treatment meant to improve female libido, after having rejected it twice. “This is a product that is neither very effective nor particularly safe,” one former FDA official told reporters at the time, and it sets “a precedent that a drug for women’s sexual health has to be treated in a very special way.” The agency reached another low the following year, when its leaders overruled their own staff to approve eteplirsen, a treatment for a rare genetic condition called Duchenne muscular dystrophy. The drug’s poor quality of evidence led a dissenting official to declare that it was nothing more than a “scientifically elegant placebo.” The 21st Century Cures Act easily cleared Congress a few months after that, though two former ACT UP members and a former FDA commissioner had declared in a Times op-ed that the new law’s encouragement of even-lower low standards was “potentially placing patients at unnecessary risk of injury or death.” In 2019, the bioethicist Ezekiel Emanuel warned about the approval of a slew of new cancer therapies with uncertain or very limited benefits, noting that “drugs with unproven effectiveness sell false hope to desperate patients.” [Read: In between the FDA and Pharma, people wait for treatments] The FDA says that it must balance the importance of meeting rigorous standards with the need to provide timely access to potentially lifesaving medicines. “Commentators have noted FDA’s increasing use of these programs over the last decade, often with a view that the increase is driven by a loosening of our approval standards,” Woodcock and the FDA official Peter Marks wrote in 2019. “In reality, the FDA’s standards have not changed. Instead, the increased use of expedited approval pathways is directly related to the increasing numbers and scope of these programs provided by Congress, as well as the kinds of medicines that are being developed, and the types of diseases that are being studied.” For all the panicky commentary, the problem is a diffuse and slowly growing one, with specific harms that are tricky to assess. That’s why the approval of yet another costly, ineffective drug on the basis of a suspect surrogate marker ends up being like another deadly set of wildfires in the West: We’re told that it has to do with long-standing changes in the climate, but responding to the immediate crisis distracts from broader fixes. Even the agency’s “historic” and ill-advised sign-off on aducanumab might not move the needle of public opinion toward favoring greater scientific rigor over quicker access, according to Daniel Carpenter, a government professor at Harvard who has studied the FDA. It’s hard to feel invested in medical regulation without tangible, personal reminders of what happens when it fails. If aducanumab were to prove really dangerous for patients—if it ended up killing people—that would certainly grab attention. (There’s currently no evidence of major harm from aducanumab, though the FDA’s expert advisers did raise concerns about brain swelling in some clinical-trial patients.) The experience of children who were born with severe disabilities from thalidomide in the 1950s and ’60s, like that of the victims of sulfanilamide poisoning in the ’30s, prompted significant strengthening of government oversight. Thalidomide had that influence, Carpenter told me, “precisely because the nature of the deformities the victims had was so visceral, so evocative.” But the approval of a merely ineffective and expensive drug simply wouldn’t have the same effect. You need to see the health-care system’s version of a starving polar bear, he said, or else most people won’t care. Even aducanumab’s staggering price tag of $56,000 a patient per year may not be conspicuous enough, because few will pay the full cost themselves. Most of the expense incurred for each new drug—which, for aducanumab, could be larger than NASA’s yearly budget—ends up being quietly subsumed into strained public-health budgets and rising health-insurance premiums. The actions of drug regulators, like those of industrial polluters, are often freighted with unacknowledged externalities. “The FDA specifically does not really worry about those larger societal issues and doesn’t really worry about cost,” Walid Gellad, a drug-policy researcher at the University of Pittsburgh, told me. Instead, the agency is judged by how many drugs it can approve. No regulator “wants to go before Congress or the American people and say, ‘This year we approved 50 percent fewer drugs than last year,’” Gellad said. There are proposals for incentivizing the FDA to pursue cost-effective therapies, just as there are proposals for incentivizing reductions in carbon emissions. For example, health-policy researchers have suggested allowing the agency to shrink the window in which pharmaceutical companies can exclusively profit from their compounds, if those companies charge too much money for negligible benefits. Carpenter has recommended increasing the fees that companies pay to the FDA, and then having the agency use those resources to fund more-rigorous clinical studies. Medicare already has the authority to withhold payment for questionable treatments (and is now considering that option for aducanumab). But as with cap-and-trade policies for carbon emissions, aggressive approaches have failed in the face of powerful stakeholders. It’s not just the profit-driven pharmaceutical industry fighting these policies; patient groups are also effective advocates for quicker, easier access to new treatments. [Read: An age-old battle: the FDA versus the shill] In the absence of meaningful political progress or collective action, efforts to address the spread of bad or useless therapies—like efforts to address climate change—are left to individuals. The FDA may keep approving marginal treatments, but doctors don’t have to prescribe them. In theory, we could take a stand, and just say no to aducanumab. “There’s an assumption that physicians are good stewards and they’re going to take care of everybody and they’re not going to prescribe something that’s not effective,” Joseph Ross, a physician and health-policy expert at Yale, told me. “But you and I know how it really works in the real world.” Indeed, I do. For doctors, the allure of slowing the progression of a debilitating condition, satisfying patient requests, and even profiting from every prescription will make aducanumab hard to resist. Many of the passionate academic physicians I talk with seem willing to take up this fight in their own clinic, and recommend against the drug’s use, but they’re just idealists at the fringe, not the rank and file of the profession—91 percent of whom recently responded that they generally trust that the benefits of an FDA-approved therapy will outweigh its risks. This is the tragedy of the concerned citizen: We are personally destined to fail. Just as switching to an electric car or turning your lights off won’t cool a warming planet, a minority of idealistic doctors won’t stop the flood of ineffective treatments. But it’s not impossible that the aducanumab fiasco will yield some systemic change. Vinay Prasad, an oncologist and drug-policy expert at UC San Francisco, suspects that the total cost of this or some future drug could end up being high enough to cause a fiscal crisis, prompting action at long last. “The American economy can handle a great deal of wasteful health-care spending,” he told me. “But it can’t tolerate an infinite number.” The FDA might have finally acknowledged these financial considerations when it rapidly reversed course to recommend that only a subset of patients with early Alzheimer’s disease receive aducanumab. That change could save insurers billions of dollars, and it makes them more likely to place explicit limits on which patients will have their expenses covered. An interminable health-care-cost crisis will eventually spill over into other political issues, Prasad said. For example, the average worker experiences rising health-insurance premiums as stagnating wages. “It’s profoundly destabilizing