|
Thinking too hard about saliva can really ruin a nice meal. And to eat inside a restaurant in 2020 requires ignoring the harsh reality of drool: the residue left behind by a chip dipped in a shared bowl of guacamole, the flecks of spit flung loose by a drunken laugh, and the veritable makeout session that is sampling someone else’s cocktail. The unfortunate ubiquity of mucus is why restaurants, it brings me no pleasure to report, are contributing to the spread of the coronavirus. Indoor public places, including restaurants, played a significant role in the spread of COVID-19 this spring, according to scientific analyses of cellphone data. In a September study, people who tested positive for COVID-19 were more than twice as likely as those who tested negative to report eating in a restaurant recently. Talking with someone who has COVID-19 for 30 minutes or longer—about the time between your bloomin’-onion appetizer and molten-chocolate dessert—more than doubles your odds of catching it. So why on earth would anyone eat inside a restaurant right now? This is the question I mulled as I walked up and down the Crystal City strip in Virginia last week, dressed in a mask and an Ann Taylor sweater. I had journeyed to this chunk of suburban Washington, D.C., near the Pentagon, because, despite its concrete-y soullessness, it has the advantage of being home to several restaurants in a row. And they are popular restaurants—not your TGI Fridays, but not your two-tables-and-a-vegan-tagine either. In all, I approached and interviewed about a dozen random people as they walked out of restaurants in Crystal City, and later in another little patch of Northern Virginia called the Mosaic District, a mixed-use development off a giant highway. These were not anti-mask COVID-19 deniers; people were clearly following the official rules. Nearly everyone on the street wore a mask, including the diners as soon as they exited their restaurant of choice. A man watching TV from the bar inside a Thai place had a mask on. So did the women walking down the street talking about their pharmacy-school applications. Still, lots of people were eating indoors, even though it was a balmy, 66-degree night in early November. Unless you’re extremely plugged into the public-health world, there’s little reason you would pause before eating inside. Many of the places I passed had signs outside announcing We’re Open! Like 44 other states as of this writing, Virginia hadn’t banned eating indoors, even though the day after my interviews there were 14 coronavirus cases per 100,000 people in Fairfax County and 17 in Arlington. That’s well over the 10-per-100,000 measure that Caitlin Rivers, an assistant professor at the Johns Hopkins Bloomberg School of Public Health, told me recently was her ceiling for socializing indoors with friends and family only. Outside McCormick & Schmick’s, a chain seafood place, I stopped three men who had just had a business dinner together. They refused to give me their full names, so I’ll identify them by the color of their masks. These three seemed relatively unconcerned about the virus. One of them, Red Mask, said he was still going to the gym; Blue Mask said he had gone to the barber recently and was impressed with how long his hairdresser spent wiping down his chair. (This is largely for show; surfaces are now thought to be less important to the spread of the virus than aerosols and droplets from other people). Black Mask told me that he was willing to go into any open restaurant. “I’m not in a high-risk category, so if I got it, it wouldn’t bother me that much,” he reasoned. They asked me, somewhat aggressively, if I would eat inside a restaurant. I said I probably would not. And then of course I sounded weird, because why wouldn’t you eat in a place that’s open? Each of us, to get through this terrible time, has clung to some coronavirus factoid or another that we believe protects us. Here’s mine: The odds of catching the coronavirus are about 20 times higher indoors than outdoors. This year I have eaten on patios, in backyards, and on benches outside. But I haven’t sat down inside a restaurant since March, and probably won’t for many more months. “Indoor eating and bars and coffee shops are among the riskiest activities you can do. Outdoors is dramatically better,” says Alex Huffman, an aerosols researcher at the University of Denver. Several of the restaurant patrons I talked with didn’t share this belief. One man, Steve Harris, even suggested that he was taking a bigger risk talking with me outdoors, with a mask on, than he was eating indoors, without a mask. (Our conversation was much less risky, but I felt awful nonetheless.) Think about when you’re standing on a back patio at a friend’s house, he said, just having a couple of beers, and the sun is setting. You can see peoples’ spit glimmer as it flies out of their mouth into the twilight air. Disgusting, right? Probably more disgusting than having a Blue Creek cheeseburger at Ted’s Montana Grill in November 2020. (Except that indoors, these speech droplets stay in the air for eight to 14 minutes. Not everyone would know this, because Donald Trump and his coronavirus advisers constantly spread incorrect information about the virus.) Most people told me that they wouldn’t eat at just any restaurant; they’d have to see “precautions” in place. Peoples’ desired precautions ranged from the waitstaff wearing masks to air purifiers to seeing tables spaced apart with partitions separating them. One couple, told me, charmingly, that during the pandemic they will eat only in restaurants they are already “familiar with,” as though knowing your way around a menu can protect you from an invisible virus. The thing is, the precautions restaurants advertise aren’t all very effective, according to experts. One woman who was dining out with her boyfriend told me that she likes to see temperature checks at restaurants. That makes sense, because retail establishments have been ostentatiously taking their patrons’ temperatures for months now. But temperature checks are security theater; not everyone who has COVID-19 has a fever, and a fever can be caused by something other than COVID-19. Measures such as spacing tables apart and installing air purifiers can be helpful, experts told me, but they can’t eliminate the risk entirely. Partitions don’t do much, Huffman says: “They could actually help the aerosol pool on one side of it by disrupting the whole ventilation flow.” Near the Mosaic District, Silver Diner displayed a sign that claimed the establishment was Making Indoor Dining Like Outdoors, in part through the use of ultraviolet lights, both inside its HVAC system and beaming toward surfaces. Do Hyung Kim, who had just finished up a meal with his wife inside the diner, told me that the UV lights made him feel safer, since he had read about them in the newspaper. But two experts I spoke with said there’s still not much evidence that UV lights prevent infection. “The data behind that is not definitive,” said Tom Tsai, a health-policy professor at Harvard. Why are people willing to risk it all for a T-bone? In general, humans tend to fall victim to “comparative optimism,” in which we believe that bad things are more likely to happen to other people. There’s still a relatively low likelihood of contracting COVID-19 during any given restaurant outing, but “people aren’t particularly good at perceiving that kind of risk,” says Toby Wise, a researcher at Caltech who has studied coronavirus risk perception. People don’t learn from statistics, such as cases per 100,000, but rather from their own experiences, says Maria Konnikova, a psychologist and the author of The Biggest Bluff, about the psychology of gambling. Eating at restaurants is comforting and familiar, which breeds “overconfidence and the downplaying of downside risk,” she says. How could something so fun hurt us? Plus, it’s not like authority figures are telling us to stay out of restaurants. “When there’s a muddled message, you don’t err on the side of safety,” Konnikova says. “You err on the side of desire, especially if you’re tired of quarantine.” Though some of my interviewees were drawn to the soft glow of a noodle joint because of their boredom at home or their desire for a date night, others were venturing out for the good of the restaurants themselves. With no additional coronavirus aid coming, “the money we just spent in there is gonna make sure that people are employed,” a man named Mark told me in Crystal City. “It’s absolutely important for all of us, if we’re comfortable, that we should do that. Because I’ll tell you what: The economy is our most important asset in our country.” This is the bind the government has put us in: Risk your life to eat inside a beloved restaurant, or it might not exist when this is all over. I asked all the people I spoke with whether they would be angry at government officials, the restaurant, or any other powers that be if they caught COVID-19 from eating indoors. They all said they wouldn’t be. After all, restaurants are just one of the many types of businesses that remain open; they could have contracted it anywhere. In part because our leaders have let the virus spread uncontrolled, it sometimes seems like it is an unstoppable threat and, like the weather, there’s not much you can do about it. That thinking can lead to a certain kind of fatalism. When I talked with Gabrielle Velasco and George Kosmidis, a young couple outside a Spanish restaurant called Jaleo, Kosmidis said he was still going into an office regularly. So “I think there’s a level of risk no matter what you do,” he said. Velasco added that she was nevertheless frustrated with the overall government pandemic response. If you think about it, she said, the service staff, who work in close quarters all day, is taking on a bigger risk than the diners are. Why not risk a little when other people are risking so much? Reached for comment about the state’s indoor-dining situation, a spokesperson for Virginia Governor Ralph Northam said he “is working closely with state and local health experts, and he will continue to base his decisions in data, science, and public health.” A few days after my interviews, Northam announced that he would require restaurants to stop serving alcohol after 10 p.m. and to close by midnight. Of course, how much time people spend inside restaurants before then is still entirely up to them. from https://ift.tt/3fh0DBy Check out http://natthash.tumblr.com
0 Comments
Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. Perhaps no hospital in the United States was better-prepared for a pandemic than the University of Nebraska Medical Center in Omaha. After the SARS outbreak of 2003, its staff began specifically preparing for emerging infections. The center has the nation’s only federal quarantine facility and its largest biocontainment unit, which cared for airlifted Ebola patients in 2014. They had detailed pandemic plans. They ran drills. Ron Klain, who was President Obama’s “Ebola czar” and will be Joe Biden’s chief of staff in the White House, once told me that UNMC is “arguably the best in the country” at handling dangerous and unusual diseases. There’s a reason why many of the Americans who were airlifted from the Diamond Princess cruise ship in February were sent to UNMC. In the past two weeks, the hospital had to convert an entire building into a COVID-19 tower, from the top down. It now has 10 COVID-19 units, each taking up an entire hospital floor. Three of the units provide intensive care to the very sickest people, several of whom die every day. One unit solely provides “comfort care” to COVID-19 patients who are certain to die. “We’ve never had to do anything like this,” Angela Hewlett, the infectious-disease specialist who directs the hospital’s COVID-19 team, told me. “We are on an absolutely catastrophic path.” To hear such talk from someone at UNMC, the best-prepared of America’s hospitals, should shake the entire nation. In mid-March, when just 18 Nebraskans had tested positive for COVID-19, Shelly Schwedhelm, the head of the hospital’s emergency-preparedness program, sounded gently confident. Or, at least, she told me: “I’m confident in having a plan.” She hoped the hospital wouldn’t hit capacity, “because people will have done the right thing by staying home,” she said. And people did: For a while, the U.S. flattened the curve. But now, about 2,400 Nebraskans are testing positive for COVID-19 every day—a rate five times higher than in the spring. More than 20 percent of tests are coming back positive, and up to 70 percent in some rural counties—signs that many infections aren’t being detected. The number of people who’ve been hospitalized with the disease has tripled in just six weeks. UNMC is fuller with COVID-19 patients—and patients, full stop—than it has ever been. “We’re watching a system breaking in front of us and we’re helpless to stop it,” says Kelly Cawcutt, an infectious-disease and critical-care physician. [Read: ‘No one is listening to us’] Cawcutt knows what’s coming. Throughout the pandemic, hospitalizations have lagged behind cases by about 12 days. Over the past 12 days, the total number of confirmed cases in Nebraska has risen from 82,400 to 109,280. That rise represents a wave of patients that will slam into already beleaguered hospitals between now and Thanksgiving. “I don’t see how we avoid becoming overwhelmed,” says Dan Johnson, a critical-care doctor. People need to know that “the assumption we will always have a hospital bed for them is a false one.” What makes this “nightmare” worse, he adds, “is that it was preventable.” The coronavirus is not unstoppable, as some have suggested and as New Zealand, Iceland, Australia, and Hong Kong have resoundingly disproved—twice. Instead, the Trump administration never mounted a serious effort to stop it. Whether through gross incompetence or deliberate strategy, the president and his advisers left the virus to run amok, allowed Americans to get sick, and punted the consequences to the health-care system. And they did so repeatedly, even after the ordeal of the spring, after the playbook for controlling the virus became clear, and despite months of warnings about a fall surge. Not even the best-prepared hospital can compensate for an unchecked pandemic. UNMC’s preparations didn’t fail so much as the U.S. created a situation in which hospitals could not possibly succeed. “We can prepare over and over for a wave of patients,” says Cawcutt, “but we can’t prepare for a tsunami.” A full hospital means that everyone waits. COVID-19 patients who are going downhill must wait to enter a packed intensive-care unit. Patients who cannot breathe must wait for the many minutes it takes for a nurse elsewhere in the hospital to remove their cumbersome protective gear, run over, and don the gear again. On Tuesday, one rapidly deteriorating patient needed to be intubated, but the assembled doctors had to wait, because the anesthesiologists were all busy intubating four other patients in an ICU and a few more in an emergency room. None of the people I spoke with would predict when UNMC will finally hit its capacity ceiling, partly because they’re doing everything to avoid that scenario, and partly because it’s so grim as to be almost unthinkable. But “we’re rapidly approaching that point,” Hewlett said. When it arrives, people with COVID-19 will die not just because of the virus, but because the hospital will have nowhere to put them and no one to help them. Doctors will have to decide who to put on a ventilator or a dialysis machine. They’ll have to choose whether to abandon entire groups of patients who can’t get help elsewhere. While cities like New York or Boston have many big hospitals that can care for advanced strokes, failing hearts that need mechanical support, and transplanted organs, “in this region, we’re it,” Johnson says. “We provide care that can’t be provided at any other hospital for a 200-mile radius. We’re going to need to decide if we continue to offer that care, or if we admit every single COVID-19 patient who comes through our door.” [Read: How many Americans are about to die?] During the spring, most of UNMC’s COVID-19 patients were either elderly people from nursing homes or workers in meatpacking plants and factories. But with the third national surge, “all the trends have gone out the window,” Sarah Swistak, a staff nurse, told me. “From the 90-year-old with every comorbidity listed to the 30-year-old who is the picture of perfect health, they’re all requiring oxygen because they’re so short of breath.” This lack of pattern is a pattern in itself, and suggests that there’s no single explanation for the current surge. Nebraska reopened too early, “when we didn’t have enough control, and in the absence of a mask mandate,” Cawcutt says. Pandemic fatigue set in. Weddings that were postponed from the spring took place in the fall. Customers packed into indoor spaces, like bars and restaurants, where the virus most easily finds new hosts. Colleges resumed in-person classes. UNMC is struggling not because of any one super-spreading event, but because of the cumulative toll of millions of bad decisions. When the hospital first faced the pandemic in the spring, “I was buoyed by the realization that everyone in America was doing their part to slow down the spread,” Johnson says. “Now I know friends of mine are going about their normal lives, having parties and dinners, and playing sports indoors. It’s very difficult to do this work when we know so many people are not doing their part.” The drive home from the packed hospital takes him past rows of packed restaurants, sporting venues, and parking lots. To a degree, Johnson sympathizes. “I don’t think people in Omaha thought we could ever have something that resembles New York,” he told me. “To be honest, in the spring, I would have thought it extremely unlikely.” But he adds that the Midwest has taken entirely the wrong lesson from the Northeast’s ordeal. Instead of learning that the pandemic is controllable, and that physical distancing works, people instead internalized “a mistaken belief that every curve that goes up must come down,” he said. “What they don’t realize is that if we don’t change anything about how we’re conducting ourselves, the curve can go up and up.” Speaking on Tuesday afternoon, Nebraska Governor Pete Ricketts once again refused to issue a statewide mask mandate. He promised to tighten restrictions once a quarter of the state’s beds are filled with COVID-19 patients, but even then, some restaurants will still offer indoor dining; gyms and churches will remain open; and groups of 10 people will still be able to gather in enclosed spaces. Ricketts urged Nebraskans to avoid close contact, confined areas, and crowds, but his policies nullify his pleas. “People have the mistaken belief that if the government allows them to do something, it is safe to do,” Johnson said. [Read: The pandemic safety rule that really matters] There are signs that citizens and businesses are acting ahead of policy makers. Some restaurants are ceasing indoor dining even without a prohibition. Parents are pulling their children out of schools and sports leagues. “I have heard from more friends and family about COVID-19 in the last two weeks than I have in the previous six months, expressing support and a change in attitudes,” Johnson said. But COVID-19 works slowly. It takes several days for infected people to show symptoms, a dozen more for newly diagnosed cases to wend their way to hospitals, and even more for the sickest of patients to die. These lags mean that the pandemic’s near-term future is always set, baked in by the choices of the past. It means that Ricketts is already too late to stop whatever UNMC will face in the coming weeks (but not too late to spare the hospital further grief next month). It means that some of the people who get infected over Thanksgiving will struggle to enter packed hospitals by the middle of December, and be in the ground by Christmas. Officially, Nebraska has 4,223 hospital beds, of which 1,165—27 percent—are still available. But that figure is deceptive. It includes beds for labor and deliveries, as well as pediatric beds that cannot be repurposed. It also says nothing about how stretched hospitals have already become in their efforts to create capacity. UNMC has postponed elective surgeries—those which could be deferred for four to 12 weeks. Patients with strokes and other urgent traumas aren’t getting the normal level of attention, because the pandemic is so all-consuming. Clinical research has stopped because research nurses are now COVID-19 nurses. The hospital is forced to turn down many requests to take in patients from rural hospitals and neighboring states that are themselves almost out of beds. Empty hospital beds might as well be hotel beds without doctors and nurses to staff them. And though health-care workers are resilient, “many of us feel like we haven’t had a day off since this thing began,” Hewlett says. The current surge is pushing them to the limit because people