|
Many Americans have relied on the Affordable Care Act during the pandemic, but an upcoming Supreme Court case may invalidate it. With worries about the ACA looming over Amy Coney Barrett’s confirmation hearings, staff writer James Hamblin and executive producer Katherine Wells are joined on the podcast Social Distance by Karen Pollitz, a senior fellow at the Kaiser Family Foundation. An expert on the landmark health-care law, Pollitz gives them a refresher on what the ACA did—and what could happen if it goes away in the time of the coronavirus. Listen here to their conversation here: Subscribe to Social Distance on Apple Podcasts, Spotify, or another podcast platform to receive new episodes as soon as they’re published. What follows is a transcript of their conversation, edited and condensed for clarity: James Hamblin: What is in jeopardy now with the case before the Supreme Court? Karen Pollitz: The case that was filed challenges the whole Affordable Care Act. Republican state officials and the Trump administration have filed briefs saying, Now that the individual-mandate penalty is gone, you have to throw out the entire law. All of it: the Medicaid expansion, the market reforms, the subsidies, the insurance standards. There were tons of changes across our health-care system in the ACA. And the case that’s before the Court says all of that is invalidated because this one provision no longer has a penalty. Hamblin: And the initial challenge to the ACA in the Supreme Court was over the mandate being unconstitutional? Katherine Wells: Yeah, I thought we already went through this. Didn’t the Supreme Court already say the law is fine? Pollitz: It did, but the argument is that the Supreme Court ruled that because there were penalties tied to the mandate, that the mandate was really a tax provision. And Congress clearly has authority under the Constitution to levy taxes, so that was okay. Now the plaintiffs are saying that the tax penalty is gone, so it isn’t a tax anymore. They say there’s a mandate—albeit with no penalty—but that’s still unconstitutional, and so the whole law has to come down. A lot of legal scholars look at this—even conservative legal scholars—and say that’s kind of ridiculous on its face. But that is the case that is before the Supreme Court now. Wells: Is the likely outcome that the Supreme Court just says, “Okay, sure, we can’t have a mandate, but the law isn’t unconstitutional”? Pollitz: I certainly won’t say what a likely outcome is—2020’s been quite a year. And now, with the Supreme Court makeup changing, nobody knows what the outcome is. At the one end, the Court could agree and invalidate the whole thing. At the other end, they could say this is stupid on its face, and dismiss the case. In between, they could say the mandate now is unconstitutional, but there’s this severability argument. Maybe the whole law doesn’t have to go, but what would have to go with it? Earlier briefs by the Trump administration in memos to Congress suggested that those market reforms would have to go, because the mandate was gone. So the individual market could go back to turning me down because I’m a cancer survivor. Group health plans at work could go back to excluding your preexisting conditions. Group plans did that before the ACA. So that severability argument lies in between the two extreme outcomes and, honestly, nobody knows with a new Court how this might work. I think there are arguments about the constitutionality of laws that the Congress enacts, what these laws can and can’t require, and how they have to be crafted ... All of that is wrapped up in this case right now, but for people, it just feels kind of scary. I mean, 20 million people could lose their coverage if this law gets erased. And a whole lot of us—over 50 million of us adults—could be again labeled uninsurable. Wells: There’s such a focus on the ACA this week with the Senate confirmation hearings, because if the new justice is confirmed before oral arguments in November, she gets to be part of the decision? Pollitz: Right. This is the third trip to the Supreme Court for the Affordable Care Act, and it’s been upheld twice before by a vote of 5–4. Now the expectation is that 5–4 is going to be harder to achieve this time. Wells: We’ve talked about preexisting conditions. Is COVID-19 a preexisting condition? Pollitz: It could be. It absolutely could be. Twenty years ago, I did a study of health-insurance companies that sold individual health insurance. We presented them with hypothetical applicants with a variety of heights, weights, ages, conditions, diagnoses, medications, etc. And we asked them: Would you sell these people coverage? At the one extreme, we had a young man who had HIV, and he got turned down every time. At the other extreme, we had a young woman who was in excellent health, except she had seasonal hay fever. And she got turned down several times. She was offered coverage most of the time. But in all but a few of those offers, she was offered a policy at a surcharge premium. Okay, we’ll sell you coverage, but you’re going to pay 50 percent more than the advertised price. She got offered policies that excluded her allergies. She also got a couple of policies that excluded her entire upper respiratory system, policies that excluded the drug benefit. Medical underwriting was pretty fussy in those days. Crosswalk that to COVID-19: It’s a little trickier. This is still a new condition, and uncertainty is something that medical underwriters just hate. They don’t want to sign on and promise to pay all your claims if they’re not sure what you might need. For now, in the first six or so months of COVID-19, we know that for most people, it’s an awful infection and uncomfortable, but it’s relatively mild. But we also know there are some folks, they may continue to have symptoms for an extended period of time and they could be severe, with long-term serious damage to the lungs, the heart, the immune system ... I think insurers would worry about that, and certainly if they saw a recent case of COVID-19, I think underwriters could act on that. Another thing they might worry about would be people who just test frequently. Maybe they drive an Uber or they’re a cashier at a store or they deliver groceries. They’re in contact with the public a lot. They’re exposed. And they’re worried about getting sick. Just being at elevated risk for COVID-19, I think, is something that insurers would look at. In addition to being uninsurable for your health condition, insurers also had lists of uninsurable occupations. I was just looking at one of the old underwriting manuals, and on that list was “taxi driver.” There was “coal miner” and “logger”—dangerous jobs, of course—but way before COVID-19, “taxi driver” was on the list, just because you get exposed to a lot of things. So, yeah, I think in a medically underwritten insurance market, COVID-19 could make it harder for you to get insurance. And if you were able to buy it, if you’re at risk, you may well be offered a policy that just excludes all treatment for anything related to COVID-19. from https://ift.tt/3nYhgWz Check out http://natthash.tumblr.com
0 Comments
Many Americans have relied on the Affordable Care Act during the pandemic, but an upcoming Supreme Court case may invalidate it. With worries about the ACA looming over Amy Coney Barrett’s confirmation hearings, staff writer James Hamblin and executive producer Katherine Wells are joined on the podcast Social Distance by Karen Pollitz, a senior fellow at the Kaiser Family Foundation. An expert on the landmark health-care law, Pollitz gives them a refresher on what the ACA did—and what could happen if it goes away in the time of the coronavirus. Listen here to their conversation here: Subscribe to Social Distance on Apple Podcasts, Spotify, or another podcast platform to receive new episodes as soon as they’re published. What follows is a transcript of their conversation, edited and condensed for clarity: James Hamblin: What is in jeopardy now with the case before the Supreme Court? Karen Pollitz: The case that was filed challenges the whole Affordable Care Act. Republican state officials and the Trump administration have filed briefs saying, Now that the individual-mandate penalty is gone, you have to throw out the entire law. All of it: the Medicaid expansion, the market reforms, the subsidies, the insurance standards. There were tons of changes across our health-care system in the ACA. And the case that’s before the Court says all of that is invalidated because this one provision no longer has a penalty. Hamblin: And the initial challenge to the ACA in the Supreme Court was over the mandate being unconstitutional? Katherine Wells: Yeah, I thought we already went through this. Didn’t the Supreme Court already say the law is fine? Pollitz: It did, but the argument is that the Supreme Court ruled that because there were penalties tied to the mandate, that the mandate was really a tax provision. And Congress clearly has authority under the Constitution to levy taxes, so that was okay. Now the plaintiffs are saying that the tax penalty is gone, so it isn’t a tax anymore. They say there’s a mandate—albeit with no penalty—but that’s still unconstitutional, and so the whole law has to come down. A lot of legal scholars look at this—even conservative legal scholars—and say that’s kind of ridiculous on its face. But that is the case that is before the Supreme Court now. Wells: Is the likely outcome that the Supreme Court just says, “Okay, sure, we can’t have a mandate, but the law isn’t unconstitutional”? Pollitz: I certainly won’t say what a likely outcome is—2020’s been quite a year. And now, with the Supreme Court makeup changing, nobody knows what the outcome is. At the one end, the Court could agree and invalidate the whole thing. At the other end, they could say this is stupid on its face, and dismiss the case. In between, they could say the mandate now is unconstitutional, but there’s this severability argument. Maybe the whole law doesn’t have to go, but what would have to go with it? Earlier briefs by the Trump administration in memos to Congress suggested that those market reforms would have to go, because the mandate was gone. So the individual market could go back to turning me down because I’m a cancer survivor. Group health plans at work could go back to excluding your preexisting conditions. Group plans did that before the ACA. So that severability argument lies in between the two extreme outcomes and, honestly, nobody knows with a new Court how this might work. I think there are arguments about the constitutionality of laws that the Congress enacts, what these laws can and can’t require, and how they have to be crafted ... All of that is wrapped up in this case right now, but for people, it just feels kind of scary. I mean, 20 million people could lose their coverage if this law gets erased. And a whole lot of us—over 50 million of us adults—could be again labeled uninsurable. Wells: There’s such a focus on the ACA this week with the Senate confirmation hearings, because if the new justice is confirmed before oral arguments in November, she gets to be part of the decision? Pollitz: Right. This is the third trip to the Supreme Court for the Affordable Care Act, and it’s been upheld twice before by a vote of 5–4. Now the expectation is that 5–4 is going to be harder to achieve this time. Wells: We’ve talked about preexisting conditions. Is COVID-19 a preexisting condition? Pollitz: It could be. It absolutely could be. Twenty years ago, I did a study of health-insurance companies that sold individual health insurance. We presented them with hypothetical applicants with a variety of heights, weights, ages, conditions, diagnoses, medications, etc. And we asked them: Would you sell these people coverage? At the one extreme, we had a young man who had HIV, and he got turned down every time. At the other extreme, we had a young woman who was in excellent health, except she had seasonal hay fever. And she got turned down several times. She was offered coverage most of the time. But in all but a few of those offers, she was offered a policy at a surcharge premium. Okay, we’ll sell you coverage, but you’re going to pay 50 percent more than the advertised price. She got offered policies that excluded her allergies. She also got a couple of policies that excluded her entire upper respiratory system, policies that excluded the drug benefit. Medical underwriting was pretty fussy in those days. Crosswalk that to COVID-19: It’s a little trickier. This is still a new condition, and uncertainty is something that medical underwriters just hate. They don’t want to sign on and promise to pay all your claims if they’re not sure what you might need. For now, in the first six or so months of COVID-19, we know that for most people, it’s an awful infection and uncomfortable, but it’s relatively mild. But we also know there are some folks, they may continue to have symptoms for an extended period of time and they could be severe, with long-term serious damage to the lungs, the heart, the immune system ... I think insurers would worry about that, and certainly if they saw a recent case of COVID-19, I think underwriters could act on that. Another thing they might worry about would be people who just test frequently. Maybe they drive an Uber or they’re a cashier at a store or they deliver groceries. They’re in contact with the public a lot. They’re exposed. And they’re worried about getting sick. Just being at elevated risk for COVID-19, I think, is something that insurers would look at. In addition to being uninsurable for your health condition, insurers also had lists of uninsurable occupations. I was just looking at one of the old underwriting manuals, and on that list was “taxi driver.” There was “coal miner” and “logger”—dangerous jobs, of course—but way before COVID-19, “taxi driver” was on the list, just because you get exposed to a lot of things. So, yeah, I think in a medically underwritten insurance market, COVID-19 could make it harder for you to get insurance. And if you were able to buy it, if you’re at risk, you may well be offered a policy that just excludes all treatment for anything related to COVID-19. from https://ift.tt/3nYhgWz Check out http://natthash.tumblr.com Sometime in the coming months, our prayers will have been answered. The researchers will have pulled their all-nighters, mountains will have been moved, glass vials will have been shipped, and a vaccine that protects us from the novel coronavirus will be here. We will all clamber to get it so we can go back to school, work, restaurants, and life. All of us, that is, except for people like Marcus Nel-Jamal Hamm. Hamm, a Black actor and professional wrestler, is what some might call an “anti-vaxxer,” though he finds that term derogatory and reductive. Since about 2013, he’s been running a Facebook page called “Over Vaccination Nation,” which now has more than 3,000 followers. One recent post is a video by the anti-vaccinationist Robert F. Kennedy Jr., wrongly suggesting that mercury-laced vaccines are shipped to predominantly Black communities. Hamm’s wariness of vaccines began when he took his son, who is now 10, to get vaccinated as a baby. He asked the pediatrician whether the boy could be exempted from the standard vaccine schedule because he has relatives with multiple sclerosis and autism. According to Hamm, the doctor treated him like a criminal just for asking. The experience left Hamm in a fog of unanswered questions: Do doctors have a quota of vaccines they have to fulfill? Why do some kids have bad reactions to vaccines? Is there something they’re not telling us? He started to distrust the accepted wisdom about vaccines, doubting that the official narrative is the true one. Today, Hamm believes the pharmaceutical industry is corrupt, and that it’s attempting to spin up a coronavirus vaccine too quickly. (The latter is a worry of the scientific community too, stoked by President Donald Trump’s ceaseless chatter about having a vaccine ready before Election Day—and the very name of the government’s vaccine project, Operation Warp Speed.) Though Hamm fears contracting COVID-19, when the coronavirus vaccine becomes available, he intends to avoid getting immunized. People like Hamm might be the missing piece to the puzzle of ending the pandemic for good. Developing a safe, effective