in a society in ways we don’t see,” he told me. But whether politicians will do more than pursue empty hearings remains unclear. Before aducanumab, the exorbitant cost of new Hepatitis C treatments, initially as much as $1,000 a pill, generated similar hand-wringing but no real policy change. If an independent investigation leads to a reversal of the aducanumab decision, then perhaps such an unprecedented turn of events will prompt a real public reckoning. The most likely outcome, though, is that the bad headlines will recede and a new, lower bar for evidence will be set. With each alarming declaration of “the hottest day on record,” after all, it gets harder to remember what cooler temperatures felt like in the first place. from https://ift.tt/3B9oCxc Check out http://natthash.tumblr.com The first thing to know about the COVID-19 vaccines is that they’re doing exactly what they were designed and authorized to do. Since the shots first started their rollout late last year, rates of COVID-19 disease have taken an unprecedented plunge among the immunized. We are, as a nation, awash in a glut of spectacularly effective vaccines that can, across populations, geographies, and even SARS-CoV-2 variants, stamp out the most serious symptoms of disease. The second thing to know about the COVID-19 vaccines is that they’re flame retardants, not impenetrable firewalls, when it comes to the coronavirus. Some vaccinated people are still getting infected, and a small subset of these individuals is still getting sick--and this is completely expected. We’re really, really bad at communicating that second point, which is all about breakthroughs, a concept that has, not entirely accurately, become synonymous with vaccine failure. It’s a problem that goes far beyond semantics: Bungling the messaging around our shots’ astounding success has made it hard to convey the truly minimal risk that the vaccinated face, and the enormous gamble taken by those who eschew the jabs. The main problem is this. As the CDC defines it, the word breakthrough can refer to any presumed infection by SARS-CoV-2 (that is, any positive coronavirus test) if it’s detected more than two weeks after someone receives the final dose of a COVID-19 vaccine. But infections can come with or without symptoms, making the term imprecise. That means breakthroughs writ large aren’t the most relevant metric to use when we’re evaluating vaccines meant primarily to curb symptoms, serious illness, hospitalizations, and death. “Breakthrough disease is what the average person needs to be paying attention to,” Céline Gounder, an infectious-disease physician at Bellevue Hospital Center in New York, told me. Silent, asymptomatic breakthroughs—those that are effectively invisible in the absence of a virus-hunting diagnostic—are simply not in the same league. (The CDC did not respond to repeated requests for comment.) To put this in perspective, consider the original criteria laid out by the FDA about this time last year, back when the United States was still solidly in its second infectious surge. An effective inoculation, the agency said, should be able to “prevent disease or decrease its severity in at least 50 percent of people who are vaccinated.” It’s an easy benchmark to forget. By the close of 2020, two vaccines absolutely obliterated those expectations; two months later, a third followed, and now there’s buzz of a fourth. If disease is our yardstick, then breakthrough COVID-19 cases—a very small subset of all known breakthroughs—might meet our criteria for concern. These are actual illnesses, events where the shots’ protection has apparently crumbled; these cases are the same ones that vaccine makers searched so diligently for in clinical trials, to ensure that their products were working. By the same logic, asymptomatic coronavirus infections fall outside our shots’ protective purview as we defined it so many months ago. And although they’re important to track and glean data from, conflating them with the rest, experts told me, risks misrepresenting what our vaccines can do. [Read: Here’s why breakthroughs happen] The term breakthrough has long been a staple of the infectious-disease community, where it’s used to describe the detection of vaccine-preventable pathogens in immunized individuals. “This is definitely not a new idea,” Kevin Escandón, an infectious-disease physician and researcher at the University of Valle, in Colombia. But as a popular notion, it was always doomed to cause some confusion. Breakthrough is still used as an adjective of praise; the pandemic has now warped the word into a foreboding noun that tends to eclipse all clarifying qualifiers. “It’s confusing, it’s fuzzy, it’s already loaded,” Alison Buttenheim, who studies human behavior around vaccines at the University of Pennsylvania, told me. And when news appears in a headline or push alert, or on social media, “people pay attention to the word breakthrough” and not much else, Ryan McNamara, a virologist at the University of North Carolina at Chapel Hill, told me. That’s unfortunate, when the simple addition of asymptomatic or symptomatic can make all the difference. As they stand, blanket breakthroughs sound far scarier than they should. Joseph Allen, a public health researcher at Harvard, recently pointed out on Twitter one such ambiguity, in a study documenting a very small number of breakthrough infections at a prison. All were asymptomatic—though you wouldn’t know it from the paper’s title. To be clear, breakthroughs of any severity are an entirely expected part of the vaccination process. No vaccines are 100 percent effective at preventing infection or disease. But our current crop of COVID-19 shots comes pretty damn close with regards to stymieing symptoms, especially the severe ones that can signal a deadly case. The Moderna and Pfizer shots have consistently demonstrated very high COVID-prevention rates, often in the 90s; Johnson & Johnson, for the most part, isn’t far behind. Symptomatic breakthroughs are the cases that wedge themselves in the gap between excellent effectiveness and perfect effectiveness; in other words, we saw them coming. Even out in the messiness of the real world, symptomatic breakthrough cases are proving themselves quite rare. The overwhelming majority of the COVID-19 cases we’re seeing are among the unvaccinated. And when the virus does affect the immunized, it seems to accumulate to lower levels, and spread less enthusiastically to new hosts; it’s causing, on average, milder and more transient symptoms. All of this is a reminder of how vaccines work—by ratcheting up our immunity against the version of SARS-CoV-2 that the shots were formulated to mimic. If humans are wood that fuels a flame, and coronaviruses are the sparks that ignite it, vaccines are the fire suppressants that protect best against the worst of the viral burn: severe disease, hospitalization, and death. Stopping milder cases requires more immune investment, and blocking asymptomatic infections—ones that barely singe the bark—is most difficult of all. It’s part of why the vaccines’ goalposts were at first set so conservatively. “This is not a magic shield that just bounces coronavirus right off you,” McNamara told me. Considering that we first took aim at stopping disease, it’s great news that the majority of known breakthroughs have actually been asymptomatic infections, not COVID-19 cases. The proportions of silent breakthroughs reported by various studies and federal agencies are certainly undercounts, because vaccinated people aren’t regularly screened for the coronavirus. (On May 1, the CDC controversially switched its reporting strategy to documenting only breakthrough cases involving some form of hospitalization or death, skewing national counts further.) Since the vaccines first deployed, the news has only improved: Researchers didn’t bank on it, but in many people, the shots seem to stop the coronavirus from establishing itself at all. “The vaccines are better than anything we ever dreamed of,” Gounder told me, exceeding