with COVID-19 are far sicker than the average patient. In an ICU, they need twice as much attention for three times the usual stay. To care for them, UNMC’s nurses and respiratory therapists are now doing mandatory overtime. The hospital has tried to hire travel nurses, but with the entire country calling for help, the pool of reinforcements is dry. “Even before COVID-19 hit, we were short-staffed,” says Becky Long, a lead nurse on a COVID ICU floor. Of late, there have been days when the hospital had 45 to 60 fewer nurses than it needed. “Every time I’ve been at work, I’ve thought: This is going to be the final straw. But somehow we continue to make it work, and I truly have no idea how.” [Read: The end of the pandemic is now in sight] Before COVID-19, Long worked in oncology. Death is no stranger to her, but she tells me she can barely comprehend the amount she has seen in recent weeks. “I used to be able to leave work at work, but with the pandemic, it follows me everywhere I go,” she said. “It’s all I see when I come home, when I look at my kids.” Long and other nurses have told many families that they can’t see their dying loved ones, and then sat with those patients so they didn’t have to die alone. Lindsay Ivener, a staff nurse, told me that COVID-19 had recently killed an elderly woman whom she was caring for, the woman’s husband, and one of her grandchildren. A second grandchild had just been admitted to the hospital with COVID-19. “It just tore this whole family apart in a month,” Ivener said. “I couldn’t even cry. I didn’t have the energy.” Until recently, Ivener worked in corporate America as a retail buyer and inventory manager. Wanting to help people, she retrained as a nurse and graduated this May. “I’ve only worked as a nurse during a pandemic,” she told me. “It’s got to get better, right?” from https://ift.tt/32ZC6MA Check out http://natthash.tumblr.com Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. For all that scientists have done to tame the biological world, there are still things that lie outside the realm of human knowledge. The coronavirus was one such alarming reminder, when it emerged with murky origins in late 2019 and found naive, unwitting hosts in the human body. Even as science began to unravel many of the virus’s mysteries—how it spreads, how it tricks its way into cells, how it kills—a fundamental unknown about vaccines hung over the pandemic and our collective human fate: Vaccines can stop many, but not all, viruses. Could they stop this one? The answer, we now know, is yes. A resounding yes. Pfizer and Moderna have separately released preliminary data that suggest their vaccines are both more than 90 percent effective, far more than many scientists expected. Neither company has publicly shared the full scope of their data, but independent clinical-trial monitoring boards have reviewed the results, and the FDA will soon scrutinize the vaccines for emergency use authorization. Unless the data take an unexpected turn, initial doses should be available in December. The tasks that lie ahead—manufacturing vaccines at scale, distributing them via a cold or even ultracold chain, and persuading wary Americans to take them—are not trivial, but they are all within the realm of human knowledge. The most tenuous moment is over: The scientific uncertainty at the heart of COVID-19 vaccines is resolved. Vaccines work. And for that, we can breathe a collective sigh of relief. “It makes it now clear that vaccines will be our way out of this pandemic,” says Kanta Subbarao, a virologist at the Doherty Institute, who has studied emerging viruses. The invention of vaccines against a virus identified only 10 months ago is an extraordinary scientific achievement. They are the fastest vaccines ever developed, by a margin of years. From virtually the day Chinese scientists shared the genetic sequence of a new coronavirus in January, researchers began designing vaccines that might train the immune system to recognize the still-unnamed virus. They needed to identify a suitable piece of the virus to turn into a vaccine, and one promising target was the spike-shaped proteins that decorate the new virus’s outer shell. Pfizer and Moderna’s vaccines both rely on the spike protein, as do many vaccine candidates still in development. These initial successes suggest this strategy works; several more COVID-19 vaccines may soon cross the finish line. To vaccinate billions of people across the globe and bring the pandemic to a timely end, we will need all the vaccines we can get. But it is no accident or surprise that Moderna and Pfizer are first out of the gate. They both bet on a new and hitherto unproven idea of using mRNA, which has the long-promised advantage of speed. This idea has now survived a trial by pandemic and emerged likely triumphant. If mRNA vaccines help end the pandemic and restore normal life, they may also usher in a new era for vaccine development. The human immune system is awesome in its power, but an untrained one does not know how to aim its fire. That’s where vaccines come in. They present a harmless snapshot of a pathogen, a “wanted” poster, if you will, that primes the immune system to recognize the real virus when it comes along. Traditionally, this snapshot could be in the form of a weakened virus or an inactivated virus or a particularly distinctive viral molecule. But those approaches require vaccine makers to manufacture viruses and their molecules, which takes time and expertise. Both are lacking during a pandemic caused by a novel virus. mRNA vaccines offer a clever shortcut. We humans don’t need to intellectually work out how to make viruses; our bodies are already very, very good at incubating them. When the coronavirus infects us, it hijacks our cellular machinery, turning our cells into miniature factories that churn out infectious viruses. The mRNA vaccine makes this vulnerability into a strength. What if we can trick our own cells into making just one individually harmless, though very recognizable, viral protein? The coronavirus’s spike protein fits this description, and the instructions for making it can be encoded into genetic material called mRNA. Both vaccines, from Moderna and from Pfizer’s collaboration with the smaller German company BioNTech, package slightly modified spike-protein mRNA inside a tiny protective bubble of fat. Human cells take up this bubble and simply follow the directions to make spike protein. The cells then display these spike proteins, presenting them as strange baubles to the immune system. Recognizing these viral proteins as foreign, the immune system begins building an arsenal to prepare for the moment a virus bearing this spike protein appears. This overall process mimics the steps of infection better than some traditional vaccines, which suggests that mRNA vaccines may provoke a better immune response for certain diseases. When you inject vaccines made of inactivated viruses or viral pieces, they can’t get inside the cell, and the cell can’t present those viral pieces to the immune system. Those vaccines can still elicit proteins called antibodies, which neutralize the virus, but they have a harder time stimulating T cells, which make up another important part of the immune response. (Weakened viruses used in vaccines can get inside cells, but risk causing an actual infection if something goes awry. mRNA vaccines cannot cause infection because they do not contain the whole virus.) Moreover, inactivated viruses or viral pieces tend to disappear from the body within a day, but mRNA vaccines can continue to produce spike protein for two weeks, says Drew Weissman, an immunologist at the University of Pennsylvania, whose mRNA vaccine research has been licensed by both BioNTech and Moderna. The longer the spike protein is around, the better for an immune response. All of this is how mRNA vaccines should work in theory. But no one on Earth, until last week, knew whether mRNA vaccines actually do work in humans for COVID-19. Although scientists had prototyped other mRNA vaccines before the pandemic, the technology was still new. None had been put through the paces of a large clinical trial. And the human immune system is notoriously complicated and unpredictable. Immunology is, as my colleague Ed Yong has written, where intuition goes to die. Vaccines can even make diseases more severe, rather than less. The data from these large clinical trials from Pfizer/BioNTech and Moderna are the first, real-world proof that mRNA vaccines protect against disease as expected. The hope, in the many years when mRNA vaccine research flew under the radar, was that the technology would deliver results quickly in a pandemic. And now it has. “What a relief,” says Barney Graham, a virologist at the National Institutes of Health, who helped design the spike protein for the Moderna vaccine. “You can make thousands of decisions, and thousands of things have to go right for this to actually come out and work. You’re just worried that you have made some wrong turns along the way.” For Graham, this vaccine is a culmination of years of such decisions, long predating the discovery of the coronavirus that causes COVID-19. He and his collaborators had homed in on the importance of spike protein in another virus, called respiratory syncytial virus, and figured out how to make the protein more stable and thus suitable for vaccines. This modification appears in both Pfizer/BioNTech’s and Moderna’s vaccines, as well as other leading vaccine candidates. The spectacular efficacy of these vaccines, should the preliminary data hold, likely also has to do with the choice of spike protein as vaccine target. On one hand, scientists were prepared for the spike protein, thanks to research like Graham’s. On the other hand, the coronavirus’s spike protein offered an opening. Three separate components of the immune system—antibodies, helper cells, and killer T cells—all respond to the spike protein, which isn’t the case with most viruses. In this, we were lucky. “It’s the three punches,” says Alessandro Sette. Working with Shane Crotty, his fellow immunologist at the La Jolla Institute, Sette found that COVID-19 patients whose immune systems can marshal all three responses against the spike protein tend to fare the best. The fact that most people can recover from COVID-19 was always encouraging news; it meant a vaccine simply needed to jump-start the immune system, which could then take on the virus itself. But no definitive piece of evidence existed that proved COVID-19 vaccines would be a slam