coronavirus vaccine will be a monumental achievement, but it might not be enough. Encouraging people to actually get the vaccine might be the real battle, and people are even less predictable than viruses. If the coronavirus vaccine is 75 percent effective—which would be excellent, considering that the flu shot is only about 50 percent effective—roughly two-thirds of the population would need to be vaccinated, according to Paul Offit, the director of the Vaccine Education Center at the Children’s Hospital of Philadelphia. That number is enough to reach herd immunity—the level at which everyone is protected because there are not enough vulnerable people for the virus to pass between. [Read: A new understanding of herd immunity] Unfortunately, in some polls, far fewer than two-thirds of Americans say they are interested in getting a coronavirus vaccine. Though this number might change as we learn more about the vaccine’s effectiveness and side effects, at some points only about 50 percent of Americans have said they plan to get the vaccine when it becomes available. Some reports suggest that Facebook groups formerly dedicated to merely asking questions about vaccines have switched to more vociferous anti-vaccine views in recent months. Convincing people like Hamm that the vaccine is safe and effective will be a thorny and complicated task, for which experts say there is no one best approach. It’s something the United States government should start preparing for now—but isn’t. It’s hard to pin down just who, exactly, the vaccine-hesitant are. White adults are more likely to be vaccinated than Black adults are, perhaps because the latter have less access to medical care, and decades of maltreatment have eroded their trust in the medical establishment. Anti-vaccine groups have also targeted Black people. About a decade ago, anti-vaxxers in Minnesota invited the discredited researcher Andrew Wakefield, who falsely tied vaccines to autism, to give talks to the state’s Somali immigrant community. Vaccination rates among Somalis plummeted, and a few years later, the community suffered a large measles outbreak. Otherwise, experts told me, there’s a loose correlation between being Republican and questioning vaccines, and also between harboring vaccine skepticism and believing in conspiracy theories or having a lower level of education. But in general, vaccine skepticism spans from Goop-reading Californians to the ultra-Orthodox Jews of New York. In some ways, being anti-vaccine is a deeply American sentiment: It’s the stubborn belief that individuals know better than the government. Jennifer Reich, a sociologist at the University of Colorado Denver, views vaccine skepticism as an outgrowth of the societal push for people to take personal responsibility for their health. People are told “they should count their calories, count their steps, monitor their health,” she told me. Some people take it a notch further, deciding that they can train their bodies to fend off diseases without the help of vaccines. Vaccine-hesitant parents want to do everything exactly “right” for the health of their children, including personally choosing what substances are injected into them. Other vaccine-hesitant people, like Hamm, suspect that the pharmaceutical industry is in cahoots with doctors and the government, in a dark cycle of profit and secrecy. This fear of nefarious medicine is perhaps understandable in a world where drug companies actually did, through lies and greed, spark an opioid epidemic that has killed nearly half a million people. Vaccines are not actually very profitable for doctors, but the otherwise bafflingly opaque and extremely expensive health-care industry does not inspire confidence. Experts are divided as to whether it’s better to try to change anti-vaxxers’ minds about vaccines or to simply push them to get vaccinated anyway, without worrying about how they feel. Foremost among the strategies researchers have devised to break through misgivings about vaccination is, essentially, scaring people into doing it. In 2015, Zachary Horne, a psychology professor at Arizona State University, divided 315 participants into three groups. The first group read a story about a child who contracted measles; looked at a picture of a child with measles, mumps, or rubella; and read warnings about the importance of vaccination. The second simply read statistics showing there is no link between vaccination and autism. The third read about an unrelated topic. The group exposed to the vivid anecdotes were more likely to change their attitude toward vaccines than the other two. Vaccine skeptics often tell frightening personal stories of injury; Horne did the same thing, but for diseases. [Read: A vaccine reality check] This approach might prove effective when it comes to the COVID-19 vaccine. Americans tend to be more interested in personal security than the collective good, so emphasizing how the virus could harm you, specifically, could drive people to vaccination, experts told me. Doctors could, for example, show skeptics grim pictures of intubated patients or damaged lungs. In a similar study that came out last year, vaccine-hesitant college students were assigned to interview people who had vaccine-preventable diseases, such as polio. Afterward, nearly 70 percent of them became pro-vaccine. For those who are afraid of injecting unnatural substances into their bodies, some pediatricians and advocacy campaigns are trying to sell vaccines as a way for the body to mount a “natural immune response” to an unnatural invader. “Basically, we flip the logic on its head,” says Matt Motta, a political-science professor at Oklahoma State University. “You know what else is a foreign substance that enters the body and can potentially do harm? Diseases themselves. And vaccines are the single best way to prevent these violations of bodily sanctity.” In his own studies, Motta has found that for people who are concerned about contamination and uncleanliness—as many vaccine-hesitant people are—hearing measles symptoms described in depth leads to a 10 percent decrease in their acceptance of vaccine misinformation. In another study currently undergoing peer review, he found that reading messages emphasizing the personal and collective health consequences of not vaccinating slightly increased peoples’ intention to get the COVID-19 vaccine. But other experts say adjusting attitudes is a fruitless exercise. Some evidence shows that giving people —including the vaccine-hesitant—correct information actually causes them to double down on their resistance, in a psychological concept known as the “backfire effect.” In a study similar to Horne’s, another group of researchers found that images of sick children only worsened parents’ misperceptions about the vaccine-autism link, and did not boost their intent to vaccinate their children. Instead, this camp endorses a strategy called “direct behavior change.” Pediatricians might, for example, simply tell parents which vaccinations they’ll be performing during their child’s appointment, rather than ask them whether they’d like to vaccinate. According to research, parents are much more likely to avoid vaccinating if the pediatrician says something like, “What do you want to do about shots?” as opposed to, “Well, we have to do some shots.” Many schools already do a form of this by barring kids who haven’t received their childhood vaccinations. Once a coronavirus vaccine exists, some schools and workplaces will likely require it too. Other research-tested methods in this bucket are phone calls and postcards reminding parents to get their children vaccinated, especially if these reminders include the practice’s name. “Most people are open to vaccinating, and they just need to have the path to vaccination simplified,” says Noel Brewer, a health-behavior professor at the University of North Carolina. Direct behavior change is not foolproof, though. As Horne points out, the rise of “religious exemptions” to vaccine mandates show how parents try to get around vaccine rules. Before long, some denomination might claim that the coronavirus vaccine is offensive to their god. It might be worth listening to people who have already switched from the anti-vaccine to the pro-vaccine camp. For Kristen O’Meara, it happened in 2015, when her three young daughters came down with a brutal bout of rotavirus. The girls projectile-vomited and leaked diarrhea in their sleep. As they recovered, O’Meara had the sickening realization that there’s a vaccine for rotavirus. She picked up books by Offit and others, which extolled vaccines’ benefits. Eventually, she could formulate counterarguments to the points made by the anti-vaccine groups she was once part of. She thinks vaccine advocates should recognize that the vaccine-hesitant, like most people, want to be heard, not mocked. “It is not crazy to wonder about all these unpronounceable, scary-sounding ingredients that are in vaccines,” O’Meara told me. Their concerns should be addressed without implying, Oh, you’re just some nutball, crazy anti-vaxxer. [Read: Paging Dr. Hamblin: what if the vaccine works only half the time?] Toward the end of our conversation, I asked Hamm whether anything might reassure him about the safety of vaccines. “It needs to be unbiased, it needs to be apolitical, and come directly from the sources,” he responded. Herein lies the problem: Unbiased information on vaccine safety already exists. The Vaccine Education Center, where Offit works, is just one example. But Hamm dismissed these types of websites as “one-sheet pamphlets” and “cute pictures of a cartoon doctor giving a kid a shot.” Talking with him, I got the sense that converting the most hardened vaccine skeptics will take the kind of tireless public-education effort that U.S. officials have so far failed at during the pandemic. Despite ramping up vaccine production, the federal government has devoted scant resources to counteracting reluctance toward getting the COVID-19 vaccine, according to a recent report by a nationwide task force of epidemiologists and behavior specialists. Maybe Offit and his ilk could profile every child who has ever had side effects after a vaccine, and describe exactly how the symptoms were (or more likely were not) related to the immunization. Maybe a news site could walk laymen through every debunked vaccine-injury study, showing precisely why, down to the P values, they don’t show what vaccine skeptics think they show. Maybe doctors could take a cue from the measles studies and encourage people to imagine choking on a ventilator tube as their spouse videochats them in a hospital bed. Maybe they could do all of the above. As Motta told me, “you need to have lots of different strategies aimed at reaching lots of different people. And if you can move a couple of percentage points here and a couple of percentage points there, ultimately you put something together that gets us the herd immunity.” from https://ift.tt/3lYFO01 Check out http://natthash.tumblr.com Consider the cantaloupe. It’s a decent melon. If you, like me, are the sort who constantly mixes them up, cantaloupes are the orange ones, and honeydews are green. If you, like me, are old enough to remember vacations, you might have had them along with their cousin, watermelon, at a hotel’s breakfast buffet. Those spreads are not as bad as you remember, especially when it’s hot out; add a couple of cold bagels and a pat of unmelted butter and it’s a party. Maybe you want the cool, refreshing mildness of a melon cup at home. Unless there’s a good fruit stand nearby and cantaloupe is in season, that means taking a trip to the grocery store. Maybe you’ll stroll down aisles kept just cool enough to make the skin on your arms prickle. You’ll browse refrigerated produce shelves doused in cold water every so often. Then you’ll find it: the perfect cantaloupe. It’s round and rough, with no dimples or spots. When you thump it, there’s a satisfying, muffled thud. It’s a sweet one. Consider how the cantaloupe got there. It likely took a long ride to the supermarket or the hotel kitchen in a truck cooled to just above freezing. Maybe, like many melons, it was planted, picked, and packed on a plantation in the town of Choluteca, in southern Honduras, before it began its careful ballet of climate control. Workers told me they aren’t allowed phones in the fields in Choluteca, so they don’t always know exactly how hot it is. But during the growing season on the Fyffes melon plantation, temperatures hover in the mid-30s in Celsius—the mid-to-upper 90s in Fahrenheit. The sun broils the open spaces where workers chop the melons from their stems. The heat is overwhelming and omnipresent, an overseer whose hand is always heavy, and whose eye is never distracted. Workers have told me of conditions that push the human body to its limits—sometimes, past them. Protective gloves are prohibited, they say, so their hands bleed from the rough work handling plants that are doused in corrosive chemicals. Pickers say they are hesitant to show any signs of weakness or illness, fearing that taking time off or even appearing to be sick while working will result in termination. (A Fyffes spokesperson told me that gloves are always provided upon request, and are mandatory in certain parts of the packhouse where workers handle chemicals, and that unwell workers receive sick days and are required to see a doctor.) But the most common complaint is the most elemental: It’s damn hot in the fields. “El calor es bien fuerte,” one woman, 25, told me. She didn’t want to reveal her name for fear of retaliation, but she said she’s worked on a farm in Choluteca for four years, shuffling through almost every job available, from cleaning the facilities to picking the fruit. Many people who have worked for decades are marked by skin blemishes that, even if they’re not yet cancerous, aren’t all benign: hives, rashes, and chocolate-colored splotches. The spokesperson for Fyffes told me that the workers start very early in the morning to avoid the heat as much as possible, and are provided cold water and hats to shield them from the sun. But even for workers who begin in the dark, when sun and heat and exertion act together over long periods of time, the effects can be worrisome. “Varias mujeres se desmayan,” the same worker said. “Se les sube la presión … todo eso.” They faint. Their blood pressure spikes. And they keep working. [Read: Introducing Atlantic Planet] Thousands of miles separate the fields of Honduras and the continental breakfasts in the States. But these are terminals of a single, continuous system. Heat bears down most on the global working poor and developing countries, while their wealthier planetmates are able to evade the worst of the warming. What’s more, consumption by those wealthier folks helps create the warming, which in turn robs the poor of opportunity and walls off economic mobility. Garment workers in Cambodia and Bangladesh toil in sweatshops to sew the moisture-wicking fabrics that make summer in Phoenix or Miami or Washington, D.C., bearable. In Qatar, itinerant workers labor at the outer edge of human survivability to fabricate air-conditioned hotels, malls, and arenas for the rich. And thousands of families flee environmental pressures in Central America only to find themselves suffering from the heat in the United States. Scientists and people with good sense around the world recognize the manifold perils of a climate crisis: an onslaught of tropical systems in the Atlantic Ocean, the relentless burn of wildfires in California and Oregon, the hundred-year floods that now encroach annually. Less appreciated, perhaps, are the direct effects of that increasing warmth on human bodies and communities. Heat is already often deadly, and even below fatal thresholds it is a grinding attrition that saps personal and economic vitality a little more each day. In the coming century, when wealth inequality will likely increase and the spaces where humans can live comfortably will shrink, the heat gap between rich and poor might be the world’s most daunting challenge. It will reflect existing wealth disparities, but will also deepen them. It will destroy some bodies, while others are spared. It will spark uprisings and set the stage for conflict, both between and within nations. In a hot world, the heat gap will be a defining manifestation of inequality. 