our first expectations in more ways than one. The shots are even holding their own against SARS-CoV-2 variants. A few versions of the virus have picked up mutations that help them dodge certain anti-coronavirus antibodies. But these genetic alterations chip away only incrementally at immune protection, rather than obliterating it. Against Delta, for instance, vaccines like Pfizer’s are still curbing severe disease, hospitalization, and death to an extraordinary degree. And while the shot’s strength has slightly slackened when it comes to milder illnesses and silent infections, those are simply lower hurdles for a virus to clear. Pfizer’s protection is still hitting its mark where it matters the most. (One asterisk on this is long COVID, a condition whose relationship to vaccination is still being actively researched.) None of this means, of course, that asymptomatic breakthrough infections should be ignored. To fully understand what the virus is doing and where it might be headed, experts need as comprehensive a picture as they can get of whom it’s afflicting, and what form those infections take, across the entire spectrum of disease. They also need to know how and when it’s most likely to spread. Asymptomatic infections are a part of that. Researchers around the world are still diligently sequencing any and all test-positive coronavirus samples they can, regardless of symptoms, in part to check whether any particular variants are disproportionately infiltrating the inoculated. They’re also tabulating who’s experiencing breakthroughs, and testing whether select populations might benefit from an early vaccine boost. [Read: What breakthrough infections can tell us] And when vaccines start to consistently falter against more severe tiers of disease—because of either a new variant, waning immune memory of the virus, or both—the diligent monitoring of breakthroughs will pick it up. Tracking milder breakthroughs is also crucial to figuring out how well the virus can be transmitted from vaccinated people, something that’s much more difficult to determine than whether inoculations merely block disease. From a surveillance standpoint, casting a broad net for breakthroughs—one that accounts for infections of all types—is essential, Buttenheim said. “That’s how you catch everything.” The question of which breakthroughs matter ultimately depends on another: What’s the goal of vaccination? Gounder thinks that, for now, the focus should stay on using immunizations to control COVID-19, especially while so much of the world remains unvaccinated; understanding whether we’re accomplishing that goal, then, hinges on symptomatic breakthroughs. Eventually, we’ll have the bandwidth to turn our attention to halting transmission and infection more comprehensively. Then, we’ll pull asymptomatic breakthroughs back into the conversation, with more data to guide our next move. from https://ift.tt/3AYlMuM Check out http://natthash.tumblr.com Lindsey Kaczmarek gets called an ambulance driver more often than she gets called a paramedic. “That’s absolutely not what I do,” she told me. What she does do is show up when someone needs medical help, figure out what’s wrong with them, and do whatever she can to help them survive the trip to the hospital—in her case, the Mayo Clinic in Rochester, Minnesota. The primary symptom for one in three 911 medical calls is simply “pain,” but during any given shift, Kaczmarek might attend to a heart attack, a stroke, a car crash, a labor and delivery gone wrong, a mental-health crisis, a shooting, or an elderly patient suffering from a severe urinary tract infection. “If they’re not breathing, I will breathe for them,” she said. “If their heart’s not beating, I will be the heartbeat for them.” The job of providing emergency medical services, or EMS, often resembles medical detective work, with limited clues, no specialists to consult, and very little, if any, of the sophisticated equipment available to doctors and nurses. But even though emergency medics—a catchall term used throughout this story for paramedics, emergency medical technicians, and emergency medical responders—handle tens of millions of calls in the United States each year and make life-altering decisions for their patients every day, they remain all but excluded from institutional medicine. “You’re basically like a glorified taxi,” says Sarayna McGuire, a Mayo Clinic emergency physician who has studied pre-hospital health care. The misconception that emergency medics provide transportation, not medicine, leaves them to cope with all sorts of indignities. “They’re used to being second-class citizens,” says Michael Levy, the president of the National Association of EMS Physicians. In one hour—during which they may respond to several 911 calls—the median paramedic or EMT makes a little more than $17. That’s half the hourly pay of registered nurses and less than one-fifth the pay of doctors—if they’re paid at all. During the pandemic, emergency medics were literally enclosed in rolling boxes with COVID-19 patients. But in some states, they were not prioritized alongside other essential health-care workers for the first round of vaccines. After delivering their precious cargo to a hospital, in many cases they don’t learn the final diagnosis, or whether their patient ever makes it back home. That medicine treats emergency medics like disposable, low-wage workers instead of the health-care professionals they are isn’t just unfortunate for the workers themselves—it also leads to less than optimal care for the rest of us on the day we may need it most. [Read: What it’s like to be a paramedic] The divide between health-care workers who respond to medical emergencies and those who treat patients in brick-and-mortar clinics is not new. In the 1800s, most accident victims were rushed to their homes, where they awaited medical care from private physicians. Hospitals started to staff their own 24/7 emergency departments only in the mid-20th century, in part thanks to the advent of lifesaving measures such as antibiotics, defibrillation, and blood transfusions. By the 1960s, a loose network of unregulated emergency medical systems had sprung up around the country. Undertakers and law-enforcement officers provided the bulk of hospital transports—known as “you call, we haul” missions—in the back of police cars, hearses, or delivery vans. These makeshift responders often had little or no formal medical instruction. “It was a little bit of the wild West,” says Chris Richards, an emergency-medicine physician at the University of Cincinnati. In the late ’60s and early ’70s, in response to growing concerns over traffic fatalities, the Department of Transportation—not the Department of Health and Human Services—developed a structured national EMS system, codifying the idea that emergency medics are drivers, not health-care workers. But the field has evolved significantly since then. Today, some emergency medics can dispense medications, and ambulances can house heart monitors and ultrasound machines. Over time, training and accreditation requirements have grown more and more rigorous. Still, in the eyes of some hospital staff, medics belong as much to today’s medical establishment as police officers and undertakers did in the 1960s. 