dunk. “There’s nothing like a Phase 3 clinical trial,” Crotty says. “You don’t know what’s gonna happen with a vaccine until it happens, because the virus is complicated and the immune system is complicated.” Experts anticipate that the ongoing trials will clarify still-unanswered questions about the COVID-19 vaccines. For example, Ruth Karron, the director of the Center for Immunization Research at Johns Hopkins University, asks, does the vaccine prevent only a patient’s symptoms? Or does it keep them from spreading the virus? How long will immunity last? How well does it protect the elderly, many of whom have a weaker response to the flu vaccine? So far, Pfizer has noted that its vaccine seems to protect the elderly just as well, which is good news because they are especially vulnerable to COVID-19. Several more vaccines using the spike protein are in clinical trials too. They rely on a suite of different vaccine technologies, including weakened viruses, inactivated viruses, viral proteins, and another fairly new concept called DNA vaccines. Never before have companies tested so many different types of vaccines against the same virus, which might end up revealing something new about vaccines in general. You now have the same spike protein delivered in many different ways, Sette points out. How will the vaccines behave differently? Will they each stimulate different parts of the immune system? And which parts are best for protecting against the coronavirus? The pandemic is an opportunity to compare different types of vaccines head-on. If the two mRNA vaccines continue to be as good as they initially seem, their success will likely crack open a whole new world of mRNA vaccines. Scientists are already testing them against currently un-vaccinable viruses such as Zika or cytomegalovirus and trying to make improved versions of existing vaccines, such as for the flu. Another possibility lies in personalized mRNA vaccines that can stimulate the immune system to fight cancer. But the next few months will be a test of one potential downside of mRNA vaccines: their extreme fragility. mRNA is an inherently unstable molecule, which is why it needs that protective bubble of fat called a lipid nanoparticle. But the lipid nanoparticle itself is exquisitely sensitive to temperature. For longer-term storage, Pfizer/BioNTech’s vaccine has to be stored at –70 degrees Celsius and Moderna’s at –20 Celsius, though they can be kept at higher temperatures for a shorter amount of time. Pfizer/BioNTech and Moderna have said they can collectively supply enough doses for 22.5 million people in the United States by the end of the year. Distributing the limited vaccines fairly and smoothly will be a massive political and logistical challenge, especially as it begins during a bitter transition of power in Washington. The vaccine is a scientific triumph, but the past eight months have made clear how much pandemic preparedness is not only about scientific research. Ensuring adequate supplies of tests and personal protective equipment, providing economic relief, and communicating the known risks of COVID-19 transmission are all well within the realm of human knowledge, yet the U.S. government has failed at all of that. The vaccine by itself cannot slow the dangerous trajectory of COVID-19 hospitalizations this fall or save the many people who may die by Christmas. But it can give us hope that the pandemic will end. Every infection we prevent now—through masking and social distancing—is an infection that can, eventually, be prevented forever through vaccines. from https://ift.tt/2IMegwE Check out http://natthash.tumblr.com Coronavirus infections in the United States are growing exponentially, and lawmakers may soon face an awful choice between another round of shutdowns and the deaths of tens of thousands more Americans. A small band of scientists insist there is another way. They say that if every American took multiple coronavirus tests a week at home, we’d be able to figure out who is contagious. People who tested positive would stay home for two weeks while the rest of us more or less went about our lives. With masks and social distancing, yes—but also with safer schools and larger funerals. These rapid tests, these scientists argue, would help Americans survive until a vaccine becomes widely available next summer. A similar testing scheme conducted in Slovakia recently helped cut infections in half, Reuters reported. Other studies have suggested that testing people for symptoms, such as fevers, alone won’t stop the spread of the coronavirus, and that everyone—symptomatic or not—should be tested frequently. But the easy, cheap, at-home coronavirus tests that would make all of this possible still aren’t available to most Americans. My colleagues Robinson Meyer and Alexis C. Madrigal wrote about the promise of such testing in August. At the time, the concept had circulated for months. A handful of at-home tests are now for sale in some stores, but they cost more than $100 and take more than a day to return the results. Yesterday, the FDA approved another at-home test, Lucira, that will cost less than $50 and return results within 30 minutes. But it will be available only by prescription, NPR reported, and won’t be widely available until this spring. The types of tests scientists such as the Harvard epidemiologist Michael Mina, an advocate for the idea, are envisioning are extremely cheap—a few bucks a pop—and wouldn’t require a prescription. Mina and others suspect that at-home COVID-19 testing isn’t widely available yet because President Donald Trump and his administration haven’t tried particularly hard to make it so. “The only reason that we don’t have these out in massive numbers is that the federal government hasn’t prioritized it in any way,” Mina told me recently. Though the Lucira news is encouraging, Mina sees it as a “baby step.” He said the feds should be pumping money into the companies developing and manufacturing cheap, over-the-counter tests, and accelerating the regulatory-approval process. Simply sitting back and letting the market do its work, Mina and his allies argue, is wasting time and costing lives. The Trump administration insists that further government intervention in the testing market is neither necessary nor appropriate. But President-elect Joe Biden has a plan that includes pushing harder for rapid testing. Whether he’s able to carry it out could determine the course of the pandemic. T he most common variety of at-home rapid tests that Mina and others envision are what are called antigen tests—strips of paper that have monoclonal antibodies printed on them that attach to the virus if it’s present, turning the paper a darker color. These aren’t the polymerase-chain-reaction, or PCR, tests clinicians use to diagnose people with COVID-19. Although PCR tests look for any recent sign of the virus, antigen tests hunt for live, infectious virus. “In other words, PCR testing is like a detective at a crime scene, looking for any evidence that a crime is or was in the past few weeks committed,” Mina said. “An antigen test is more like a security guard, looking only for an actionable crime, currently being committed.” (The company Abbott has designed a rapid test called the BinaxNOW, but it is approved only for use by health-care providers. Other companies, such as Lucira, are working on at-home rapid tests that don’t rely on antigens. More on those tests later.) [Read: The pandemic safety rule that really matters] Although these rapid tests are not very sensitive to the presence of any virus, their proponents say that they catch the people who are most likely to be contagious. Think of these tests like a pregnancy test, but for COVID-19. Just like you would get a pregnancy confirmed by a doctor if you test positive, you would confirm your COVID-19 at-home antigen test either by taking a different type of antigen test or by getting tested at the doctor. “Think about the number of situations where you would love to have something like that,” says Jeff Huber, the president of OpenCovidScreen, which is running a contest for companies to invent a better COVID-19 test. “There was a death in the family and you want to have a funeral and you want people to come together, but you want to do that as safely as possible.” School, work, and even weddings could be back on—even if not everyone had been vaccinated yet. But some experts say the FDA has been slow to approve these tests. Typically, the agency approves new coronavirus tests based on how well they detect the presence of the virus—and how well they don’t erroneously flag negative cases. Rather than hold antigen tests to that standard, the FDA should approve these tests based on how well they catch people with high levels of virus in their system, Mina argues. This standard has “turned a lot of the companies off for many, many months, from even submitting anything,” Mina said. A company called E25Bio, in Cambridge, Massachusetts, has already developed such a test. It costs less than $10, and it provides results in three to 10 minutes. To use it, you swab your nose and dab the goo on a paper strip housed inside a plastic cassette. On November 10, the company told me it had an application in for approval with the FDA, and had been waiting for several weeks to hear back. Eric Topol, a cardiologist and the director of the Scripps Research Translational Institute, has gotten the sense that the FDA thinks antigen at-home tests will be too confusing for everyday people to use, and thus will lead to chaos and the erratic reporting of positive cases. In an interview with Topol for Medscape, FDA commissioner Stephen Hahn said, “it’s a whole different level with at-home tests because there won’t be a provider that’s providing information and guidance to someone who’s doing this at home. We need to make sure that they’re easy to use, easy to understand, and highly reliable.” In response to a request for comment, a spokesperson for the agency said, “The role of the FDA is to ensure the safety and efficacy of diagnostic tests when used by the intended user. In the case of at-home tests, we assure they are easy for consumers to administer and the results are clear for consumers to interpret … The FDA wants data to show that consumers can also get accurate results and interpret them.” The agency added that “a developer could opt to validate their test by demonstrating its ability to detect people who are likely infectious. However, that may be more difficult to demonstrate than the validation approach we’ve recommended