One billion people work in agriculture, performing the same kind of labor as the melon pickers in Choluteca. Add to that the millions and millions of people who work outdoors in construction jobs, or indoors in sweatshops and factories without air-conditioning, and significant numbers of low-income workers--including hundreds of millions of children—have little control over the temperatures in which they spend the majority of their waking hours. According to a recent report by the United Nations’ International Labour Organization (ILO), heat stress is threatening their work and their lives. Heat stress—defined by the ILO as “heat received in excess of that which the body can tolerate without physiological impairment”—has always affected workers in the summer and in tropical or subtropical climates. Sunburns, skin cancer, heat exhaustion, fainting, dehydration, and long-term kidney problems have been accepted as basic risks of outdoor work. But as the Earth has experienced a sustained, record-breaking run of overall temperatures, these problems have become more and more of a burden—and, more and more often, a fatal one. Tord Kjellstrom, an environmental- and occupational-health expert and one of the main authors of the ILO report, told me that “it’s well understood from a physiological, medical point of view that these hot temperatures limit people’s abilities to carry out work.” It’s not just work—extreme heat can disrupt or destroy many of the pieces of a healthy life—but in his research, Kjellstrom has found productivity to be one of the main proxies for all the ways heat can affect the global poor. Kjellstrom’s work has zeroed in on so-called mass fainting events in South Asian and Southeast Asian factories over the past decade. In 2017, hundreds of garment workers in Bangladesh fell ill with what one worker described as “nausea, vomiting and stomach pain after working [a] few hours.” That same year, “there were more than 1600 cases of factory workers in Cambodia fainting in various incidents,” according to an epidemiological study of the faintings. Over and over, these incidents have been described as “mysterious.” One common explanation is possession by spirits. The usual official line is that mass fainting—among a mostly female workforce—is caused by “hysteria” of an inexplicable, gendered extraction. A secret report by officials in Cambodia after two such mass fainting events found its way to Kjellstrom. “Their report was quite long, and half of it was about the heat problems,” he told me. “And still, at the end they concluded that it was hysteria: You know, one young woman in the factory, she faints, and then all her friends start fainting as well. And of course that doesn’t make sense.” Epidemiological evidence also points to stress, air pollution, long hours, and the punishing pace of work as potential contributors to the fainting incidents, but with factory temperatures in Cambodia regularly topping 100 degrees Fahrenheit, the likely main contributor seems obvious. [Read: Beyond climate denial and despair] Other places have caught Kjellstrom’s eye as well. In Qatar, where the stadiums the emirate is scrambling to build for the 2022 World Cup require lots and lots of outdoor labor, heart-disease deaths among workers have spiked during the summer months. Chronic kidney disease has swept Central America; again, the etiology of the epidemic has been described as mysterious. Similar waves of kidney disease have been observed in India and Sri Lanka. Scientists have tended toward a kitchen-sink explanation, identifying genetics, diet, pollution, and age as contributors to the epidemic. But a common factor in each outbreak—and the one that has increased most dramatically in recent years—is the heat. One way to track the increasing impact of heat on people has been to measure how much it affects working hours, because workers naturally take more breaks and perform jobs more slowly when enduring dangerous levels of heat. The ILO report projects that 2.2 percent of total working hours worldwide will be lost to high temperatures, with the greatest predicted losses coming in the developing world, by 2030. And while the productivity losses in those places are a major concern for development trajectories and population-level wealth, they also mean lost wages, more unstable work situations, and more pressure to work in those unstable conditions. The places with the most exploitative labor conditions and the steepest poverty rates also face the largest burdens from a changing climate, which then are absorbed mostly by poor people, thus reducing their mobility and economic welfare further. 
Women and the elderly are both overrepresented in the workforce and face unique health hazards from heat stress. “They are in jobs that cannot be air-conditioned easily or replaced by mechanization,” Kjellstrom said. “Of course, these are the people who are usually the lowest-paid and the most vulnerable in a socioeconomic sense. So as the heat affects them further and further, while at the other end, rich people sit in air-conditioned offices, then it will definitely be a reason for increased inequality.” At both the population and the individual levels, heat and poverty are something of an ouroboros, a cycle that wealthy people and countries perpetuate via emissions, but themselves are able to escape by way of air-conditioning, indoor work, and social and geographic mobility. It might follow that people stuck on the receiving end of the heat gap would do their best to move to the other end. This happens, to some extent. The ILO found that “heat stress is increasingly becoming a driver of international migration.” Climate migration today is a dramatic new chapter in an ancient story—much of human migration in history has been, in some sense, climate-driven. But in the places where the heat gap already operates the most aggressively, leaving might not be an option. Moving is hard and costly; moving when you need a new kidney can be physically impossible. For those who are able to move, no land is promised. Millions of people have left Central America and Mexico in the face of rising temperatures, droughts, and crop failures. But as migrants have moved northward, heat stress has followed. That’s especially true in places like California and Florida, where farmwork has always involved a good deal of exposure to high temperatures. Jeannie Economos, a coordinator for the Pesticide Safety and Environment Health Project within the Farmworker Association of Florida, has been organizing and assisting workers in fields and on farms for a long time. Farmwork in Florida has always been hot, often dangerously so, and she’s always counted the heat as an issue. But the current climate moment is something else. “I’ve been here since 1961, and this feels different,” Economos told me. “There’s a different quality to the heat. It used to be scorching, but now it feels like it’s searing.” The science backs her up. Florida is definitely hotter now than it was a century ago, and the situation is accelerating. A report from the Union of Concerned Scientists, an advocacy group, found that a combination of rising temperatures and humidity could make a third of every year across the state dangerously hot for human bodies within the century. A few weeks’ worth of days every year already meet that threshold. The Florida heat and sun exposure take a toll on all the farmworkers Economos encounters. Surprisingly, she worries most about a group that typically works indoors: the people who grow ferns and ornamental plants, propagating and tending and picking year-round so that poinsettias will be ready for Christmas, and fern fronds will be available for Valentine’s Day bouquets. Towns like Pierson, Florida—the “fern capital of the world”—are dotted with ferneries. Ferns tend to prefer shade, so they are grown either under wide mesh canopies or in enclosed greenhouses. But although these places are shaded, the conditions that are good for growing ferns are bad for people: incredibly humid, and often lacking wind or ventilation. They are “brutally hot,” as Economos said. And to keep their clothes from being soaked by the wet plants and moist air, pickers often wrap themselves in black garbage bags, trapping the heat even closer to their bodies. [Read: How bad are gas stoves, really?] Economos has been involved in several efforts to study what the increasing heat actually does to people. One longitudinal study of 252 agricultural workers conducted with Emory University researchers found that those employed in the Pierson ferneries experienced an average heat index of 101 degrees Fahrenheit over the course of the study, a level that the National Weather Service says necessitates “extreme caution”; heatstroke or exhaustion is possible with prolonged activity. With this kind of everyday, year-round exposure to dangerous heat, damage to the body is virtually certain. In 2018, Economos’s research team found significant evidence of acute kidney injuries related to dehydration among Pierson fern harvesters, a correlation that grew stronger as the heat index increased. In essence, the “mysterious” kidney disease in Central America is now striking farmworkers in the United States. 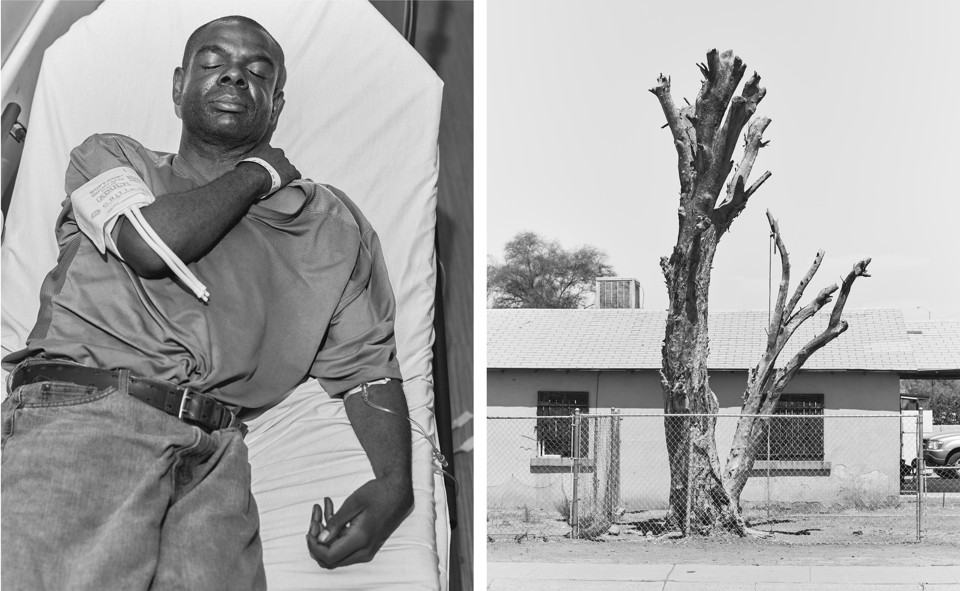
Across Florida, organizations advocating for immigrant communities are scrambling to confront this problem. Oscar Londoño, the executive director of WeCount!, a workers’ center in Miami-Dade County, says the organization has had to get up to speed on heat quickly. A few years ago, “we began seeing a lot of members that were reporting issues at their workplace,” Londoño told me. Most of those members were day laborers, farmworkers, or plant-nursery harvesters, many of them in workplaces or informal roles that don’t require breaks after heat indices reach a certain level, or other protections. “Many of the employers aren’t providing these protections voluntarily,” Londoño said. WeCount! has pushed for legislation in Florida that would mandate more stringent heat protections. While it waits for government intervention, it is using its Spanish-and-indigenous-language radio program, Radio Poder, to run public-service announcements about the dangers of heat. The ads tell workers to drink water, seek shade, and rest when they can. Translated from Spanish, one ad warns that “this summer is one of the hottest in history.” What it doesn’t say is that this summer will likely be remembered as a pretty mild one in our near future. 