Many of Remle Crowe’s EMT runs in rural Ohio ended with a dissatisfying reminder of her place in medicine’s hierarchy. “I would drop [patients] off at the hospital and they would disappear,” she told me. As she sped off to the next call, she’d wonder about her last pickup, and what happened to them beyond the emergency-room doors. “There was no way of knowing,” Crowe said. [Read: What I learned as an EMT at the border wall] For the most part, EMS providers don’t learn whether the split-second decisions they make—say, whether to intubate someone—ultimately help their patients. Only about one in three EMS agencies reports having any access to electronic, patient-specific medical information. Many hospitals refuse to share any outcome data with EMS, claiming it’s a HIPAA violation (legally, it’s not). Ultimately, even in the most clear-cut of cases, a patient dies in the ambulance, an emergency medic may not learn the cause of death, or whether there was anything they could have done differently to change the outcome. “They’re kind of flying blind,” says Michael Sayre, the medical director of Seattle’s EMS. Leaving emergency medics out of the loop doesn’t only turn their jobs into repeated chronic cliffhangers. It also keeps them from improving the care they give to their patients, experts told me, robbing them of the opportunity to learn which of their instincts are correct and which to avoid. “Without creating this feedback loop, you really can’t get better,” Sayre says. “Of course medical errors happen because of that. You didn’t have enough of the puzzle pieces.” Few other fields, especially in the world of medicine, demand that its professionals tolerate working in a feedback-free environment. What if a chef never tasted a final dish? What if a teacher wasn’t allowed to grade tests? Would a lawyer be okay with never hearing a verdict? “If you don’t know if you’re bettering patients,” Kaczmarek said, “how do you keep coming to work?” [Read: ‘They just feel that they’ve been violated’] Some don’t. Emergency medics routinely struggle with high rates of burnout and job dissatisfaction, as well as PTSD and other mental illnesses. They are regularly bitten, punched, or otherwise assaulted by their patients, enduring a rate of occupational violence that is about 22 times higher than the average for all other U.S. workers. Altogether, the low pay, the absence of performance feedback, and the chronic mental and emotional toll “sends the message that no one cares about you and your work,” Crowe said. The treatment of emergency medics as chauffeurs and not clinicians—as a profession of nonprofessionals—means that not enough Americans choose this career. While nurses and doctors generally stick around in the field for decades, the average age for an emergency medic is just 34, and about 80 percent leave the job after seven years or less. This affects the quality of medical care provided: Data suggest that more experienced EMS clinicians save more patients and lead to better health outcomes. Retention issues in EMS are so widespread that some states and counties are plagued by staffing shortages and, in turn, delayed emergency care. “In many places the turnover in this workforce is very high,” Sayre says. “People accumulate these mental injuries that don’t heal, and they don’t work in the field long enough to become truly excellent.” As emergency medics continue to be undervalued, their work has never been more valuable. We needed them, and badly, during the pandemic, as 911 call volumes skyrocketed. We need them to respond to the urgent health needs of the country’s growing population of elderly people, who are more likely than in the past to suffer from several chronic conditions and take a dozen-plus prescriptions. We need them on the scene of mass shootings and drug overdoses. We need them as our planet continues to warm, leading to natural disasters, bouts of extreme weather, and infrastructure collapses. America’s health-care system ignores emergency medics at its own risk—and all of ours. from https://ift.tt/3k7bYse Check out http://natthash.tumblr.com Nicole Lawson spent the beginning of the pandemic incredibly worried about her daughter, who has asthma. Five-year-old Scarlett’s asthma attacks were already landing her in the ER or urgent care every few months. Now a scary new virus was spreading. Respiratory viruses are known triggers of asthma attacks, and doctors also feared at the time that asthma itself could lead to more severe coronavirus infections. So Lawson’s family in Ohio hunkered down quickly and masked up often to keep Scarlett healthy. The ensuing months, to everyone’s surprise, turned into “this beautiful year,” Lawson told me. Scarlett hasn’t had a single asthma attack. Not a single visit to the ER. Nothing. She’s breathing so much better, and all it took was a global pandemic that completely upended normal life. All around the country, doctors have spent the pandemic wondering why their patients with asthma were suddenly doing so well. Asthma attacks have plummeted. Pediatric ICUs have sat strangely empty. “We braced ourselves for significant problems for the millions of people living with asthma,” says David Stukus, Scarlett’s doctor at Nationwide Children’s Hospital. “It was the complete opposite. It’s amazing.” (Fears about people with asthma getting more severe COVID-19 infections haven’t been borne out either.) Studies in other countries, including England, Scotland, and South Korea, also found big drops in hospital and doctor’s-office visits for asthma attacks. The massive global experiment that is the pandemic is now leading doctors to rethink some long-held assumptions about the disease. Asthma is a chronic condition that occasionally flares up, leading to 3,500 deaths and 1.6 million emergency-room visits a year in the United States. These acute attacks can be triggered by a number of environmental factors: viruses, pollen, mold, dust mites, rodents, cockroaches, pet dander, smoke, air pollution, etc. Doctors have often scrutinized allergens that patients can control at home, such as pests and secondhand smoke. But patients have stayed at home for a year and suffered dramatically fewer asthma attacks—suggesting bigger roles for other triggers, especially routine cold and flu viruses, which nearly vanished this year with social distancing and masks. With life in the U.S. snapping back to normal, asthma doctors and patients are facing another new reality. Masks are going away; schools will be reopening in the fall. The pandemic unexpectedly reduced asthma attacks, and now doctors and patients have to navigate between what they know is possible in extraordinary conditions and what is practical in more ordinary ones. The most compelling evidence that asthma attacks truly did go down during the pandemic exists because of a stroke of good luck. Back in 2018, Elliot Israel, a pulmonologist at Brigham and Women’s Hospital, in Boston, began asking Black and Hispanic or Latino adults with asthma to track their attacks at home for a study called PREPARE. (These groups have disproportionate rates of severe asthma, compared with white patients.) Israel intended to compare two different ways of using long-term asthma medication, such as inhaled steroids. His team enrolled its last participant—patient No. 1,201—in March 2020. The COVID-19 shutdowns began a week later. “We were very lucky,” Israel told me. Because of the study’s timing, his team had plenty of data from before the pandemic. And because the participants were filling out monthly questionnaires from home, the shutdowns did not affect the data collection. Meanwhile, Israel, like his colleagues across the country, was noticing an eerie lack of non-coronavirus patients. Hospital visits for heart attacks and strokes were also dropping during the pandemic. Were asthma patients just avoiding the hospital because they were afraid of catching the virus? “That was the initial thought: What if these people are suffering at home?” says Justin Salciccioli, a pulmonologist at Brigham and Women’s Hospital and a co-author with Israel on the resulting paper about asthma attacks during the pandemic. The answer became clear as the monthly questionnaires started rolling in. The number of attacks the participants suffered at home really was dropping. It fell by 40 percent after the onset of the pandemic. “We know that this isn’t reluctance to go to the emergency room,” Israel said. “This is a true, real decrease.” In that case, why? Israel and his team didn’t see a clear pattern connected to changes in air pollution. People who normally worked outside the home, however, had bigger decreases in asthma attacks than those who worked at home (65 percent compared with 23 percent), perhaps because they were no longer being exposed to viruses and irritants at work. And