because there isn’t an accepted way to measure it.” Another problem that Mina and others point to is that the Trump administration has failed to infuse money into at-home testing companies. The companies producing these antigen tests, with the exception of Abbott, are small start-ups. The government is essentially waiting for these underdogs to independently raise cash and develop tests, then weighing whether it’s willing to approve them. “If somebody was bombing us, killing even a fraction of the number of people who have died at the hands of this virus, we would not be sitting idly by and saying, I wonder who’s going to make the next crop of missiles for us to use to defend ourselves?” Mina said. The federal government, he and others argue, should be throwing money at companies to produce the tests, or possibly even building factories to produce them itself. With $20 billion, Mina argues, the government could build four factories that produce enough antigen tests to stop most outbreaks in the country. That may sound like a lot of money, but it’s just 1 percent of the COVID-19 stimulus package, the CARES Act. And after the pandemic ends, the factories could be repurposed for flu tests and other efforts. “But they haven’t done it, and I don’t know why,” Mina said. One way for the federal government to get affordable, at-home tests to Americans faster would be to use the Defense Production Act, which allows the government to prioritize the manufacturing of goods and infrastructure deemed essential to national security. Though Trump used the act occasionally throughout the pandemic, some, like Mina, say he should have been using it to ramp up at-home testing. Multiple experts shared Mina’s concern that the government has not already churned out rapid tests. “They kept saying to me, ‘We don’t want to use the [Defense Production Act]; the market will work,’” one person who is working on testing strategies and has had conversations with the Trump administration told me. But once a vaccine for the coronavirus becomes widely available, the market for the tests will diminish, if not disappear entirely. Small companies aren’t eager to put up their own capital for a type of manufacturing that won’t be useful in eight months. This person got the impression that Trump administration officials were under pressure from the White House not to use the DPA for the production of tests, only to buy up tests that are already available. In August, for instance, the Trump administration bought 150 million rapid tests from Abbott and distributed them to states, colleges, and nursing homes. Mina and his ilk argue that’s not enough—the government should become a manufacturer, and make the test printer go brrr. [Read: All the president’s lies about the coronavirus] Before the election, I asked Peter Navarro, the assistant to Trump for trade and manufacturing, whether the president planned to use the DPA for the production of at-home tests if he was reelected. “Companies along the supply chain working with Abbott understand the power of the DPA—which we have used more than 100 times—so it need not be explicitly invoked to get the desired effect,” he told me. A spokesperson for Biden’s campaign told me the president-elect plans to use the DPA to scale the production of at-home tests. Vivek Murthy, the former surgeon general under President Barack Obama, will co-chair Biden’s COVID-19 task force. In a recent interview with NPR, Murthy said, “[Biden] wants to expand our testing capacity … not just diagnostic testing, but also screening testing so that we can better open up schools and workplaces.” There are some pleas for caution on at-home tests, even among their boosters. Topol, from the Scripps Research Translational Institute, argues that we first need a large clinical trial to show that the tests are effective at stopping outbreaks. The test that does so, then, could set the standard for others like it. Other experts say that imprecise, at-home tests are a terrible idea. Michael Osterholm, the director of the Center for Infectious Disease Research and Policy at the University of Minnesota, worries that if the country is awash in tests that return too many incorrect results, people will lose confidence in testing. They might refuse to get tested, refuse to self-isolate if they test positive, or get PCR and antigen tests mixed up. After the federal government gave nursing homes some antigen rapid tests, the state of Nevada ordered the homes to stop using them once they were found to have an error rate of nearly 60 percent. Another rapid test made by the company Quidel was found to detect only 32 percent of the positive cases identified by a PCR test. (Part of the explanation for the delayed development of cheap, at-home testing might be the mixed messages experts are sending on the effectiveness of at-home tests.) Osterholm and others are concerned that if people start testing at home, positive cases might not be reported back to public-health departments. Advocates of at-home tests say they should come with apps that people can use to report their results anonymously to their local health department. The point of rapid testing is not to stop all cases, proponents argue, but to reduce how many there are. People would still have to take precautions, but they would have an extra measure of security knowing they are (likely) not contagious. What’s more, different types of tests could be used in tandem. A positive antigen test could be confirmed with a PCR test, or one antigen test could confirm a different kind of antigen test. (This type of confirmation is similar to what happens with positive HIV antibody tests.) “We don’t have enough money to do PCR in everybody, every day,” says Mara Aspinall, a biomedical-diagnostics professor at Arizona State University. In the case of a positive antigen test at a nursing home, for example, “if you have to send a nurse home for a day, before you get a central-lab PCR test, it’s a small price to pay. It’s not ideal; it’s logistically a hassle. But it’s a lot cheaper than an outbreak.” Besides, right now, we’re keeping everyone home because we don’t even know who might have the coronavirus. There is no “perfect,” these experts argue, and the alternative is bad. “Knowing more is better than knowing less,” says Paul Romer, a Nobel Prize–winning economist and an advocate for this kind of testing. To help people understand the risks of false positives and negatives, Mina said, the U.S. needs a major public-education initiative paired with the tests. People should be told what their results mean, and how to incorporate them into their already-careful lifestyles. “The NIH and the CDC should be hiring, for whatever cost it takes, Coca-Cola’s branding team,” to show people how to use the tests, Mina said. If the government remains reluctant to fund antigen tests, it could funnel money into other types of tests instead. Sherlock Biosciences, another Cambridge-based company, is working on a molecular test that’s similar to a PCR test but can be performed at home. It will be slightly more expensive—about $20 to $30 a test—but the results would still take only half an hour. But because of the challenge of getting investors to throw money at a temporary public-health risk, Sherlock will not have the tests out in wide circulation until the middle of next year. The company could get it out sooner, but that would require getting money from the federal government, CEO Rahul Dhanda told me. And so far, that money hasn’t come. Dhanda told Trump’s coronavirus task force about his company’s plans a few months ago. But “it didn’t lead to a response,” he recalled. “It just sort of fizzled. We never really heard back.” from https://ift.tt/38QwzM1 Check out http://natthash.tumblr.com
Dear Dr. Hamblin, I’m a senior who has spent considerable effort at staying out of harm’s way. My wife and I spent much of March through June at home, making quick shopping trips when needed. We are always masked when indoors in a public space, but we do get within six feet of others when grocery shopping or eating outdoors with a few friends. Surely we have been exposed, at least slightly, to low quantities of the coronavirus over the course of the pandemic. Even if we don’t get sick, is our immune system activated? Can we develop antibodies through repeated low-dose exposures? Richard Clark Friendswood, Texas Richard, That’s the dream scenario: building up immunity without getting sick. The short answer is that it’s possible. The long answer is that it’s not very likely. At least not yet. Many people have tested positive for antibodies, to their surprise, without having had symptoms or known contact with an infected person. It seems clear that you don’t even need repeated low-dose exposures to the coronavirus to develop antibodies. A single exposure could do it. Unfortunately, immunity is rarely so simple. The dream scenario probably does occur occasionally. But although many people have tested positive for antibodies without getting sick (or, at least, without getting seriously sick), that doesn’t mean they’re immune. The main issue is that not all coronavirus antibodies are the same. Some antibodies latch onto the virus, but won’t stop its spread. Detecting these types in someone’s blood can tell you that that person has been exposed to the virus, but not that they’re immune. Other antibodies, known as neutralizing antibodies, go right for the virus’s Achilles’ heel. They bind to the spike proteins on its surface, the grappling hooks that it uses to latch onto human cells. By taking out those spikes, they render the virus incapable of spreading within the body and causing disease. Only some people who test positive for antibodies have neutralizing antibodies. Most current antibody tests can’t tell the difference. Only last week did the U.S. Food and Drug Administration give emergency-use authorization for the first test that singles out neutralizing antibodies. [Read: Should you get an antibody test?] Neutralizing antibodies seem to be less common after an asymptomatic infection than after a serious case of COVID-19. Whatever antibodies do develop in those cases seem to fade more quickly, too. So a brief exposure to a tiny amount of virus in a grocery store may be enough to turn your antibody test positive, but it seems less likely to confer meaningful, lasting protection than if you’d had a serious case of COVID-19. The degree to which the severity of COVID-19 is related to the types of antibodies that develop remains unclear, and we can expect outliers