F or millennia, humans have lived within a slender range of temperatures. According to a study published in the Proceedings of the National Academy of Sciences of the United States of America (PNAS) in May, most people born in the past 6,000 years have lived in places with average annual temperatures of about 11 to 15 degrees Celsius, or 52 to 59 degrees Fahrenheit. (The major band of historical population densities above 20 degrees Celsius is in the Indian monsoon region, where the annual rains are the main lifeline making human thriving possible.) The places where humans live have gotten slightly warmer in those thousands of years, but they’ve done so gradually, giving people time to adapt and move. But, thanks to human-driven global warming, that sliver of global society-friendly temperatures is due to shift more in the next 50 years than it ever did in centuries prior. The May PNAS study found that in the worst-case climate scenario—where emissions continue to rise and the global average temperature increases by 2 degrees Celsius—the average annual temperature experienced by people in 2070 will hover around 20 degrees Celsius (68 Fahrenheit), with most people living in a range of temperatures between 18 and 22 degrees Celsius, or 64 and 71 degrees Fahrenheit. Population growth is expected to be highest in the hottest places; according to PNAS’s projection, by 2070 more than 3 billion people will be regularly exposed to temperatures that are not typically found outside the Sahara Desert today. Average annual temperatures, however, tell only part of the story. The real medical danger from heat usually comes from summer heat waves. By most accounts, including an article published in Nature this summer, extreme heat waves have increased in frequency, duration, and intensity over the past five decades. A 2019 Nature article produced a startling finding: Under the same 2-degrees-Celsius scenario as above, and assuming ever-deepening global inequality, the kinds of extreme heat waves that now happen only twice in a millennium, on average, will become events that happen multiple times each decade for billions of people by 2075. Under each possible climate scenario, poor areas will be most affected. The 2019 Nature study predicts that even if global governments can curb emissions enough to limit warming to 1.5 degrees Celsius instead of 2 degrees, the poorest countries will still face more additional risk from heat waves than the wealthiest countries would face with the full, catastrophic 2-degree increase. In short, people in countries like Nigeria, Ethiopia, and Haiti will see a greater total increase in heat waves under the more optimistic global climate scenario than the average U.S. citizen will under the worst possible runaway global-warming crisis we can imagine. But these climate effects don’t just highlight differences among countries. Regional differences in heat exposure over the next century will also exacerbate differences in wealth within national borders. As my colleague Robinson Meyer has reported, while the convulsions and pressures of climate change are projected to squeeze the total gross domestic product of the United States by the end of the century, a closer look by researchers found that the majority of the losses will be accrued by counties in the South. The counties most affected are, on average, poorer than the counties that appear to fare well. Indeed, while several counties in the Deep South are predicted to lose a fifth or more of their GDP, some counties in the Pacific Northwest and New England might actually see their economies grow. Deaths caused by climate change will likely be clustered in the southernmost third of the country. While the model considers several different climate-change-related problems, it’s clear that the main driver of the inequality within regions will be heat itself. There is compelling evidence that the heat gap operates on an even more local level. In 2019, an NPR investigation found that in the majority of the 97 American cities analyzed, poor neighborhoods tend to be hotter than wealthy neighborhoods. Much of this disparity has to do with what’s called “urban heat-island effect,” whereby the asphalt, building materials, and reflective surfaces that dominate denser, poorer neighborhoods tend to absorb sunlight and trap and amplify ambient heat. Another factor is the extreme disparity in green space between rich and poor neighborhoods. Wealthy neighborhoods and single-family dwellings are much more likely to have tree cover and other forms of vegetation that cool places off by creating shade and modifying airflow. 
A recent New York Times article corroborates these findings, but with an alarming addendum: The disparities also seem to track closely with historical patterns of residential racial discrimination. “In cities like Baltimore, Dallas, Denver, Miami, Portland and New York, neighborhoods that are poorer and have more residents of color can be 5 to 20 degrees Fahrenheit hotter in summer than wealthier, whiter parts of the same city,” write Brad Plumer and Nadja Popovich. The hottest spots can be linked to areas that were redlined decades ago by the federal government. Black and Latino families did not simply passively settle in the hottest, most uncomfortable neighborhoods. They were placed there, and then the same white voters and leaders who placed them there turned up the thermostat even more with carbon emissions and local zoning policies. The consequences of this increasing burden on poor communities of color are already apparent. Life on urban heat islands is associated with higher mortality from heat waves. Studies have consistently found links between poor maternal and child health outcomes and extreme temperatures, and emerging evidence suggests that the effects of heat are most damaging for Black, Latino, and Indigenous infants and mothers. A meta-analysis published in JAMA in June found a “statistically significant association between heat, ozone, or fine particulate matter and adverse pregnancy outcomes,” including preterm birth, low birth weight, and stillbirth. And the NPR investigation of heat in poor neighborhoods found that over five years, “Medicaid patients in Baltimore's hottest areas visited the hospital at higher rates than Medicaid patients in the city’s coolest areas. The low-income patients in the city’s hot spots visited more often with several conditions, including asthma, COPD and heart disease.” When Americans think about climate change, they probably don’t have these kinds of consequences in mind—an uptick in stillbirths, or more Black children with asthma. Climate communication often tends toward the apocalyptic and the episodic, for good reason: Dramatic events are a good way to get apathetic people to care. But the destruction wrought by the heat gap in American neighborhoods is just as important as the high-profile cataclysms. That destruction is insidious and hard to follow because it plays out along existing lines of inequality and injustice. Comparable to its role in some chemical reactions, heat accelerates the logical outcomes of unequal human systems. In this reaction, heat is not necessarily a bomb that will suddenly vaporize civilizations. Here, its preferred pathway is decomposition, working slowly and steadily at severing bonds until two components are separate, if not equal. 
Almost 5,000 people were arrested in the streets on June 2, the height of turmoil in a summer of uprisings. That day, as protests over the killing of George Floyd by Minneapolis police entered their second week, the temperature in Minneapolis hit 90 degrees Fahrenheit, about 12 degrees above average. The same day, as protesters in Louisville, Kentucky, prepared to commemorate what should have been Breonna Taylor’s birthday, the temperature also approached 90. As opponents of white supremacy engaged in some of the most widespread, sustained protests in American history, the country also headed toward one of its hottest summers ever. The devastating fire season that would reduce much of the West to cinders was about to begin. Almost 2 million Americans had contracted COVID-19. More than 100,000 had already died. The heat was not just part of the setting. The coronavirus pandemic and the summer of protest have both been propelled by vulnerabilities that heat and inequality create. In the case of the pandemic, long-term climate change is not incidental to the progress of a novel coronavirus from bats to people: As my colleague Ed Yong has written, climate change is one of the key elements that pushes zoonotic diseases like COVID-19 from wild spaces into human populations. “Through intensive agriculture, habitat destruction, and rising temperatures, we have uprooted the planet’s animals, forcing them into new and narrower ranges that are on our own doorsteps,” Yong says. In considering the role of potential comorbidities in the pandemic, heat is not ancillary either. It might worsen asthma and other pulmonary diseases, and it definitely influences kidney disease and hypertension--two risk factors for complications from COVID-19. Before George Floyd lost consciousness with officer Derek Chauvin’s knee on his neck, he had, according to the county medical examiner’s autopsy, contracted the coronavirus, and developed some level of heart disease and hypertension. The medical examiner named heart failure the official cause of death. For some, the report served to shift blame away from the officer in a way reminiscent of the response to Eric Garner’s death in 2014, when Garner’s history of asthma and heart disease was used to minimize the culpability of the officer who put him in a chokehold. But there’s another way to think about how those risk factors really operate. Unequal exposure to heat and pollution weakens Black people’s bodies. That exposure consistently assaults Black folks’ hearts, lungs, kidneys, and blood vessels. It makes them more vulnerable to mortality from all causes, including targeted brutality from police. And so, just as protests against incidents of police brutality have also expanded their scope to denounce the bigger picture of systemic white supremacy, mass incarceration, and other necessary conditions for police violence, the heat gap should also be understood as a part in the whole of injustice. Several other protest movements in our pandemic summer also sprang from heat-induced inequality. Lockdowns and shelter-in-place orders forced many families “to choose between cooling their homes and paying for necessities such as food, medicine, and child care,” according to the Center for American Progress. People with low incomes are less likely to have air-conditioning in their homes than wealthier people, and tend to pay more per square foot when they do have it, because their homes are less energy-efficient. And after lockdowns and pandemic-influenced contraction erased entire sectors’ worth of blue-collar jobs, even families that otherwise would have had no problem cooling their homes have faced utility shutoffs—or worse, evictions—because of lost incomes. In Miami, activists fought this summer to try to keep the local utility companies from shutting off power to people who couldn’t pay after losing their jobs. Cheryl Holder, a faculty member at the Herbert Wertheim College of Medicine at Florida International University, regularly treats undocumented immigrants and other workers who are most at risk. “I have folks now who have air-conditioning, but they can’t afford to run it,” Holder told me. She says that among her patients, while pandemic-related pauses in work have eased some of the onslaught of kidney damage, people have still faced serious risks from staying home. In the places and times that used to provide relief for workers, now there is less to be found. “People have worked in the heat forever,” Holder said. “But they’ve relied on respite during cool nights. There are fewer and fewer cool nights. More hot nights.” As a co-chair of the advocacy group Florida Clinicians for Climate Action, Holder has given serious thought to figuring out how to break the bond between heat stress and poverty. The pandemic has accelerated her inquiry. “How do we get our infrastructure to support good health?” she asked. She’s got a laundry list of things that obviously might help. Adding green space and shade in working-class and poor communities, providing more water and more breaks on the job, providing more access to public cooling centers, and providing both affordable air-conditioning and efficiency upgrades for poor homes are all important bullet points on that list. The main barrier she encounters is an eternally vexing one for people with any kind of imagination: “Who’s going to help pay the bills?” 