people whose type of asthma is driven by environmental triggers also saw bigger improvements than those whose asthma is driven more by underlying inflammation. All of this suggests that people really were able to avoid triggers during the pandemic. Ordinary respiratory viruses may play a bigger role in asthma attacks than previously thought, Israel said. People with asthma, like everyone else who masked up and practiced social distancing, were this year exposed to many fewer viruses known to trigger flare-ups. Even asymptomatic infections that normally go unnoticed might cause an asthma attack in someone who’s airways are especially sensitive. “That extra irritation, that extra inflammation, pushes them over the edge,” Israel said. Asthma experts I spoke with all agreed that reduced viral exposure likely played a part in the drop, but the pandemic changed so many things at once that other factors are hard to rule out. Staying at home might have made it easier for people to keep up with their regular long-term asthma medication. They were also no longer exposed to potential triggers at work or school, such as diesel from school buses or chemicals in cleaning products. Asthma can be very individual, with exact triggers varying from person to person. But the overall picture is impossible to ignore: The sweeping changes to our social lives during the pandemic made asthma a lot easier to control. If viruses indeed play a bigger factor in asthma attacks than initially thought, doctors might have been mistakenly fixating on other factors. “We’ve forever talked about the environmental contribution to asthma. There are pollutants and irritants and allergens inside the home,” Stukus says. If these factors really were so important, though, asthma attacks should have gone up, not down, during the pandemic. It’s long been routine for doctors to question parents of kids with asthma about dust mites or cockroaches or smoking in the home, says Christopher Carroll, a pediatric-critical-care doctor at Connecticut Children’s. He’s asked these questions himself. But, he says, “the unstated implication when you’re asking about triggers like that is that those are causes of your child’s asthma.” This has the effect of blaming patients or parents of patients, when factors outside the home might actually play a bigger role. “We have this paternalistic attitude in medicine,” adds Janine Zee-Cheng, a pediatrician in Indiana. “You’re noncompliant with your medicines. Or you’re not monitoring your kid’s meds. Or you’re smoking indoors.” It’s “doctor knows best”—but the pandemic has exposed how much doctors did not know. Rethinking the role of viruses in asthma attacks is a bit more complicated in practice. COVID-19 precautions tamped down every other respiratory virus, but those precautions won’t last forever. Cases of respiratory syncytial virus, one cause of the common cold, have already spiked. Carroll expects that he will keep wearing a mask in hospitals, but masks are coming off everywhere else. More and more now, wearing one means sticking out. And unfortunately, the health benefits of a face mask have also been overwhelmed by its potency as a political symbol. This is what worries Lawson, as Scarlett goes off with her friends and begins pre-K in the fall. She can’t keep Scarlett cocooned forever. Her daughter will be exposed to viruses. “I would be lying if I said it didn’t make me anxious,” Lawson said. Masking up in the winter seems like a no-brainer, but she can already imagine the judgment her family might face. This choice isn’t about politics, though. It’s about Scarlett’s asthma. Lawson remembers the two Thanksgivings in a row when Scarlett got so sick, she had to be hospitalized. It didn’t happen this past Thanksgiving, and she hopes it never happens again. from https://ift.tt/36niMdr Check out http://natthash.tumblr.com Last winter, when vaccines were still incredibly scarce in the United States, Ashish Jha told The Atlantic that he was feeling optimistic about summer: By July 4, Jha, the dean of the Brown University School of Public Health, expected enough people to be vaccinated that he could host a backyard barbecue. Indeed, Jha confirmed to me this week, he will be grilling burgers and hot dogs for friends this Fourth of July. He had predicted back in the winter that guests would still need to mask up indoors, but even that feels unnecessary now. “Fifteen, 20 vaccinated people inside my house, if it starts raining, feels very safe,” he said. This is because, he added, he lives in Massachusetts, which has one of the lowest COVID-19 case rates in the nation (fewer than one new case per 100,000 people a day) and one of the highest vaccination rates (82 percent of adults have had at least one dose). His town, Newton, is an outlier even among outliers: More than 95 percent of people older than 30 have gotten at least one dose. It’s one of the safest places in the world with respect to the coronavirus. The outlook is dramatically different elsewhere in the country. COVID-19 cases are rising sharply in several states with low vaccine coverage, fueled by the spread of the coronavirus’s more transmissible Delta variant. In southwest Missouri, understaffed hospitals are already having to send COVID-19 patients hundreds of miles away. The same July 4 party that is very safe in Massachusetts is riskier in Missouri, where much more virus is circulating (15 new cases per 100,000 people a day) and many fewer adults are at least partially vaccinated (56 percent). Earlier this year, the Biden administration set a goal of partially vaccinating at least 70 percent of adults by Independence Day. The U.S. will narrowly miss the mark; the number is currently hovering around 67 percent. When you zoom in closer, though, we’re doing both better and worse than that, depending on where you look. Our pandemic fates have diverged. The plateauing national case numbers obscure two simultaneous trends: an uptick in several sparsely vaccinated states and continued declines in well-vaccinated ones. In this new reality, a single national strategy no longer makes sense. On Thursday, the White House announced that it would be sending “surge response” teams to hot spots with rising caseloads and low vaccination rates. The COVID-19 situation in different parts of the country has diverged so much now that Peter Hotez, a vaccine expert at Baylor College of Medicine, has suggested that the CDC issue two separate sets of guidelines. Delta’s increased transmissibility only exacerbates the divide between the inoculated and the un-inoculated. As my colleague Ed Yong writes, “Vaccinated people are safer than ever despite the variants. But unvaccinated people are in more danger than ever because of the variants.” For people who are fully vaccinated, Delta poses very little direct threat. Its mutations do erode immunity slightly, but most breakthrough infections that result are mild or even asymptomatic. For entirely unvaccinated people, however, this means that Delta actually poses a double danger. They cannot rely on direct immunity from a vaccine, of course. But they also cannot rely as much on the herd immunity of vaccinated people around them if the variant is causing more breakthrough infections The U.S. was always going to struggle to vaccinate its way to the herd-immunity threshold for COVID-19—the point at which enough people have gained immunity that viral spread is limited. As I wrote in February, America’s vaccine reluctance and the evolution of new variants that can evade vaccines make herd immunity difficult to achieve and maintain. The upshot is that the coronavirus will keep circulating, looking for new bodies it can infect. For the unvaccinated, getting infected is probably a matter of time. “Everybody will end up getting immunity to this virus eventually,” Jha told me. “You’ll either get it through vaccination or infection.” This time last year, vaccines were still a distant hope. It was hard to imagine, last July 4, that we would have this many different vaccines that are this effective. It