of all sorts to be reported. But don’t mistake a single report of a person who had tons of protective antibodies without ever getting sick for the norm. For now, no one should behave any differently just because they’ve had a positive antibody test. We still need to get better at deciphering which antibodies people have—and how many are needed to confer immunity—before we can assure them that they are protected. All of these variables are why vaccination is so complex, and usually takes many years to get right. The goal is to create that dream scenario you described: to stimulate people’s immune system into developing neutralizing antibodies that last, and to do so without causing side effects. Threading that needle is always a challenge, but especially with a virus like this one, which affects people in such different ways. That’s why this month’s news of the apparent effectiveness of the Pfizer and Moderna vaccines--90 percent and 95 percent, respectively, according to preliminary data—was so surprising. Even more amazing will be if the number stays that high over time, and no significant side effects are reported. But it looks as if, once clinical trials are complete, we should have a vaccine that can reliably deliver that dream scenario: a protective immune response without ever getting sick, or even infected. The bottom line is that your question is an interesting academic one, but the answer shouldn’t change anyone’s day-to-day life. In reality, most infected people have at least some symptoms, and many get extremely sick. More than 1,000 Americans are dying each day. Many others are developing chronic disease. There’s no reason to assume that low-level exposure to the virus is beneficial. Flirting with mild exposure is not something to even consider doing deliberately. Even if you didn’t get sick, you could become an asymptomatic carrier and spread the virus, infecting and potentially killing other people. And you’d probably have no immunity to show for it. “Paging Dr. Hamblin” is for informational purposes only, does not constitute medical advice, and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. By submitting a letter, you are agreeing to let The Atlantic use it—in part or in full—and we may edit it for length and/or clarity. from https://ift.tt/2UDWUok Check out http://natthash.tumblr.com Photographs by Julia Sellmann Every few weeks or so, Grete Fält-Hansen gets a call from a stranger asking a question for the first time: What is it like to raise a child with Down syndrome? Sometimes the caller is a pregnant woman, deciding whether to have an abortion. Sometimes a husband and wife are on the line, the two of them in agonizing disagreement. Once, Fält-Hansen remembers, it was a couple who had waited for their prenatal screening to come back normal before announcing the pregnancy to friends and family. “We wanted to wait,” they’d told their loved ones, “because if it had Down syndrome, we would have had an abortion.” They called Fält-Hansen after their daughter was born—with slanted eyes, a flattened nose, and, most unmistakable, the extra copy of chromosome 21 that defines Down syndrome. They were afraid their friends and family would now think they didn’t love their daughter—so heavy are the moral judgments that accompany wanting or not wanting to bring a child with a disability into the world. All of these people get in touch with Fält-Hansen, a 54-year-old schoolteacher, because she heads Landsforeningen Downs Syndrom, or the National Down Syndrome Association, in Denmark, and because she herself has an 18-year-old son, Karl Emil, with Down syndrome. Karl Emil was diagnosed after he was born. She remembers how fragile he felt in her arms and how she worried about his health, but mostly, she remembers, “I thought he was so cute.” Two years after he was born, in 2004, Denmark became one of the first countries in the world to offer prenatal Down syndrome screening to every pregnant woman, regardless of age or other risk factors. Nearly all expecting mothers choose to take the test; of those who get a Down syndrome diagnosis, more than 95 percent choose to abort. Denmark is not on its surface particularly hostile to disability. People with Down syndrome are entitled to health care, education, even money for the special shoes that fit their wider, more flexible feet. If you ask Danes about the syndrome, they’re likely to bring up Morten and Peter, two friends with Down syndrome who starred in popular TV programs where they cracked jokes and dissected soccer games. Yet a gulf seems to separate the publicly expressed attitudes and private decisions. Since universal screening was introduced, the number of children born with Down syndrome has fallen sharply. In 2019, only 18 were born in the entire country. (About 6,000 children with Down syndrome are born in the U.S. each year.) Fält-Hansen is in the strange position of leading an organization likely to have fewer and fewer new members. The goal of her conversations with expecting parents, she says, is not to sway them against abortion; she fully supports a woman’s right to choose. These conversations are meant to fill in the texture of daily life missing both from the well-meaning cliché that “people with Down syndrome are always happy” and from the litany of possible symptoms provided by doctors upon diagnosis: intellectual disability, low muscle tone, heart defects, gastrointestinal defects, immune disorders, arthritis, obesity, leukemia, dementia. She might explain that, yes, Karl Emil can read. His notebooks are full of poetry written in his careful, sturdy handwriting. He needed physical and speech therapy when he was young. He loves music—his gold-rimmed glasses are modeled after his favorite Danish pop star’s. He gets cranky sometimes, like all teens do. One phone call might stretch into several; some people even come to meet her son. In the end, some join the association with their child. Others, she never hears from again. These parents come to Fält-Hansen because they are faced with a choice—one made possible by technology that peers at the DNA of unborn children. Down syndrome is frequently called the “canary in the coal mine” for selective reproduction. It was one of the first genetic conditions to be routinely screened for in utero, and it remains the most morally troubling because it is among the least severe. It is very much compatible with life—even a long, happy life. 
The forces of scientific progress are now marching toward ever more testing to detect ever more genetic conditions. Recent advances in genetics provoke anxieties about a future where parents choose what kind of child to have, or not have. But that hypothetical future is already here. It’s been here for an entire generation. [Read: ‘I am a man with Down syndrome and my life is worth living’] Fält-Hansen says the calls she receives are about information, helping parents make a truly informed decision. But they are also moments of seeking, of asking fundamental questions about parenthood. Do you ever wonder, I asked her, about the families who end up choosing an abortion? Do you feel like you failed to prove that your life—and your child’s life—is worth choosing? She told me she doesn’t think about it this way anymore. But in the beginning, she said, she did worry: “What if they don’t like my son?” ••• In January, I took a train from Copenhagen south to the small town of Vordingborg, where Grete, Karl Emil, and his 30-year-old sister, Ann Katrine Kristensen, met me at the station. The three of them formed a phalanx of dark coats waving hello. The weather was typical of January—cold, gray, blustery—but Karl Emil pulled me over to the ice-cream shop, where he wanted to tell me he knew the employees. His favorite ice-cream flavor, he said, was licorice. “That’s very Danish!” I said. Grete and Ann Katrine translated. Then he zagged over to a men’s clothing store and struck up a conversation with the clerk, who had just seen Karl Emil interviewed on a Danish children’s program with his girlfriend, Chloe. “You didn’t tell me you had a girlfriend,” the clerk teased. Karl Emil laughed, mischievous and proud. We sat down at a café, and Grete gave her phone to Karl Emil to busy himself with while we spoke in English. He took selfies; his mother, sister, and I began to talk about Down syndrome and the country’s prenatal-screening program. At one point, Grete was reminded of a documentary that had sparked an outcry in Denmark. She reclaimed her phone to look up the title: Død Over Downs (“Death to Down Syndrome”). When Karl Emil read over her shoulder, his face crumpled. He curled into the corner and refused to look at us. He had understood, obviously, and the distress was plain on his face. Grete looked up at me: “He reacts because he can read.” “He must be aware of the debate?” I asked, which felt perverse to even say. So he’s aware there are people who don’t want people like him to be born? Yes, she said; her family has always been open with him. As a kid, he was proud of having Down syndrome. It was one of the things that made him uniquely Karl Emil. But as a teenager, he became annoyed and embarrassed. He could tell he was different. “He actually asked me, at some point, if it was because of Down syndrome that he sometimes didn’t understand things,” Grete said. “I just told him honestly: Yes.” As he’s gotten older, she said, he’s made his peace with it. This arc felt familiar. It’s the arc of growing up, in which our self-assuredness as young children gets upended in the storms of adolescence, but eventually, hopefully, we come to accept who we are. The decisions parents make after prenatal testing are private and individual ones. But when the decisions so overwhelmingly swing one way—to abort—it does seem to reflect something more: an entire society’s judgment about the lives of people with Down syndrome. That’s what I saw reflected in Karl Emil’s face. Denmark is unusual for the universality of its screening program and the comprehensiveness of its data, but the pattern of high abortion rates after a Down syndrome diagnosis holds true across Western Europe and, to a somewhat lesser extent, in the United States. In wealthy countries, it seems to be at once the best and the worst time for Down syndrome. Better health care has more than doubled life expectancy. Better access to education means most children with Down syndrome will learn to read and write. Few people speak publicly about wanting to “eliminate” Down syndrome. Yet individual choices are adding up to something very close to that. 