In a TED Talk she delivered earlier this year, Holder outlined her own theory of how climate change and poverty were linked. “Poor, vulnerable people are already feeling the effects of climate change,” she said. “They are the proverbial canary in a coal mine. Truly, their experiences are like oracles or prophecies.” This view of climate justice transforms the dominant narrative of climate change from one of a shared experience of gradual challenges into one where poor people, women, and minorities are on the front lines, serving as a vanguard against oblivion. In the end, everything comes down to a handful of considerations. Poor people—and those otherwise marginalized by way of race, class, caste, or gender—are more likely to live in hot places and do jobs in the heat. And the people who generated most of the emissions making those places and jobs hotter are likely to be wealthier, living in conditions that shelter them from the heat. This is true on every level: Developed countries have emitted the lion’s share of the carbon that got us into this mess in the first place. According to Oxfam and the Stockholm Environment Institute, even as rapid industrialization has brought more intermediate and developing economies into the fold of powerhouse emitters, the wealthiest 1 percent of the global population has been responsible for twice as much carbon output as the poorest half. And in America, the individual carbon footprint of high-income homes is significantly higher than that of poor ones. The climate catastrophe might one day be so overwhelming that the ordeals of poor people and racial minorities become predictive in some way for the experiences of the elite. But maybe they aren’t really the canaries in the climate-change coal mine. Maybe they are the victims of a massive, global wealth transfer that affects almost every facet of life in a warming world, and will continue to do so well into the future. The people on the margins of society assume an unwanted role as buffers—absorbing the climate risks that the rest of the world has created and now shirks. Following melons and pickers from the fields in Honduras on their journey north and witnessing epidemics of kidney failure migrate with them, this dynamic is in clear view. On some level, this is not surprising. The climate has always had a hand in the fate of societies, and climate pressures have always animated global conflict and class division. Yet generations of humanity have now been born into a world where the global totality of those climate pressures is directly controlled not by God nor by random gradients in the atmosphere, but by a small, insular cadre of humans. Perhaps it is true that recent history has all been a grand game played by elites, with the lives of everyone else in the balance. But now, in the climate crisis, the spaces on the board, the rules of the game, and the moves available cannot be hidden. In the past century, the American liberal order has celebrated advancements in racial and gender equality and the proliferation of civil and human rights. The country defeated malaria in the swamps of the South and fought back against the kind of hunger that once starved people in city slums. In the age of carbon, global life expectancy has increased steadily, abject poverty is abating in some places, and there has never been a safer era in human history to have a baby. But heat presents a challenge to every single advance in health and medicine. It aids the spread of infectious diseases and makes chronic diseases worse. Heat might be reversing precious gains in infant and maternal mortality. And it’s creating new economic burdens on the global poor. All while the better-off folks crank up their air conditioners and travel in cars to climate-controlled white-collar jobs, where they stream data from servers kept chilled in massive, power-sucking farms. We have a long, hot century ahead of us. Human civilization will face threats and challenges that seem beyond the scope of our imagination, and definitely lie beyond the scope of our experience. As it turns out, humanity is familiar with the enemy it faces. That nemesis may now come heralded by “bomb cyclones” and mega-droughts, but a peek beneath its smog shroud reveals its true nature. The enemy is human-engineered inequality, as powerful—and as vulnerable—as it has always been. from https://ift.tt/3k0PV3z Check out http://natthash.tumblr.com
Dear Dr. Hamblin, My daughter is part of an accomplished high-school woodwind quintet. For two years, they practiced constantly and participated in competitions, becoming one of the best in the state. But the shutdowns in March put an end to it. They haven’t played together at all since. The group wants to start practicing again, and one of the parents volunteered to have them play in their backyard. My family has health conditions, so we have been very cautious about the pandemic. Would it be safe for her to play outdoors with her classmates? Shannon Chapman Henderson, Nevada At first glance, it clearly doesn’t sound ideal: blowing forcefully through a woodwind instrument in close proximity to other people who are also blowing forcefully through woodwind instruments. Given what we’ve learned about how singing and even talking loudly can increase the amount of coronavirus in the air, a quintet could seem ill-advised. But the danger of music is all in how you make it. I would let your daughter start practicing again. Although there are no clearly documented cases of coronavirus transmission via woodwind, there is a lot of evidence of the benefit of kids studying musical instruments, and taking part in team-based competition. Even during a pandemic, immersing kids in the arts isn’t an indulgence. It should be a top priority, right alongside that of opening schools. Playing an instrument is not absolutely risk-free, but if you keep a few things in mind, it could be close. As with pretty much every other activity right now, having the quintet gather outdoors is a great idea. If any neighbors complain, explain that the backyard practices are part of a global effort to keep them from dying. If anyone happens to be infected, any virus that emanates in the heat of performance will likely fade into the sky and disperse like the music itself. Indoors, as any parent of a child who’s learning an instrument knows, everything is trapped and can echo around the room indefinitely. [Read: When will it be safe of to sing together?] Some instruments do seem to pose more risk than others. Obviously, string instruments can be played without even opening your mouth, but it sounds like your daughter’s quintet is too far along to take kindly to a suggestion that they all learn new instruments. Because the virus is sent into the air by talking, coughing, and singing—any forcible exhalation of air through the pharynx—playing a woodwind or brass instrument would logically pose a risk. These instruments are effectively designed to amplify what’s coming out of our mouths and to carry the sound. A 2011 study of vuvuzelas (the long, straight plastic horns that people blow at soccer games) found that their capacity for spreading infections could be tremendous. Compared with shouting, blowing through the horn sent several hundred times more particles into the air. Thankfully for everyone, kids don’t train for vuvuzela quintets. Woodwind and brass instruments send air through a maze of twists and turns, and buttons create turbulent airflow patterns that don’t simply shoot everything out in a piercing plume. Breathing into a convoluted contraption such as a saxophone or a tuba, then, actually serves as a sort of filter that collects the larger droplets you might be spewing out. This is familiar to anyone who has emptied a spit valve and seen what pours out. The real question is the potential danger of smaller, aerosolized particles that can blast out of an instrument and linger in the air. In May, the Vienna Philharmonic reported that it had conducted a study of the aerosols from various instruments. Researchers hooked tubes up to musicians’ noses, and as they played, they inhaled an aerosolized salt solution that could be visualized when it was exhaled. The researchers mapped the clouds of air around musicians while they were playing and reported that none of the instruments sent respiratory droplets beyond the commonly recommended radius of six feet. In most cases, no significant amount of the aerosolized salt particles were detectable coming out the end of the wind and brass instruments. Flutes were the worst offender, passing a “large amount” of aerosol in a cloud covering two and a half feet. In July, another study in Germany offered findings and hope similar to those from Vienna. But neither study measured actual coronavirus particles, and the overall evidence is still thin. Doctors at the University of Iowa have expressed concern about the rigor of both findings, given that they weren’t peer-reviewed, and raised additional variables that the research failed to take into consideration: “Wind players buzz on their mouthpieces, blow out tone holes, blow out spit valves, clean their instruments with swabs and feathers, and might have leaking embouchures or nasal emissions during playing,” they wrote. “How to mitigate these risks is not yet known.” Ultimately, the risk posed by playing a woodwind instrument should fall somewhere between talking softly and aiming a vuvuzela at someone’s face. This is a wide range, but much can be done to ensure that you’re closer to the former. Preliminary guidelines issued by a coalition of performing-arts organizations currently recommend that all musicians presume that aerosols are coming from the keyholes and bells of their instruments, and that everyone should use bell covers—or, in the case of flutes, “flute socks”—which are like masks for your instruments. They’re not ideal for sound quality, but they’re great for practice. Musicians should also wear masks with slits to insert the mouthpiece. And while playing, they should face in the same direction, to avoid sending woodwind emissions into anyone else’s face. [Read: How we survive the winter] Every musician should have a six-foot radius when outdoors. As it gets colder and the kids want to practice indoors, there will be new challenges: The six-foot rule isn’t sufficient when people are in an enclosed space with little ventilation. Airborne transmission isn’t a problem that can be solved with plexiglass, either. In fact, it might create ventilation “dead zones.” The larger and better-ventilated the space, the safer. All of the standard advice applies: Open windows, use HEPA air filters, and limit the time of exposure. The guidelines suggest that indoor rehearsals should last no more than 30 minutes, followed by 20 minutes to let the air in the room turn over. Even though a woodwind quintet isn’t an ideal pandemic scenario, the opportunity for these kids to learn and develop artistically and socially is too great to abandon. The goal should be to find a way to come as close as possible to the old ways of practicing and playing music while avoiding any major or unnecessary risk. A little conscientiousness will go a long way. Good luck to the quintet. I hope they destroy the competition. “Paging Dr. Hamblin” is for informational purposes only, does not constitute medical advice, and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. By submitting a letter, you are agreeing to let The Atlantic use it—in part or in full—and we may edit it for length and/or clarity. from https://ift.tt/2SV1cqc Check out http://natthash.tumblr.com For months now, Americans have been told that if we want to socialize, the safest way to do it is outdoors, the better to disperse the droplets that spew from our mouths whenever we do anything but silently purchase grapefruit. But in many parts of the country, this is the last month that the weather will allow people to spend more than a few minutes outside comfortably. And next month, America will celebrate a holiday that is marked by being inside together and eating while talking loudly to old people. Federal and local officials have offered little guidance on whether and how people should be socializing this winter. That has left even medical experts confused about what’s safe, and what’s not. About a month ago, Megan Ranney, an emergency physician who teaches at Brown University, was trying to decide whether to take her son to his favorite restaurant for his ninth birthday. The family has not dined out since the pandemic hit the U.S. But Ranney’s son really, really wanted to go. “And I was trying to think in my brain, Is it safe for us to go outside? What if we're inside and we're in a private room?” Ranney told me. “It's just, it's too complicated to figure it out on your own.” No indoor gathering will be perfectly safe. Although many states have allowed indoor public settings such as gyms and restaurants to reopen at least in some capacity, experts don’t recommend spending a lot of time indoors with others, especially in situations where masking isn’t possible. The odds of catching coronavirus are about 20 times higher indoors, and private, indoor gatherings have been linked to several coronavirus outbreaks. In June, a surprise birthday party in Texas resulted in 18 coronavirus cases. In July, a house party in Michigan led to 43 cases, and a family gathering in North Carolina led to 40 cases because the attendees “went about their daily lives” before they started showing symptoms. In some places, in-home gatherings are now responsible for the majority of new coronavirus cases. A recent CDC report showed how a chain of family gatherings in Chicago led to three deaths. But it’s unrealistic to expect Americans to stay inside all winter without seeing anyone. Even if people could do that without going batty, it’s likely that, with January feeling endless and no stay-at-home order in place, people will take their chances. “Making a rule that says zero indoor gatherings until we have a vaccine is totally impractical,” says Julia Marcus, an infectious-disease epidemiologist at Harvard Medical School. In the absence of such a rule, “we have a mishmash of risk communication and guidelines from different entities,” Marcus told me, “and people are continuing to muddle through. It’s funny, because now I’m sitting here thinking, What are the rules in my city? I actually don’t know.” [ Read: America’s Terrible Internet Is Making Quarantine Worse ] Beyond “stay at home” and “it’s okay to go out now,” government officials aren’t explaining the relative risks clearly and widely enough for everyone to understand. Ever since states publicized their “reopenings,” some people have only seen unrelated people from a six-foot distance and outside. Others are throwing indoor weddings. Often, these people live in the same city. Given this information vacuum, researchers like Ranney and some public-health workers have launched their own efforts to help people decide what types of social activities are safe, based on where they live. In a few phone calls, I too was able to figure out whether socializing indoors is okay. But not everyone is a health reporter. Here’s what to consider before you host that dinner party inside your dining room on a nippy October day: If you make it small, and primarily comprising people under 60, that’s safer. If your guests can stay six feet apart, even better—though consider that this is not likely to happen once they have had a few glasses of wine and the board games come out. Perhaps the most important factor is the level of so-called community transmission: how many new COVID-19 cases are in your immediate area. Caitlin Rivers, an assistant professor at the Johns Hopkins Bloomberg School of Public Health, told me she wouldn’t be comfortable at an indoor dinner party right now, no matter what. But if you were going to risk it, it’s safer in areas that are seeing only 5 to 10 new cases a day per 100,000 people, and have a test-positivity rate less than 5 percent. Tom Tsai, a health-policy professor at Harvard, puts this number slightly higher, at 25 cases per 100,000. But this community transmission number is hard for most people to keep track of. Part of the problem is that Americans no longer have a centralized source for news. Though interest in TV news has picked up recently, the three major evening newscasts get only about half the viewers today that they did in the 1980s. Some newspapers run transmission numbers on their front pages, but many Americans live in news deserts, and only 29 percent of Americans get a newspaper either digitally or in print. People tend to get news from social media, which will often circulate stories of national interest but not, say, the case numbers in a given county. Health departments can post things on social media, but how many people follow their local health department on Facebook? Rivers told me that to find the community transmission rate and other information, people should be checking their local public-health department’s website. But after more than a decade of severe budget cuts, many health departments don’t have the money to make snazzy, user-friendly