was hard to imagine scaling up factories to manufacture this many doses so quickly—more than enough for every American. But we also did not imagine that variants would emerge and how quickly they would widen the divide between the vaccinated and the unvaccinated. Here we are a year later, with too many doses and too few willing arms, at a time when the advantages of vaccination are clearer than ever. from https://ift.tt/3dBiMdx Check out http://natthash.tumblr.com The most reliable way to inflame the heart is to bother it with a virus. Many types of viruses can manage it--coxsackieviruses, flu viruses, herpesviruses, adenoviruses, even the new coronavirus, SARS-CoV-2. Some of these pathogens bust their way straight into cardiac tissue, damaging cells directly; others rile up the immune system so overzealously that the heart gets caught in the crossfire. Whatever the cause, the condition is typically mild, but can occasionally be severe enough to permanently compromise the heart, requiring lifesaving interventions including ventilators or organ transplants; in very rare cases, it’s fatal. That is decidedly not what we’re seeing in the CDC’s recent reports. The agency has confirmed more than 500 cases of myocarditis or pericarditis—inflammation of the heart itself or of the lining that shrouds it—in people younger than 30 who recently received Pfizer-BioNTech’s or Moderna’s two-shot COVID-19 vaccines. These events are, so far, not matching the most terrifying versions of the condition, which have been observed with coronavirus infections. Rather, compared with more typical cases of myocarditis, the ones linked to the vaccines, on average, involve briefer symptoms and speedier recoveries, even with less invasive treatments. Still, the incidents are showing up in the few days that follow each vaccine’s second dose at higher-than-expected rates, especially in boys and young men, and no one is yet sure why. The CDC’s Advisory Committee on Immunization Practices, or ACIP, met last week to weigh the risks and benefits of keeping the vaccines in circulation among the nation’s eligible youngest. It rapidly reached a familiar verdict: The perks of immunization far outweigh the potential drawbacks of these side effects and others. Days later, the FDA appended a warning about the rare events onto its fact sheets for the vaccines. Most of the experts I spoke with enthusiastically backed both agencies’ decisions without reservation. Vaccines, they said, remain our most powerful defensive tool against the coronavirus; if anything, staying unimmunized is the bigger gamble when it comes to severe organ inflammation. But several of them also noted that this particular side effect, and the country’s response to it, represents a new type of stumbling block for our inoculations. The shots themselves, which are excellent, haven’t changed. But the context in which we’re deploying them has. This potential side effect is the first to concentrate like this in children, who are still relatively new to COVID-19 vaccination. Post-vaccine myocarditis still isn’t well defined; neither are the full consequences of pediatric COVID-19. For more than a year now, the pandemic has forced people to pit a pile of risky unknowns against another pile of risky unknowns, but anything that concerns kids’ health is bound to make tensions run particularly high. A recent Kaiser Family Foundation poll found that recent news of heart problems was a top-of-mind concern for many parents, who are often less likely to vaccinate their children than themselves. That the recent cases of post-vaccination myocarditis are relatively mild is, to start, “very reassuring,” said Judith Guzman-Cottrill, a pediatric-infectious-disease physician at Oregon Health & Science University (OHSU), who helped identify some of the earliest instances of inflammation back in April. Symptoms have lasted just a couple of days; most of the inflammation has been fairly straightforward to treat. According to Katherine Poehling, a pediatrician at Wake Forest Baptist Medical Center and an ACIP member, no deaths or severe outcomes had been reported at the time of last week’s meeting. “This is not like any myocarditis I’m used to seeing,” said Grace Lee, a pediatrician at Stanford and a member of ACIP. Though most of the identified patients have been hospitalized, “it’s because we wanted to monitor them, out of an abundance of caution,” said Sallie Permar, the chair of pediatrics at Weill Cornell Medicine and New York–Presbyterian Komansky Children’s Hospital. Many of these patients were discharged after receiving little more than over-the-counter pain medication as therapy. “Even the kids are asking, ‘Why am I going to the hospital?’” Permar said. But vaccine-induced heart inflammation of any severity still warrants concern, especially without a known root cause. Myocarditis and pericarditis, which mysteriously skew young and male, can arise from an array of triggers, including bacteria and fungi as well as medications and autoimmune disease, but many cases go entirely unexplained. There’s no curative, or even standard, treatment for either condition; doctors try to manage symptoms and tamp down inflammation, said John Jarcho, a cardiovascular-medicine specialist at Brigham and Women’s Hospital, in Boston. Cases related to vaccines are more puzzling still. Only a few immunizations have previously been linked to heart inflammation, among them the smallpox vaccine, which looks nothing like the jabs we’re doling out now. Researchers remain unsure what’s triggering the body to act out, or which children, especially which adolescent boys, might be most vulnerable. Mark Slifka, a vaccinologist at OHSU, told me he suspects the inflammation is caused by a bit of friendly fire—an extreme manifestation of the side effects already known to come with the Pfizer and Moderna vaccines, especially after the second injection. Perhaps immune cells are pumping out excessive alarm signals that marshal forces to the heart, or maybe the body’s defenders, confused by a vaccine ingredient, mistakenly wallop cardiac tissue. (Kids’ immune systems are generally feistier than adults’.) We also don’t yet know whether these brief bouts of inflammation are leaving lasting damage, perhaps through subtle scarring of the heart, said Jeremy Asnes, a co-director of Yale New Haven Children’s Hospital Heart Center. His team has seen about a dozen adolescents with the conditions and will conduct follow-ups over the next several months. Guzman-Cottrill is doing the same in Oregon. All of these factors make the risk of this complication tough to quantify, and several researchers have criticized the CDC’s recent evaluation. But most of the experts I spoke with said that the calculations still come out strongly in favor of vaccination, in part because of another set of disconcerting ambiguities, this time on the side of the virus. SARS-CoV-2 does, on average, cause less severe disease in kids. But less is no longer a terribly comforting qualifier. Millions of young people have been infected; thousands have been hospitalized; more than 300 younger than age 18 have died. We still don’t know how many kids hit by the virus will go on to develop long COVID, and the CDC has also logged more than 4,000 cases of a severe inflammatory complication called MIS-C. This condition can itself involve severe myocarditis—far worse than the cases that typically follow vaccination—and seems to carry a 1 percent fatality rate. It also disproportionately impacts people of color. “If you think about all the risks that come with getting COVID itself, those are way more common” than the very low myocarditis rates we’re seeing with vaccines, Permar told me. “If you’re playing the numbers, every time you would choose to vaccinate your child to prevent disease.” Not all experts have taken the same stance; some have argued that there’s no rush to vaccinate kids. Coronavirus transmission in the United States has, after all, been dropping for months. But while absolute numbers of infections are