In the 1980s, as prenatal screening for Down syndrome became common, the anthropologist Rayna Rapp described the parents on the frontier of reproductive technology as “moral pioneers.” Suddenly, a new power was thrust into the hands of ordinary people—the power to decide what kind of life is worth bringing into the world. The medical field has also been grappling with its ability to offer this power. “If no one with Down syndrome had ever existed or ever would exist—is that a terrible thing? I don’t know,” says Laura Hercher, a genetic counselor and the director of student research at Sarah Lawrence College. If you take the health complications linked to Down syndrome, such as increased likelihood of early-onset Alzheimer’s, leukemia, and heart defects, she told me, “I don’t think anyone would argue that those are good things.” But she went on. “If our world didn’t have people with special needs and these vulnerabilities,” she asked, “would we be missing a part of our humanity?” ••• Sixty-one years ago, the first known prenatal test for a genetic disorder in the world took place in Copenhagen. The patient was a 27-year-old woman who was a carrier for hemophilia, a rare and severe bleeding disorder that is passed from mothers to sons. She had already given birth to one infant boy, who lived for just five hours. The obstetrician who delivered the baby, Fritz Fuchs, told her to come back if she ever became pregnant again. And in 1959, according to the published case study, she did come back, saying she couldn’t go through with her pregnancy if she was carrying another son. Fuchs had been thinking about what to do. Along with a cytologist named Povl Riis, he’d been experimenting with using fetal cells floating in the yellow amniotic fluid that fills the womb to determine a baby’s sex. A boy would have a 50 percent risk of inheriting hemophilia; a girl would have almost no risk. But first they needed some amniotic fluid. Fuchs eased a long needle into the woman’s abdomen; Riis studied the cells under a microscope. It was a girl. The woman gave birth to a daughter a few months later. If the baby had been a boy, though, she was prepared to have an abortion—which was legal under Danish law at the time on “eugenic grounds” for fetuses at risk for severe mental or physical illness, according to Riis and Fuchs’s paper describing the case. They acknowledged the possible danger of sticking a needle in the abdomen of a pregnant woman, but wrote that it was justified “because the method seems to be useful in preventive eugenics.” That word, eugenics, today evokes images that are specific and heinous: forced sterilization of the “feebleminded” in early-20th-century America, which in turn inspired the racial hygiene of the Nazis, who gassed or otherwise killed tens of thousands of people with disabilities, many of them children. But eugenics was once a mainstream scientific pursuit, and eugenicists believed that they were bettering humanity. Denmark, too, drew inspiration from the U.S., and it passed a sterilization law in 1929. Over the next 21 years, 5,940 people were sterilized in Denmark, the majority because they were “mentally retarded.” Those who resisted sterilization were threatened with institutionalization. Eugenics in Denmark never became as systematic and violent as it did in Germany, but the policies came out of similar underlying goals: improving the health of a nation by preventing the birth of those deemed to be burdens on society. The term eugenics eventually fell out of favor, but in the 1970s, when Denmark began offering prenatal testing for Down syndrome to mothers over the age of 35, it was discussed in the context of saving money—as in, the testing cost was less than that of institutionalizing a child with a disability for life. The stated purpose was “to prevent birth of children with severe, lifelong disability.” That language too has long since changed; in 1994, the stated purpose of the testing became “to offer women a choice.” Activists like Fält-Hansen have also pushed back against the subtle and not-so-subtle ways that the medical system encourages women to choose abortion. Some Danish parents told me that doctors automatically assumed they would want to schedule an abortion, as if there was really no other option. This is no longer the case, says Puk Sandager, a fetal-medicine specialist at Aarhus University Hospital. Ten years ago, doctors—especially older doctors—were more likely to expect parents to terminate, she told me. “And now we do not expect anything.” The National Down Syndrome Association has also worked with doctors to alter the language they use with patients—“probability” instead of “risk,” “chromosome aberration” instead of “chromosome error.” And, of course, hospitals now connect expecting parents with people like Fält-Hansen to have those conversations about what it’s like to raise a child with Down syndrome. [Pepper Stetler: The gap between my daughter and her peers is growing] Perhaps all of this has had some effect, though it’s hard to say. The number of babies born to parents who chose to continue a pregnancy after a prenatal diagnosis of Down syndrome in Denmark has ranged from zero to 13 a year since universal screening was introduced. In 2019, there were seven. (Eleven other babies were born to parents who either declined the test or got a false negative, making the total number of babies born with Down syndrome last year 18.) Why so few? “Looking at it from the outside, a country like Denmark, if you want to raise a child with Down syndrome, this is a good environment,” says Stina Lou, an anthropologist who has studied how parents make decisions after a prenatal diagnosis of a fetal anomaly. Since 2011, she has embedded in the fetal-medicine unit at Aarhus University Hospital, one of the largest hospitals in Denmark, where she has shadowed Sandager and other doctors. Under the 2004 guidelines, all pregnant women in Denmark are offered a combined screening in the first trimester, which includes blood tests and an ultrasound. These data points, along with maternal age, are used to calculate the odds of Down syndrome. The high-probability patients are offered a more invasive diagnostic test using DNA either from the fetal cells floating in the amniotic fluid (amniocentesis) or from placental tissue (chorionic villus sampling). Both require sticking a needle or catheter into the womb and come with a small risk of miscarriage. More recently, hospitals have started offering noninvasive prenatal testing, which uses fragments of fetal DNA floating in the mother’s blood. That option has not become popular in Denmark, though, probably because the invasive tests can pick up a suite of genetic disorders in addition to Down syndrome. More diseases ruled out, more peace of mind. But Lou was interested in the times when the tests did not provide peace of mind, when they in fact provided the opposite. In a study of 21 women who chose abortion after a prenatal diagnosis of Down syndrome, she found that they had tended to base their decisions on worst-case scenarios. An extra copy of chromosome 21 can cause a variety of symptoms, the severity of which is not known until birth or even later. Most people with Down syndrome learn to read and write. Others are nonverbal. Some do not have heart defects. Others spend months or even years in and out of the hospital to fix a heart valve. Most have healthy digestive systems. Others lack the nerve endings needed to anticipate bowel movements, necessitating more surgeries, possibly even a stoma bag or diapers. The women who chose abortion feared the worst possible outcomes. Some even grieved the possibility of aborting a child who might have had a mild form of Down syndrome. But in the end, Lou told me, “the uncertainty just becomes too much.” 
This emphasis on uncertainty came up when I spoke with David Wasserman, a bioethicist at the U.S. National Institutes of Health who, along with his collaborator Adrienne Asch, has written some of the most pointed critiques of selective abortion. (Asch died in 2013.) They argued that prenatal testing has the effect of reducing an unborn child to a single aspect—Down syndrome, for example—and making parents judge the child’s life on that alone. Wasserman told me he didn’t think that most parents who make these decisions are seeking perfection. Rather, he said, “there’s profound risk aversion.” It’s hard to know for sure whether the people in Lou’s study decided to abort for the reasons they gave or if these were retrospective justifications. But when Lou subsequently interviewed parents who had made the unusual choice to continue a pregnancy after a Down syndrome diagnosis, she found them more willing to embrace uncertainty. Parents of children with Down syndrome have described to me the initial process of mourning the child they thought they would have: the child whom they were going to walk down the aisle, who was going to graduate from college, who was going to become president. None of this is guaranteed with any kid, of course, but while most parents go through a slow realignment of expectations over the years, prenatal testing was a rapid plummet into disappointment—all those dreams, however unrealistic, evaporating at once. And then the doctors present you with a long list of medical conditions associated with Down syndrome. Think about it this way, Karl Emil’s sister, Ann Katrine, said: “If you handed any expecting parent a whole list of everything their child could possibly encounter during their entire life span—illnesses and stuff like that—then anyone would be scared.” “Nobody would have a baby,” Grete said. ••• A peculiar effect of Denmark’s universal-screening program and high abortion rate for Down syndrome is that a fair number of babies born with Down syndrome are born to parents who essentially got a false negative. Their first-trimester screening results said their odds were very low—so low that they needed no invasive follow-up testing. They simply went on with what they thought was an ordinary pregnancy. In other words, like the couple Grete once counseled, these are parents who might have chosen to abort, had they known. The day after I met Grete, I attended a meeting of the local Copenhagen Down syndrome group. The woman who invited me, Louise Aarsø, had a then-5-year-old daughter with Down syndrome, Elea. Aarsø and her husband had made the unusual choice to opt out of screening. Though they support the right to abortion, they knew they would want to have the baby either way. At the meeting, two of the seven other families told me their prenatal screening had suggested extremely low odds. At birth, they were surprised. A few others said they had chosen to continue the pregnancy despite a high probability for Down syndrome. Ulla Hartmann, whose son Ditlev was 18, noted that he was born before the national screening program began. “We’re very thankful we didn’t know, because we had two twin boys when I got pregnant with Ditlev and I really don’t think we would have been, ‘Okay, let’s take this challenge when we have these monkeys up in the curtains,’ ” she told me. “But you grow with the challenge.” Daniel Christensen was one