websites with constantly updating figures. For instance, Wisconsin is currently erupting into a COVID-19 hot spot, and one county, La Crosse, had 41 cases per 100,000 people as of this writing—four times the rate Rivers said is safe for indoor gatherings. But La Crosse County’s health-department website is rudimentary, offering a link to a separate COVID website in a small font. That site says, “Personal social gatherings are not recommended,” and that the “new case rate” is 97, with a red arrow pointing up. A layman in La Crosse County is unlikely to know the meaning of this rate. Another Wisconsin county, Kewaunee, which also had 123 new cases per 100,000 people, has a health-department website on which the number of cases is not displayed anywhere. (In a response to a request for comment, the Kewaunee County Public Health Department said it posts its total number of coronavirus cases on the county website. In an email, Maggie Smith, a health educator with the La Crosse County health department, said, “As a public health department, we are limited in both funds and capacity and rely heavily on free and low cost tools to support our communication efforts.” Smith added that the department has used Facebook, Instagram, and local celebrities in its outreach.) “A lot of local health departments in the United States don’t even have an epidemiologist,” says Albert Ko, a professor at the Yale School of Public Health. “When a local health department doesn’t have the capacity to use 21st-century technology to disseminate important public-health information, that’s a real challenge. And that’s what puts us behind other countries that have had successful responses.” There are a number of websites that show the levels of community transmission by county, such as one Tsai worked on, at GlobalEpidemics.org, but they are not widely known among the general public. (According to this map, in the county where I live, for example, it would be safe to gather indoors according to Rivers’s standards, because there are only eight new cases a day per 100,000 people. But in my parents’ county in Texas, which has just over 10 cases, it would be less safe.) To check these types of websites, “you have to be interested,” says Tara Kirk Sell, a senior scholar at the Johns Hopkins Center for Health Security. “And if you're already someone who thinks this is important, and you’re checking out your numbers of cases per 100,000,” you’re probably already doing all the right things when it comes to social distancing. Some health departments are stepping up their communications, holding Facebook Live events and press conferences in which they urge people to avoid indoor gatherings. The Kansas City, Missouri, health department has produced videos showing how easily coronavirus spreads. (Still, illustrating the limits of social media, the first reply to a tweet with one of its videos is: “Masks don’t do anything.”) In Chicago, the public-health department has developed a tool that can help people decide whether a gathering is safe through questions such as “Is everyone healthy?” and “Can you always keep a 6-foot distance?” Commissioner Allison Arwady has also been hosting regular Facebook Lives in which she answers questions from the public, and she hosts a weekly press conference in which she often highlights stories of individuals who caught coronavirus at a small gathering. She’s running focus groups with Black and Latino Chicagoans to test messages that might resonate with them. But, she acknowledges, not every health department has the money or manpower to do all this. Together with her colleagues at Brown, Ranney has developed a free app called My COVID Risk that will allow users to input the type of activity they want to do, whether it’s indoors or outdoors, how many people will be there, what protective measures they’ll take, and where they live, along with other factors. The app will then generate a relative risk of catching coronavirus at that activity—from “very low” to “very high”—using community-level data from The New York Times’s coronavirus map. People can modify their risk level by reducing the number of people, for example, or adding a mask requirement. “Given the lack of clear national guidelines on what's safe and not safe, our hope is that this will fill a void for the average American who's really struggling to judge the safety of various activities,” Ranney told me. Still, Ranney says, this app is the kind of thing the federal government really should have developed by now. It’s odd that in a wealthy, industrialized country, a random researcher is the one designing a tool to keep citizens safe from public-health threats, using data she scraped from a newspaper. These efforts are commendable, but experts agree that they should be publicized by officials at the federal level, so that all Americans know how to find and use them. Some have even advocated for a national system of COVID-19 risk levels that could tell Americans when it’s safe to, say, visit with friends outside, versus shelter in place, versus live normally. In response to a request for comment, a spokesperson from the U.S. Department of Health and Human Services said, the agency “consistently educates the public on the three W’s, advising Americans to: Watch your distance, Wear a mask when you can’t watch your distance, and Wash your hands.” Sell says the government should team public-health departments up with influencers, faith leaders, and celebrities to make people aware of how to gauge the risk of indoor gatherings, before it’s too late. “Public health can make a message, but we want people to hear it,” she says. “It should be centrally led and pushed for by the federal government.” Instead, Sell says, officials have veered between over-reassuring and over-worrying people. The Trump administration has undermined its own scientists, making people unsure whom to trust. “I've never had to deal with so much misinformation and, frankly, sometimes just unpredictability of the messaging that's been coming out, especially at the federal level,” Arwady said. With Americans befuddled as to which risks are acceptable, social media has overflowed with posts shaming people who appear to be in the company of other people. But these witch hunts miss the point that people generally don’t want to kill their friends and relatives. Most people want to do the right thing. But they can’t do it if they don’t know what it is. from https://ift.tt/36T4keF Check out http://natthash.tumblr.com On Monday, as President Donald Trump left Walter Reed National Military Medical Center, Senator Kelly Loeffler of Georgia tweeted a doctored clip of the president tackling and punching the wrestler Vince McMahon. In the edited version, McMahon’s face has been replaced with a picture of a virus. “COVID stood NO chance against @realDonaldTrump!” Loeffler wrote. Similar sentiments, trumpeting Trump’s strength and fighting spirit, have poured forth since he tested positive for COVID-19. “#TrumpStrong,” Twitter users wrote. “Our president is strong and will beat the virus,” said House Minority Leader Kevin McCarthy. “He’s a fighter,” said former press secretary Sarah Huckabee Sanders. He has the “strength and stamina” of someone decades younger, said a urologist. Such rhetoric is not unique to Trump. In the Western world, bouts of illness are regularly described as “battles.” Viruses and other pathogens are “enemies” to be “beaten.” Patients are encouraged to “be strong” and praised for being “fighters.” “It’s so embedded in our nature to give encouragement in that way,” says Esther Choo, an emergency physician at Oregon Health and Science University, “but it’s language that we try not to use in health care.” Equating disease with warfare, and recovery with strength, means that death and disability are linked to failure and weakness. That “does such a disservice to all of the families who have lost loved ones, or who are facing long-term consequences,” says Megan Ranney, an emergency physician at Brown University. Like so much else about the pandemic, the strength-centered rhetoric confuses more than it clarifies, and reveals more about America’s values than the disease currently plaguing it. The state of a person’s body and mind affects the course of a virus, but typically in subtle ways that aren’t captured by simplistic talk of “strength.” People who are infected with the SARS-CoV-2 virus are more likely to die or become severely ill if they are elderly, or have preexisting illnesses such as heart disease, cancer, or diabetes. But “we’ve seen very healthy, young, athletic, strong people get COVID-19 and die, or end up with long-term disability,” says Akiko Iwasaki, a Yale immunologist. College athletes have died from the disease. Some long-haulers, who have dealt with months of symptoms, were marathon runners and martial artists who have since struggled to walk up stairs. “I’ve seen not only elderly people with comorbidities, but also young people in their 30s, come in with visible respiratory distress,” says Uché Blackstock, an emergency physician and the founder of Advancing Health Equity. [Read: Long-haulers are redefining COVID-19.] Colloquially, people talk about having “strong” immune systems, easily boosted by good food and sufficient sleep. But immunity is famously complicated. Many people die because their immune system reacts to the coronavirus too forcefully for too long, creating a prolonged and sometimes harmful inflammatory state. “Some of the most distressing cases I have seen were young people who were fine and all of a sudden weren’t, and that was largely to do with how strong this immune overreaction was,” Ranney says. These overreactions also explain some intriguing connections between a person’s mental and physical health. In several experiments, Sheldon Cohen at Carnegie Mellon University, who studies the connections between the nervous and immune systems, has found that volunteers who suffer from chronic stress—especially unemployment or long-running personal conflicts—are more likely to fall sick after inhaling small doses of common-cold or influenza viruses. That’s not because, as Cohen initially assumed, stressed people are more likely to take up unhealthy habits, but because stress makes their immune system more likely to overreact. Cohen also found that people who are more emotionally positive are less likely to get sick from respiratory viruses. This fits with some other evidence (and a widespread belief) that optimists are more likely to recover from disease. But that connection is easy to misinterpret. It’s less that patients with viral diseases can will themselves better by putting on a happy face, and more that positivity reflects prior advantage. Optimists are more likely to have stronger social ties and adhere to medical advice. They’re less likely to have suffered the chronic stress that Cohen has linked to a higher infection risk. “I believe there are [psychological] factors that might extend your well-being,” says Choo, “but at the bedside, what I can tell you is that no one wants to die. Everyone is fighting to live with everything they have.” A pandemic can tear away emotional resources that can help in that fight. “One of the things that’s so difficult about this virus is the fear and loneliness that accompanies it,” Ranney says. “People can’t have their normal support systems. They can’t have friends and family at their bedside. I look like an alien in full personal protective equipment, and I can’t do any of the things that would enhance a patient’s resilience, like hold their hands.” As Susan Sontag wrote in 1978, it is difficult to enter “the kingdom of the ill unprejudiced by the lurid metaphors with which it has been landscaped.” Metaphors work by drawing connections between the familiar and the unfamiliar. This is useful when thinking about diseases, where unseen entities damage our bodies in largely unseen ways. By casting viruses as opponents, the immune system as defenders, and the course of illness as a fight, “we create a representation where we have control,” says Elena Semino, a linguist at Lancaster University. Metaphors have downsides, though. In studying metaphors for cancer, Semino has seen patients blaming themselves for the spread of their tumors—casting themselves as failures for not winning their battles. And when we use “strength” to describe muscles, immune systems, personality, morality, and political power, meaning hops from one sense to another. In the 19th century, a new movement called “muscular Christianity” deliberately connected moral and physical strength. Its proponents portrayed strenuous exercise and competitive sports as paths to hardy manliness, in opposition to what they saw as the softening feminization of Church and home. Muscular Christianity spurred the creation of the YMCA (and, by extension, basketball and volleyball). It became entwined with eugenics and imperialism, adding genetic and geopolitical “strength” to the metaphorical melting pot. It deeply influenced President Theodore Roosevelt, whose rugged persona was rooted in moving past the debilitating asthma of his childhood. “His effort to overcome the weakness of his youth instantiated itself through colonialism,” says Zoë Wool, a medical anthropologist at the University of Toronto. “He demonstrated strength through the claiming of nature in the name of the nation.” This connection between physicality and righteousness created, as its dark corollary, a link between disability and moral failing. That explains why presidents like Woodrow Wilson and Franklin D. Roosevelt tried to cover up their disabilities, on the misguided notion that “someone with a disability can’t be a good decision maker,” says Wool. It explains, she adds, why “we take it for granted that every villain in every classic story will be physically marked in some way,” including Captain Hook, Darth Vader, multiple Bond villains, and Scar from The Lion King (who, for extra measure, is also coded as queer). American society has long portrayed strength “as the opposite of disability and feminization,” Wool says. “Those go together, and are seen to be incapacitating. This is relevant in the case of Donald Trump.” As a patient, Trump has physical traits that place him among the riskiest categories for dying from COVID-19. He is also emotionally brittle, requiring constant validation and reassurance. But as his niece Mary Trump recently wrote, among Trump’s family, “weakness was the greatest sin of all.” So, in lieu of actual strength, Trump excels at performing a specific masculinized version of it, in which aggression, volume, stubbornness, overconfidence, and mockery are stand-ins for might. This is a man who sees wounded veterans and casualties of war as “suckers” and “losers.” “He’s a caricature of masculinity,” says Rosemarie Garland-Thomson, an emerita disability scholar at Emory University. [Read: Trump: Americans who died in war are ‘losers’ and ‘suckers’] But the leaky nature of metaphor allows displays of strength to be mistaken for its presence. “Strongman characterizations seem to revolve around the dispositional, temperamental features of a leader,” says Martha Lincoln, a medical anthropologist at San Francisco State University, “but I think there’s some magical thinking about the physical resilience of such a person too.” Even when Trump himself fell sick, he and his supporters couched his experience in the language of strength, victory, and courage. “Don’t let it dominate you,” he said in a video. This strength-centered rhetoric is damaging for three reasons. First, it’s a terrible public-health message. It dissuades people from distancing themselves from others and wearing a mask, and equates those measures with weakness and cowardice. “The more you personify the virus, the more one version of heroism is to ignore it,” says Semino. “When people take that idea to extremes, they say, I’m strong. I’m not going to be cowed by this.” Second, it ignores the more than 210,000 Americans who have died from COVID-19, and the uncounted thousands who have been disabled. Such dismissals are already common. In recent years, the ideologies of eugenics, where “if you’re sick, it’s your own fault and you don’t deserve support, [have] become more and more blatant,” says Pamela Block, an anthropologist at Western University. As the pandemic progressed, many saw the deaths of elderly people, or those with preexisting conditions, as acceptable and dismissible. And as COVID-19 disproportionately hit Black, Latino, Indigenous, and Pacific Islander communities, “people who believed in the idea of white supremacy felt like the virus was doing their work for them, and could promote the idea that they’re genetically stronger,” Block adds. One of Trump’s supporters recently predicted that the president would beat COVID-19 because of his “god-tier genetics”; Trump himself recently told a largely white audience that they have “good genes” before warning about incoming Somalian refugees. Third, “metaphors redirect our attention,” says Wool, the medical anthropologist, and create “dead zones” in our thinking. “The idea of fighting a