down, the face of COVID-19 in this country has shifted. With vaccines concentrated among older adults, younger individuals are now shouldering more of the nation’s coronavirus burden: About a third of the infections reported to the CDC in May were in people ages 12 to 29, many of them unvaccinated. And the low spread we’re seeing right now won’t necessarily hold against the rise of highly contagious variants like Delta. It’s a terrible time to lose the momentum we’ve gained. “I’m not looking at transmission rates now,” Guzman-Cottrill told me. “I’m looking at what might happen in fall and winter.” Vaccination would shield kids, as well as those around them; immunizing more today means better protection later, even if we can’t yet see the threats on the horizon. [Read: The 3 simple rules that underscore the danger of Delta] Doctors are carefully monitoring new cases that come their way. If the inflammation they’re seeing continues to be mild, Asnes said, the people who experience it might be able to leave the hospital even earlier, or never check in at all. But if there’s an unexpected uptick in severity, experts will reassess. More vaccine options could also change these calculations. For now, Pfizer is the only COVID-19 shot that can be used in children. But other vaccines with gentler side-effect profiles, including those from J&J and Novavax, could be easier on the heart, OHSU’s Slifka said. In the interim, some experts have floated the notion of tinkering with Pfizer and Moderna dosing to safeguard younger heart tissue. Vinay Prasad, a hematologist-oncologist at UC San Francisco who has been very critical of the CDC’s evaluation of heart inflammation, told me he’d like to see the agency consider skipping second doses, or trimming doses down for at-risk populations. Neither of those strategies has been rigorously tested, though. Dose-reducing revisions run the risk of blunting protection, which might have contributed to the failure of the CureVac mRNA vaccine. Forgoing second doses could also backfire: Repeat shots seem crucial for conferring strong protection against variants like Delta. Then again, kids aren’t just tiny adults, and adapting vaccines to their needs isn’t just a matter of bending down to stick a needle in a shorter, smaller person. Youthful immune systems react more enthusiastically to certain inoculations, which can mean more side effects, or simply that they need less vaccine to mount a defense. Several existing vaccines, such as the ones we use for chickenpox/shingles and tick-borne encephalitis, come in lower doses for children; Moderna and Pfizer are adopting this same strategy in their clinical trials for kids under 12. As they’re ushered into younger populations, our vaccines can be expected to undergo some growing pains. The key, experts told me, is to stay flexible. Everyone’s chess board will end up looking a little different. Yale pediatrician Thomas Murray, whose two older children have already gotten their shots, told me he and his younger son, who will soon turn 12, will “engage in shared decision making,” he said. “I don’t want him to have to worry about him getting COVID.” Cornell’s Permar told me her family heard of the myocarditis reports the day before her 12-year-old son, Sam, was scheduled to receive his second dose of Pfizer. “We didn’t question it,” she said. “Looking at the numbers, there are so many more benefits of my son getting the vaccine.” Still, she kept a close eye on him for a few days after his shot. from https://ift.tt/3hGlGzh Check out http://natthash.tumblr.com Fifteen months after the novel coronavirus shut down much of the world, the pandemic is still raging. Few experts guessed that by this point, the world would have not one vaccine but many, with 3 billion doses already delivered. At the same time, the coronavirus has evolved into super-transmissible variants that spread more easily. The clash between these variables will define the coming months and seasons. Here, then, are three simple principles to understand how they interact. Each has caveats and nuances, but together, they can serve as a guide to our near-term future. 1. The vaccines are still beating the variantsThe vaccines have always had to contend with variants: The Alpha variant (also known as B.1.1.7) was already spreading around the world when the first COVID-19 vaccination campaigns began. And in real-world tests, they have consistently lived up to their extraordinary promise. The vaccines from Pfizer-BioNTech and Moderna reduce the risk of symptomatic infections by more than 90 percent, as does the still-unauthorized one from Novavax. Better still, the available vaccines slash the odds that infected people will spread the virus onward by at least half and likely more. In the rare cases that the virus breaks through, infections are generally milder, shorter, and lower in viral load. As of June 21, the CDC reported just 3,907 hospitalizations among fully vaccinated people and just 750 deaths. Could the Delta variant (also known as B.1.617.2) change that picture? Data from the U.K. suggest that it is 35 to 60 percent better at spreading than Alpha, which was already 43 to 90 percent more transmissible than the original virus. (It may also be deadlier, but that’s still unclear.) It now causes 26 percent of new infections in the U.S. and will soon cause most of them. But even against Delta, full vaccination—with a heavy emphasis on full—is effective. Two doses of Pfizer’s vaccine are still 88 percent effective at preventing symptomatic Delta infections, according to a U.K. study, and 96 percent effective at preventing hospitalization. (A single dose, however, is only 33 percent effective at stopping symptomatic infection.) Israel, a highly vaccinated country, is experiencing a small Delta surge, but so far, none of the new cases has been severe. And while about 30 percent of those new cases have been in fully vaccinated people, this statistic reflects, in part, the country’s success at vaccination. Because Israel has fully vaccinated about 85 percent of adults, you would expect many new infections to occur in that very large group. “It does seem like the vaccines are holding their own against the variants,” Emma Hodcroft, an epidemiologist at the University of Bern, told me. “That’s something we can take some comfort from.” But the coronavirus can cause serious problems without triggering severe infections. Because people can develop long COVID without ending up in the hospital, could Delta still cause long-term symptoms even if vaccines blunt its sting? The anecdotal reports of long-haulers whose symptoms abated after vaccination might suggest otherwise, but “we don’t know enough to say,” Bill Hanage, an epidemiologist at Harvard, told me. Another crucial question that “we really need to understand is the nature of transmission from breakthrough cases,” Hanage said. Worryingly, a recent study documented several cases during India’s spring surge in which health-care workers who were fully vaccinated with AstraZeneca’s vaccine were infected by Delta and passed it on. If other vaccines have similar vulnerabilities, vaccinated people might have to keep wearing masks indoors to avoid slingshotting the virus into unvaccinated communities, especially during periods of high community transmission. “That is unfortunately the direction this is headed,” says Ravindra Gupta, a clinical microbiologist at the University of Cambridge, who led the study. Israel has reimposed a mask mandate, while Los Angeles County and the World Health Organization have advised that vaccinated people should wear masks indoors. And such measures make sense because ... 2. The variants are pummeling unvaccinated peopleVaccinated people are safer than ever despite the variants. But unvaccinated people are in more danger than ever because of the variants. Even though they’ll gain some protection from the immunity of others, they also tend to cluster socially and geographically, seeding outbreaks even within highly vaccinated communities. The U.K., where half the population is fully vaccinated, “can be a cautionary tale,” Hanage told me. Since Delta’s ascendancy, the country’s cases have increased sixfold. Long-COVID cases will likely follow. Hospitalizations have almost doubled. That’s not a sign that the vaccines are failing. It is a sign that even highly vaccinated countries host plenty of vulnerable people. Delta’s presence doesn’t mean that unvaccinated people are doomed. When Alpha came to dominate continental Europe, many countries decided not to loosen their restrictions, and the variant didn’t trigger a huge jump in cases. “We do have agency,” Hodcroft said. “The variants make our lives harder, but they don’t dictate everything.” In the U.S., most states have already fully reopened. Delta is spreading more quickly in counties with lower vaccination rates, whose immunological vulnerability reflects social vulnerability. Black and Hispanic Americans are among the most likely groups to die of COVID-19 but the least likely to be vaccinated. Immunocompromised people may not benefit from the shots. Children under 12 are still ineligible. And unlike in many other wealthy countries, the pace of vaccinations in America is stalling because of lack of access, uncertainty, and distrust. To date, 15 states, most of which are in the South, have yet to fully vaccinate half their adults. “Watch the South in the summer,” Hanage said. “That’ll give us a flavor of what we’re likely to see in the fall and winter.” Globally, vaccine inequities are even starker. Of the 3 billion vaccine doses administered worldwide, about 70 percent have gone to just six countries; Delta has already been detected in at least 85. While America worries about the fate of states where around 40 percent of people are fully vaccinated, barely 10 percent of the world’s population has achieved that status, including just 1 percent of Africa’s. The coronavirus is now tearing through southern Africa, South America, and Central and Southeast Asia. The year is only half over, but more people have already been infected and killed by the coronavirus in 2021 than in 2020. And new variants are still emerging. Lambda, the latest to be recognized by the WHO, is dominant in Peru and spreading rapidly in South America. Many nations that excelled at protecting their citizens are now facing a triple threat: They controlled COVID-19 so well that they have little natural immunity; they don’t have access to vaccines; and they’re besieged by Delta. At the start of this year, Vietnam had recorded just 1,500 COVID-19 cases—fewer than many individual American prisons. But it is now facing a huge Delta-induced surge when just 0.19 percent of its people have been fully vaccinated. If even Vietnam, which so steadfastly held the line against COVID-19, is now buckling under the weight of Delta, “it’s a sign that the world may not have that much time,” Dylan Morris, an evolutionary biologist at UCLA, told me. With Delta and other variants spreading so quickly, “my great fear is that in not very long, everyone globally will either have been vaccinated or infected,” Morris said. He didn’t want to pinpoint a time frame, but “I don’t want to bet that we have more than a year,” he said. And richer nations would be wrong to think that the variants will spare them, because ... 3. The longer Principle No. 2 continues, the less likely No. 1 will holdWhenever a virus infects a new host, it makes copies of itself, with small genetic differences—mutations—that distinguish the new viruses from their parents. As an epidemic widens, so does the range of mutations, and viruses that carry advantageous ones that allow them to, for example, spread more easily or slip past the immune system to outcompete their standard predecessors. That’s how we got super-transmissible variants like Alpha and Delta. And it’s how we might eventually face variants that can truly infect even vaccinated people. None of the scientists I talked with knows when that might occur, but they agree that the odds shorten as the pandemic lengthens. “We have to assume that’s going to happen,” Gupta told me. “The more infections are permitted, the more probable immune escape becomes.” If that does happen, when would we know? This is the first pandemic in history in which scientists are sequencing the genes of a new virus, and tracking its evolution, in real time—that’s why we know about the variants at all. Genomic surveillance can tell which mutations are rising to the fore, and lab experiments can show how these mutations change the virus—that’s how we know which variants are concerning. But even with such work “happening at incredible speed,” Hodcroft told me, “we can’t test every variant that we see.” Many countries lack sequencing facilities, and those that have them can be easily swamped. “Again and again, we have seen variants pop up in places that are under extraordinary strain because those variants are causing large surges,” Hanage said. Delta ripped its way through India, “but we only understood it when it started causing infections in the U.K.—a country that had plenty of scientists with sequencers and less to do.” So the first sign of a vaccine-beating variant will likely be an uptick in disease. “If vaccinated folks start getting sick and enter hospitals with symptoms, we’ll have a pretty good picture of what’s going on,” Maia Majumder, an epidemiologist at Harvard Medical School and Boston Children's Hospital, told me. We’re unlikely to be as vulnerable as we were at the beginning of the pandemic. The vaccines induce a variety of protective antibodies and immune cells, so it’s hard for a variant virus to evade them all. These defenses also vary from person to person, so even if a virus eludes one person’s set, it might be stymied when it jumps into a new host. “I don’t think there’ll suddenly be a variant that pops up and evades everything, and suddenly our vaccines are useless,” Gupta told me. “It’ll be incremental: With every stepwise change in the virus, a chunk of protection is lost in individuals. And people on the edges—the vulnerable who haven’t mounted a full response—will end up bearing the cost.” If that happens, vaccinated people might need booster shots. Those should be possible: The mRNA vaccines produced by Moderna and Pfizer should be especially easy to revise against changing viruses. But “if we need boosters, I worry that countries that are able to produce vaccines will do so for their own populations, and the division around the world will become even greater,” Maria van Kerkhove, an infectious-disease epidemiologist at the WHO, told me. The discussion about vaccine-beating variants echoes the early debates about whether SARS-CoV-2 would go pandemic. “We don’t think too well as a society about low-probability events that have far-reaching consequences,” Majumder told me. “We need to prepare for a future where we are doing vaccine rollout again, and we need to figure out how to do that better.” In the meantime, even highly vaccinated nations should continue investing in other measures that can control COVID-19 but have been inadequately used—improved ventilation, widespread rapid tests, smarter contact tracing, better masks, places in which sick people can isolate, and policies like paid sick leave. Such measures will also reduce the spread of the virus among unvaccinated communities, creating fewer opportunities for an immune-escape variant to arise. “I find myself the broken record who always emphasizes all the other tools we have,” van Kerkhove said. “It’s not vaccines only. We’re not using what we have at hand.” The WHO’s decision to name variants after the Greek alphabet means that at some point, we’ll probably be dealing with an Omega variant. Our decisions now will determine whether that sinister name is accompanied by equally sinister properties, or whether Omega will be just an unremarkable scene during the pandemic’s closing act. from https://ift.tt/3hbbkYM Check out http://natthash.tumblr.com |
Authorhttp://natthash.tumblr.com Archives
April 2023
Categories |
 RSS Feed
RSS Feed