disease creates this dyad between you and the illness” and distracts us from everything that affects that fight. Trump was born into wealth. He is white. He is the president of the United States. He had regular access to COVID-19 tests. He was given supplemental oxygen at the White House—his home—before being airlifted to Walter Reed, where he received dedicated medical care on taxpayer funds that he himself contributed nothing to in 10 of the past 15 years. When he apparently felt lonely, he left the hospital in a motorcade so he could wave to his supporters, exposing the Secret Service agents riding alongside him. He received three treatments—remdesivir, dexamethasone, and an experimental antibody cocktail from the biotechnology company Regeneron, whose CEO is an acquaintance of Trump’s and a member of one of his golf courses. “He received a level of care that no patient has received in this country, and a combination of medications that has probably never been given to another patient,” Blackstock, the emergency physician, says. “He’ll probably end up doing well because of his access to resources.” [Read: Donald Trump’s gold-plated health care] By contrast, many Americans have struggled to get tested for COVID-19 throughout the year—a problem that still dominates the lives of long-haulers who lack the diagnostic certainty needed for benefit claims or participation in research. Nearly 30 million Americans lacked health insurance last year, and that number has undoubtedly risen further amid record unemployment. Because of the combined burden of historical and everyday racism, many people of color must cope with chronic stress—the same stress that Cohen, the Carnegie Mellon researcher, showed makes them vulnerable to respiratory viruses in general. Many worked “essential jobs,” risking infections in unprotected workplaces and crowded public transport to make hourly wages that they couldn’t afford to lose. Acknowledging none of this, a defiant Trump told the country, “Don’t be afraid of it. You’re going to beat it. We have the best medical equipment. We have the best medicines.” Trump is hardly the first American to mischaracterize his own privilege as fortitude, but from his lips, that error is uniquely and doubly pernicious. It distracts not only from the massive advantages that he enjoys, but also from his singular role in America’s pandemic year. The horrors that others have endured are in large part the result of his ineptitude, and the same empty strength that he now claims has defeated the disease. Trump is both beneficiary and engine of the unequal, broken systems that have led to the deaths of more than 210,000 Americans, but have thus far averted his own. In the time since his diagnosis, more than 300,000 other people in the U.S. have tested positive. More than 4,000 have died. Their fates were not a matter of weakness, but their numbers should make the self-described most powerful nation in the world consider how strong it truly is. from https://ift.tt/3nJ7AiK Check out http://natthash.tumblr.com The sun was beaming, the air was clear, and it seemed as if President Donald Trump was finally taking coronavirus testing seriously. Standing in the White House Rose Garden early last week, Trump announced to buoyant officials that a “massive and groundbreaking expansion” in testing was under way: The federal government had purchased 150 million new coronavirus tests from the company Abbott Laboratories. These new rapid tests were “from a different planet,” Trump boasted. He was right. Each Abbott test cost only $5, one-20th the price of the most widely used test type. Instead of taking hours to deliver a result, the Abbott tests—which detect viral proteins—could provide an answer within 15 minutes. The government planned to send them to states, colleges, and nursing homes, a policy that would “more than double the number of tests already performed,” Trump said. Every state could, “on a very regular basis, test every teacher who needs it,” he promised. As Trump spoke, the coronavirus was already teeming through his body, information from his doctor now suggests. By the end of the week, the president, the first lady, and at least 23 of his advisers and staff were infected with the coronavirus. They had acted as if testing alone would protect them, but many of them seem to have been infected at a White House event where Abbott tests were used to screen visitors. This series of events could have ended another way, with tests such as Abbott’s allowing Americans to recapture a shred of normal life. But it has instead opened to public view an already ferocious debate among experts about the best way to defeat the pandemic—a fight with consequences that will outlast Trump’s symptoms. [Read: The president is not well] Since the spring, a group of experts led by Michael Mina, an epidemiology professor at Harvard, has called for the government to freely distribute tens of millions of 15-minute coronavirus tests a day. Never mind testing every teacher every day: Mina wants to test nearly every American every day, whether or not any given person shows symptoms of COVID-19. That’s impossible to do with the gold-standard reverse-transcription polymerase chain reaction, or PCR, tests—they are too expensive and take too long to return results. Frequent, cheaper testing, Mina claims, could defeat the pandemic within weeks, as infectious people are identified and quarantined. (We wrote about his plan in August.) Other experts are doubtful and have warned that cheap, rapid tests will not work as promised. If distributed en masse and used to screen asymptomatic people, these antigen tests will deliver hundreds of thousands—if not millions—of false results, they say. False negatives could lead to reckless behavior by people who don't know they're sick. False positives can also put people at risk: If a virus-free nursing-home resident with a false positive is placed in a COVID-19 ward, that person could become infected. “The point I'm trying to make here, and I'll be blunt, is that antigen testing will not and cannot work for asymptomatic screening, and [it] will probably kill a lot of people,” Geoffrey Baird, the acting laboratory-medicine chair at the University of Washington, told us. His lab at UW developed one of the earliest accurate COVID-19 tests in the U.S., and is widely respected within the diagnostic-testing field. Alexander McAdam, the director of the infectious-diseases diagnostic laboratory at Boston Children’s Hospital, told The New York Times that deploying the current antigen tests to screen populations “is a bad idea, and I’ll die on that hill.” The stakes of this dispute are not only how Abbott tests are used, but whether they should be used at all. It could shape federal policy next year and determine whether more money is spent on fixes to address the virus aside from a vaccine. Already, this conflict is playing out on the state level. In Nevada, public-health authorities have told nursing homes to stop using two models of antigen-test machines, which the federal government has sent to more than 14,000 facilities, after only 16 of 39 positive tests were confirmed by subsequent PCR testing. [Read: This overlooked variable is the key to the pandemic] What everyone agrees on is that the tests were not deployed responsibly at the White House. The president hosted dozens of guests at a ceremony honoring Supreme Court nominee Amy Coney Barrett, without masks, amid a raging pandemic, and rejected some of the most basic safety protocols. As that event has demonstrated, testing must be an and strategy, not an or one. Rapid testing and masking. Rapid testing and social distancing. Rapid testing and vaccines. “Testing is a belt-and-suspenders approach that adds incremental safety,” Baird said. “Belts and suspenders only work, though, when you are wearing pants.” The president also seems to have personally rejected testing for himself. Trump’s doctor has persistently dodged questions about when the president last tested negative. The New York Times reported that Trump—who officials once claimed was tested “multiple times a day”—was not swabbed even once a day. The debacle has accelerated preexisting concerns about the rollout of the Abbott tests. Late last month, even the proponents of rapid testing worried about the plans to distribute and use the Abbott tests. Mina, generally an advocate of rapid testing, warned that if the Abbott tests were not deployed the right way, with the proper safeguards and solid public education, they could further erode trust in the nation’s public-health systems. The White House's cavalier actions have now realized that fear. These tests have the potential to create two problems. One is commonly cited by critics and very easy to understand: False negatives will give people too much confidence that they are virus-free, just like the White House attendees who drank and celebrated together without masks, even hugging one another. Given a negative test result, many people chose to eschew the simple precautions that have helped slow the spread of the virus. The other problem is that these tests will generate many false positives, especially if deployed in asymptomatic populations where relatively few people are sick. It could very well be that, as in Nevada, the majority of positive test results are false. Besides the risks of grouping healthy people with those who are actually sick, false positives will keep well people home from work unnecessarily and prompt people to seek “confirmatory” PCR tests, potentially overwhelming an already fragile system. Mina and other proponents argue that rapid antigen tests could still be useful with their current performance, but that distribution and communication must be improved. “If these tests are not messaged appropriately, we run the risk of the whole program coming crashing down pretty much immediately,” Mina told us. [Read: How we survive the winter] The early signs are not encouraging. The new Abbott test, the Binax NOW, received an emergency use authorization (EUA) based on results from just 102 samples. The next day, the government spent $760 million to buy the entire supply of tests. Notably, the FDA did not support the use of the test for screening asymptomatic people—which the most ambitious version of Mina's plan depends on. The emergency use authorization only covered testing for people within the first seven days of developing symptoms, when viral loads remain high. In asymptomatic people, the tests will likely perform worse. The levels of virus are likely to be lower in any individual infected person, which would increase the false-negative rate. And in the general, symptom-free population, the expected levels of infection are actually quite low, so the false-positive rate could be very high. Yet Admiral Brett Giroir, the administration’s “testing czar” and an assistant secretary at the U.S. Department of Health and Human Services, has explicitly said that the tests could be used for asymptomatic screening, at schools perhaps. That contradiction worries Baird. “One branch of the government is saying, ‘Use this test for asymptomatic people,’ and then on the other side, they are saying, ‘Use this test for symptomatic people,’” he said. Baird is particularly anxious that the performance of tests will deteriorate in the field and when applied to asymptomatic people. That always happens with lab tests, he told us. “They haven’t published clinical-trials data,” he said. “You foist that test on the public after collecting evidence that it would work.” False positives worry Mina, too. Among people tested within the first seven days of showing symptoms, the Abbott test will, according to its EUA, generate a false positive from roughly one in 50 tests. Because relatively few people test positive out of the whole population, those false positives could represent a large percentage of the positive results that a batch of the tests would generate. For now, the solution is supposed to be for people who test positive to get a confirmatory PCR test. But “saying that these tests need to be confirmed with a PCR test isn’t a good answer,” Mina told us. If a “quick” positive result then forces people to wait four days for a PCR positive, the first result stops meaning much. Mina suggests that a cornucopia approach could provide the answer: If you take an Abbott test and get a positive result, then you would take another quick test, made by a different company, that detects a different viral protein, for confirmation. He said that such procedures were common in screening for relatively rare diseases, such as HIV, where the Centers for Disease Control and Prevention issues an “algorithm” for sequencing tests. “People are just thinking about COVID testing differently for some reason, but imperfect screens are pretty common, so I am scratching my head,” says Dan Larremore, a computer scientist and an infectious-disease modeler at the University of Colorado, who has collaborated with Mina. “The perfect has really been the enemy of the good here, in many ways—except that we also know how to embed the good within follow-up systems to make it nearly perfect.” Mina is running a trial comparing PCR and antigen tests in both symptomatic and asymptomatic people, in order to generate real-world data about false positives and negatives. “My hope is that six weeks from now, we’ll have a pretty good set of data to reflect the performance,” he said. He still thinks these quick, cheap tests could help America overcome the pandemic. “The point people are really missing is: What is the alternative? The alternative is no testing. Most K–12 students are not getting tested,” Mina said. “Every time we can pull a positive person out of the population, we stop tens, hundreds, or thousands of cases.” The alternative for Baird is obvious: keep going with the behavioral interventions that have helped at least slow the spread in the U.S. “I think the quintessential problem in the country is an imbalance of supply and demand of testing,” Baird said. “Mina’s solution is increasing supply. And I have a strong belief that decreasing demand will be the way to get there—masking, physical distancing, not having large events. And, unfortunately, absorbing the societal toll that all of those things take.” While the surface of the debate is about the technological characteristics of these tests, the substance of it is about human behavior. As restrictions on daily life enter their seventh full month and winter draws near, will the countermeasures that have limited, but never contained, the virus’s spread remain in force? And if we add tests that generate imperfect information, will that embolden people to abandon commonsense safety precautions? No test—and no testing strategy—is perfect; we are living through a pandemic, and people will get sick. To believe that antigen testing can improve life in this country is to believe that people will understand the limits of a test result and act accordingly. With the right public messaging, perhaps they could. from https://ift.tt/3lrM9kc Check out http://natthash.tumblr.com When I first waded into the latest mask conspiracy theory, I was literally wading. About a month ago, I was in my local pool when I overheard a middle-aged woman in the next lane whisper it to her friend, in the way you vaguely assert something that you’re pretty sure is true but don’t fully understand. “Masks don’t even do anything,” she said. “In fact, they can make you sicker. Because you’re breathing in all the ... stuff ... you breathe out.” “OK Boomer,” I thought. I dismissed her as a random neighborhood conspiracist and swam my laps. But then I started to see this false notion appear more frequently on Facebook. It wasn’t the typical argument anti-maskers use, that mask mandates infringe on people’s freedoms. It was that the masks themselves are causing illness. The horror of the idea was apparent even to me: the feds, in their hall-monitor stupidity, forcing you to do something that’s actually bad for you. Most recently, this surfaced in the form of “copypasta”—a post copied and pasted by many people onto social media, rather than shared as a link—from a purported “OSHA Inspector.” “I have worked in a clean room for 23 years and 10 years on submarines before that,” it reads. The inspector, supposedly from the Occupational Safety and Health Administration, goes on to debunk each type of mask. N95s won’t “filter your air on the way out,” so they don’t reduce the risk of catching COVID-19 from someone who has it. Surgical masks, the post claims, are rendered useless by the moisture from your breath and the “amount of particles” on them. Cloth masks, meanwhile, trap carbon dioxide, risking the health of the wearer. “I know, facts suck,” it concludes. “They throw a wrench into the perfectly (seeming) packaged pill you are willingly swallowing.” [Read: Trump’s Gold-Plated Health Care] Aside from the fact that few bureaucrats speak this plainly and concisely, there are a number of obvious signs that this information is false. Every kind of face mask has been proved, in study after study, to slow the spread of COVID-19, with N95s being the most effective. To name just one example, two stylists worked at a hair salon in Missouri while infected with the coronavirus, but none of the 139 clients they saw got sick, because everyone wore masks. Mainstream experts dismiss the idea that wearing a mask can make you sick, unless you never wash the mask or have a health condition that makes breathing difficult. “The way that masks are being recommended is perfectly safe,” says Angela Rasmussen, a virologist at Columbia University. Cloth masks don’t offer complete protection against the coronavirus, she says, but they reduce the risk enough that they’re worth wearing whenever you’re going to be around people. Though the latest public posts mentioning the supposed OSHA inspector date from September, the idea that masks make you sicker has been spreading online for months now, even after various fact-checking sites debunked the claim. I emailed Facebook to ask for more information about this type of post, but the company did not respond. One instance of the OSHA post was taken down after my email. But others live on, circulating among mask-haters and affirming what they perceive to be their righteousness. The post is an especially bizarre example of the “infodemic” scientists have been battling alongside the coronavirus pandemic, in which the internet is a giant telephone game reverberating with the weirdest stuff imaginable. In late July, the “masks make you sick” claim was already circulating in prominent conservative circles. In a video, the conservative activist Charlie Kirk said, “Some doctors think that masks actually make you sicker and have you less likely to be able to get oxygen.” (I reached out to Kirk on Twitter, but he did not respond.) The OSHA connection also came up in an anti-mask video made by a conservative chiropractor with 3,000 Facebook followers. But the previous month, the OSHA claim had already been widely debunked. Snopes wrote an article on June 18 refuting a near-identical version of the Facebook post that was still bouncing around in September. Not only does the post have its science wrong—people wearing cloth masks are in no danger of breathing in too much carbon dioxide—but it also refers to an OSHA certification that does not exist. “The author of the Facebook post claimed to be ‘OSHA 10&30 certified,’” the Snopes article says. “We reached out to OSHA, and a representative told us that these courses ‘do not include COVID-19 topics,’ nor does OSHA ‘certify’ trainers.” [ Read: The Most American COVID-19 Failure Yet ] It’s not clear how OSHA got roped into this. Part of the Department of Labor, the agency primarily concerns itself with safe working conditions, rather than pandemic responses. People who don’t want to do something, like wear masks, will often glom onto quasi-scientific rationalizations, says Matt Motta, a political scientist at Oklahoma State University who studies online misinformation. Outside of Facebook, a June 18 article on a site called GreenMedInfo claims that “OSHA says masks don’t work—and violate OSHA oxygen levels.” The article consists mainly of a video by Peggy Hall, the founder of an anti-mask site called thehealthyamerican.org, explaining how “the U.S. Department of Labor Occupational and Safety and Health Administration’s guidelines clearly show cloth and surgical masks don’t work to reduce transmission of COVID-19, and how they deplete the body of oxygen, causing adverse health effects.” (In response to a request for comment, an OSHA spokesperson told me that this is not true, and that masks do not compromise oxygen levels or cause carbon dioxide buildup.) The video is no longer available, and when I emailed Hall, she said it had been taken down. “My now-banned videos simply explained that OSHA, the FDA and the CDC all have no evidence of masks preventing the spread of this virus,” Hall wrote. (They do.) “Since they are making the claim, the burden of proof is on those agencies to show that the masks DON’T make anyone sick.” This is, of course, a completely different statement than the one made in the article. And indeed, a few days later, the fact-checking site PolitiFact debunked Hall’s article, too. Before that, anti-mask articles and advocates would occasionally claim that masks made people sick, but they rarely invoked OSHA. A Chattanooga, Tennessee, news station in early June claimed, “Wearing a fabric mask for long periods of time—or for several days at a time—can allow bacteria to build up and actually make you sick,” but didn’t cite any research or experts to back the claim. In May, a group of filmmakers released a video titled Plandemic, which traveled widely on social media. It featured the discredited researcher Judy Mikovitz saying, among other things, that masks can make people sick. Plandemic was viewed millions of times before Facebook and YouTube removed it. (Mikovitz did not respond to a request for comment.) These videos and articles all came months after government officials had begun encouraging—and then mandating—that people wear masks in public. But crucial to understanding the spread of this particular piece of misinformation is that, for many weeks early in the pandemic, everyday people were told not to wear masks. Back then, prominent experts claimed masks were needed for health-care workers and were borderline ineffective for the general public. Versions of this advice also suggested that masks could raise the risk of illness. On March 12, Jenny Harries, England’s deputy chief medical officer, claimed that masks could “actually trap the virus.” Therefore, she said, “for the average member of the public walking down a street, it is not a good idea.” (Harries did not respond to a request for comment.) In fact, the earliest instance of a “masks make you sicker” claim I could find was in a February 27 news article published on a Utah radio station’s website. (Its author did not return a request for comment.) Though the article has since been updated, the original contains the subhead “Wearing a face mask incorrectly might put you at greater risk of getting sick.” The article then quotes a doctor named David Eisenman as saying, “I think people see a mask and they see an illusion of protection.” Though Eisenman’s quote does not quite support the subheading on the article, I reached out to him to see whether he still stands by his interview. In short, he does not. “These things come back and haunt you,” Eisenman, a professor-in-residence at UCLA, told me. “Science recommendations have evolved. Now I would say that the evidence is very much in favor of masks as an important protector in the spread of COVID-19.” Eisenman says the article was widely read. People occasionally tweet at him asking how he can be recommending masks now when he didn’t six months ago. He explains that the science changed, and so did his advice, but according to him, “it doesn’t seem to satisfy anybody.” The “masks make you sicker” idea underscores how online misinformation is like an ocean liner: Once it’s headed in one direction, it’s difficult to turn around. The advice on masks changed seven months ago, but some people have stuck with what experts were saying in the confusing early days. One doctor’s criticisms of masks—which he now recants—live on in Twitter threads. And as people find new ways to share incorrect information, through posts, photos, and videos, social-media platforms are struggling to catch and remove all the hokum. Before long, the conspiracy theories break free of Facebook and infect reality. from https://ift.tt/2GLjCHg Check out http://natthash.tumblr.com For the past several days, President Donald Trump has had COVID-19. It’s unclear for how many days, because the president’s physician, Sean Conley, refuses to share that information. When asked again yesterday, Conley told reporters, “I don’t want to move backwards.” In fact, Conley has shared very little about the course of the president’s illness. On Friday, the same day Trump informed Americans that he had tested positive, he was taken to the hospital “out of an abundance of caution,” according to his press secretary. By the next morning, the narrative had shifted. Conley said that Trump was “doing much better,” but relative to what, exactly? Then, on Monday, Conley told reporters that the president was to be discharged to the White House. “He’s back,” Conley said with a smile. To hear Conley tell it, Trump was also never gone. The story of his illness jumped from “nothing to see here” to “mission accomplished.” Trump reportedly worked out of the presidential suite at the military hospital as the White House reassured Americans that his job could be done well from there. It released images of him in a suit at a desk, next to a telephone. Now, according to Conley, the president is back at the White House, where he can get “world-class medical care, 24/7.” (Conley could not be reached directly, and the White House did not immediately respond to a request for comment.) Last night, Trump was helicoptered back to the White House, crossing the lawn and removing his mask to salute Marine One in a spectacle that quickly was turned into a gauzy campaign-style video. The president is declaring victory. “Don’t be afraid of COVID,” he tweeted earlier in the day. “Don’t let it dominate your life.” This is a dangerous narrative, and Trump’s doctor has helped to shape it. Conley has served as Trump’s publicist in a white coat, reassuring Americans at every turn that Trump is doing well, while leaving out conspicuous details. His vaguery and obfuscation have repeatedly undermined these reassurances. His ethical obligation to his patient is in direct conflict with the basic moral imperative not to lie, by omission or otherwise. Any physician has a duty to the public as well, specifically when dealing with a patient who poses a direct threat to others. Conley is seemingly intent on informing the country how strong the president is, making him complicit in the downplaying of this disease when what the country needs is the bare truth. The American people still do not know when the president was infected with the coronavirus. We know little more than Trump’s age, his current vital signs, and some of the medications he is taking. Just since Saturday, Conley has declined to answer the most basic questions: Does the president have pneumonia? Why did he start taking dexamethasone? What blood tests have been abnormal? When asked by reporters for discrete data such as the president’s oxygen-saturation levels, Conley said, “Less than 94.” If there is one value that a doctor should know precisely about a patient who is being monitored for respiratory failure—for which the low 90s constitute an unstable zone—it’s this number. [Read: The president is not well] Conley has changed the story. In a press conference on Saturday, he said that Trump was not on supplemental oxygen, and then conspicuously avoided three direct questions as to whether he ever had been. But then, on Sunday, he claimed that the president had received supplemental oxygen in two instances during his illness. Conley said that he had concealed the fact before because he “was trying to reflect the upbeat attitude that the team, the president, [and] his course of illness has had … In doing so, you know, it came off that we were trying to hide something, which wasn’t necessarily true.” Maybe the biggest lingering question surrounding Conley’s statements is the decision to start Trump on dexamethasone, even while Conley has repeatedly denied that the president has had significant respiratory issues. Dexamethasone is a commonly used steroid, sometimes prescribed for COVID-19 patients in an attempt to tamp down the immune response that can cause them to crash after an initial phase of mild symptoms. But the Infectious Disease Society of America does not recommend the drug for patients who are not in “severe” or “critical” stages of COVID-19. When reporters asked Conley to explain this treatment decision on Monday, he expressed indignation at the question: “I’m not going to go into specifics of what he is and is not on.” Conley has also referenced “expected” findings in Trump’s chest-imaging tests, but that’s different from “normal,” the term doctors use to denote that nothing is wrong. “Expected” findings are not necessarily good. Conley repeatedly declined to elaborate. He also mentioned abnormal blood tests, but would not say more. On Monday, he alluded to abnormalities in Trump’s kidney functioning, saying that blood tests showed the president had been “dehydrated,” but that this test had returned to normal. For dehydration to temporarily impair the kidneys is not uncommon. It’s not typically concerning. What is concerning is Conley’s unwillingness to just say that, instead resorting to dodges like “I’m not going to get into operations” and invoking HIPAA when asked about abnormal findings. Every patient has a right to privacy, and there are some issues that the president may not want to go into extreme detail about. It’s possible that Trump directed his doctor not to talk about certain findings. As the president’s physician, Conley is not an elected official: His primary duty is to Trump. He may consider himself to be a responsible citizen and doctor as long as he is leaving the American people with a basic feeling that the president is doing fine. But a doctor who is at liberty to discuss only normal and positive findings should not be holding a press conference. The job of a physician is not to reflect an upbeat attitude. It is not to conflate optimism with obfuscation. The job of a physician is to deal in reality—to neither minimize threats nor overemphasize them. The unique bioethical dilemma of the moment is that we are in the middle of a pandemic. Accepting reality, and a shared set of facts, is vital. And there is one crucial exception to a doctor’s obligation to protect a patient’s privacy: when that patient is a threat to others. On Monday, when Conley told reporters that he had given Trump the go-ahead to return to the White House, he could not say whether or how Trump would isolate himself for the rest of his illness. He is presumably still contagious (unless he has already had the virus for 10 days). That is: The president, in the throes of COVID-19, was being discharged back to the very site of a major coronavirus cluster. Why send a contagious person back to the place where an outbreak is still unfolding, if he is able to quarantine and execute his duties in his presidential suite at Walter Reed? [Read: Trump’s doctor comes from a uniquely American brand of medicine] Conley even defended the president’s decision on Sunday to break quarantine and go on a car ride with Secret Service agents, which an attending physician at Walter Reed called “insanity.” At the very least, the appropriate response from Conley would have been to say “I advised against that.” Statistically, Trump is most likely to continue recovering uneventfully. This decision to return home is not clearly medically unwise for him. But the declaration of victory and the overall downplaying of Trump’s medical status do a grave disservice to the public. And though it is within Trump’s purview, going back home is, at the very least, inconsiderate of the staff at the White House. That creates risk not just for those who work there, but everyone who has contact with those people, and then everyone who has contact with those people. As the current cluster at the White House has made abundantly clear, a single negligent act can end up leading to multiple cases. Such acts are preventable. Most happen because of failures to take basic precautionary measures. Since the beginning of the pandemic, Trump has repeatedly failed to take such measures, and he continues to dismiss the threat, denying simple facts and implying that some form of exceptionalism will exempt Americans from suffering. Meanwhile, more than 200,000 Americans have died from COVID-19. Conley has had ample opportunities to do what Trump hasn’t done—speak objectively about the medical facts. Simply doing so would emphasize the importance of wearing masks and taking the virus seriously. Instead, Conley has opted for complicity, becoming a mouthpiece for Trump’s show of personal strength. Americans are left to speculate about Trump’s health based on what they see in curated videos and press photos—none of which show him in a hospital gown or even in a medical setting. In another time and place, it may be fine to respect a president’s privacy regarding medical issues that have no bearing on ability to govern. But downplaying Trump’s case of COVID-19 in this unique moment has widespread consequences. The hundreds of millions of Americans who are still at risk of contracting this disease could have seen the realities of what it is like, and better understood the value of stopping the virus. Instead, they have been shown that the consequences of negligence are cinematic helicopter rides and a weekend spent wearing a suit in the hospital. from https://ift.tt/30GL3ZR Check out http://natthash.tumblr.com |
Authorhttp://natthash.tumblr.com Archives
April 2023
Categories |
 RSS Feed
RSS Feed