of the parents who had been told the odds of Down syndrome were very low, something like 1 in 1,500. He and his wife didn’t have to make a choice, and when he thinks back on it, he said, “what scares me the most is actually how little we knew about Down syndrome.” What would the basis of their choice have been? Their son August is 4 now, with a twin sister, who Christensen half-jokingly said was “almost normal.” The other parents laughed. “Nobody’s normal,” he said. Then the woman to my right spoke; she asked me not to use her name. She wore a green blouse, and her blond hair was pulled into a ponytail. When we all turned to her, I noticed that she had begun to tear up. “Now I’m moved from all the stories; I’m a little …” She paused to catch her breath. “My answer is not that beautiful.” The Down syndrome odds for her son, she said, were 1 in 969. “You remember the exact number?” I asked. “Yeah, I do. I went back to the papers.” The probability was low enough that she didn’t think about it after he was born. “On the one hand I saw the problems. And on the other hand he was perfect.” It took four months for him to get diagnosed with Down syndrome. He is 6 now, and he cannot speak. It frustrates him, she said. He fights with his brother and sister. He bites because he cannot express himself. “This has just been so many times, and you never feel safe.” Her experience is not representative of all children with Down syndrome; lack of impulse control is common, but violence is not. Her point, though, was that the image of a happy-go-lucky child so often featured in the media is not always representative either. She wouldn’t have chosen this life: “We would have asked for an abortion if we knew.” Another parent chimed in, and the conversation hopscotched to a related topic and then another until it had moved on entirely. At the end of the meeting, as others stood and gathered their coats, I turned to the woman again because I was still shocked that she was willing to say what she’d said. Her admission seemed to violate an unspoken code of motherhood. Of course, she said, “it’s shameful if I say these things.” She loves her child, because how can a mother not? “But you love a person that hits you, bites you? If you have a husband that bites you, you can say goodbye … but if you have a child that hits you, you can’t do anything. You can’t just say, ‘I don’t want to be in a relationship.’ Because it’s your child.” To have a child is to begin a relationship that you cannot sever. It is supposed to be unconditional, which is perhaps what most troubles us about selective abortion—it’s an admission that the relationship can in fact be conditional. ••• Parenting is a plunge into the unknown and the uncontrollable. It is beautiful in this way, but also daunting. In the cold, scientific realm of biology, reproduction begins with a random genetic shuffling—an act of fate, if you were to be less cold, more poetic. The 23 pairs of chromosomes in our cells line up so that the DNA we inherited from our mother and father can be remixed and divided into sets of 23 single chromosomes. Each egg or sperm gets one such set. In women, this chromosomal division begins, remarkably, when they themselves are fetuses in their mother’s womb. The chromosomes freeze in place for 20, 30, even 40-plus years as the fetus becomes a baby, a girl, a woman. The cycle finishes only when the egg is fertilized. During the intervening years, the proteins holding chromosomes together can degrade, resulting in eggs with too many or too few chromosomes. This is the biological mechanism behind most cases of Down syndrome—95 percent of people born with an extra copy of chromosome 21 inherited it from their mother. And this is why the syndrome is often, though not always, linked to the age of the mother. 
In the interviews I’ve conducted, and in interviews Lou and researchers across the U.S. have conducted, the choice of what to do after a prenatal test fell disproportionately on mothers. There were fathers who agonized over the choice too, but mothers usually bore most of the burden. There is a feminist explanation (my body, my choice) and a less feminist one (family is still primarily the domain of women), but it’s true either way. And in making these decisions, many of the women seemed to anticipate the judgment they would face. Lou told me she had wanted to interview women who chose abortion after a Down syndrome diagnosis because they’re a silent majority. They are rarely interviewed in the media, and rarely willing to be interviewed. Danes are quite open about abortion—astonishingly so to my American ears—but abortions for a fetal anomaly, and especially Down syndrome, are different. They still carry a stigma. “I think it’s because we as a society like to think of ourselves as inclusive,” Lou said. “We are a rich society, and we think it’s important that different types of people should be here.” And for some of the women who end up choosing abortion, “their own self-understanding is a little shaken, because they have to accept they aren’t the kind of person like they thought,” she said. They were not the type of person who would choose to have a child with a disability. For the women in Lou’s study, ending a pregnancy after a prenatal diagnosis was very different from ending an unwanted pregnancy. These were almost all wanted pregnancies, in some cases very much wanted pregnancies following long struggles with infertility. The decision to abort was not taken lightly. One Danish woman I’ll call “L” told me how terrible it was to feel her baby inside her once she’d made the decision to terminate. In the hospital bed, she began sobbing so hard, the staff had difficulty sedating her. The depth of her emotions surprised her, because she was so sure of her decision. The abortion was two years ago, and she doesn’t think about it much anymore. But recounting it on the phone, she began crying again. She was disappointed to find so little in the media about the experiences of women like her. “It felt right for me, and I have no regrets at all,” she told me, but it also feels like “you’re doing something wrong.” L is a filmmaker, and she wanted to make a documentary about choosing abortion after a Down syndrome diagnosis. She even thought she would share her own story. But she hadn’t been able to find a couple willing to be in this documentary, and she wasn’t ready to put herself out there alone. When Rayna Rapp, the anthropologist who coined the term moral pioneers, interviewed parents undergoing prenatal testing in New York in the 1980s and ’90s, she noticed a certain preoccupation among certain women. Her subjects represented a reasonably diverse slice of the city, but middle-class white women especially seemed fixated on the idea of “selfishness.” The women she interviewed were among the first in their families to forgo homemaking for paid work; they had not just jobs but careers that were central to their identity. With birth control, they were having fewer children and having them later. They had more reproductive autonomy than women had ever had in human history. (Rapp herself came to this research after having an abortion because of Down syndrome when she became pregnant as a 36-year-old professor.) “Medical technology transforms their ‘choices’ on an individual level, allowing them, like their male partners, to imagine voluntary limits to their commitments to their children,” Rapp wrote in her book Testing Women, Testing the Fetus. But exercising those “voluntary limits” on motherhood—choosing not to have a child with a disability out of fear for how it might affect one’s career, for example—becomes judged as “selfishness.” Medical technology can offer women a choice, but it does not instantly transform the society around them. It does not dismantle the expectation that women are the primary caregivers or erase the ideal of a good mother as one who places no limits on her devotion to her children. The centrality of choice to feminism also brings it into uncomfortable conflict with the disability-rights movement. Anti-abortion-rights activists in the U.S. have seized on this to introduce bills banning selective abortion for Down syndrome in several states. Feminist disability scholars have attempted to resolve the conflict by arguing that the choice is not a real choice at all. “The decision to abort a fetus with a disability even because it ‘just seems too difficult’ must be respected,” Marsha Saxton, the director of research at the World Institute on Disability, wrote in 1998. But Saxton calls it a choice made “under duress,” arguing that a woman faced with this decision is still constrained today—by popular misconceptions that make life with a disability out to be worse than it actually is and by a society that is hostile to people with disabilities. [Pasquale Toscano and Alexis Doyle: Selective-abortion bans treat disability as a tragedy] And when fewer people with disabilities are born, it becomes harder for the ones who are born to live a good life, argues Rosemarie Garland-Thomson, a bioethicist and professor emerita at Emory University. Fewer people with disabilities means fewer services, fewer therapies, fewer resources. But she also recognizes how this logic pins the entire weight of an inclusive society on individual women. 
was introduced in 2004, the number of children in the country born with the syndrome has fallen sharply. In 2019, it was just 18. (Julia Sellmann) No wonder, then, that “choice” can feel like a burden. In one small study of women in the U.S. who chose abortion after a diagnosis of a fetal anomaly, two-thirds said they’d hoped—or even prayed—for a miscarriage instead. It’s not that they wanted their husbands, their doctors, or their lawmakers to tell them what to do, but they recognized that choice comes with responsibility and invites judgment. “I have guilt for not being the kind of person who could parent this particular type of special need,” said one woman in the study. “Guilt, guilt, guilt.” The introduction of a choice reshapes the terrain on which we all stand. To opt out of testing is to become someone who chose to opt out. To test and end a pregnancy because of Down syndrome is to become someone who chose not to have a child with a disability. To test and continue the pregnancy after a Down syndrome diagnosis is to become someone who chose to have a child with a disability. Each choice puts you behind one demarcating line or another. There is no neutral ground, except perhaps in hoping that the test comes back negative and you never have to choose what’s next. What kind of choice is this, if what you hope is to not have to choose at all? ••• Down syndrome is unlikely to ever disappear from the world completely. As women wait longer to have children, the incidence of pregnancies with an extra copy of chromosome 21 is going up. Prenatal testing can also in rare cases be wrong, and some parents will choose not to abort or not to test at all. Others will not have access to abortion. In the United States—which has no national health-care system, no government mandate to offer prenatal screening—the best estimate for the termination rate after a diagnosis of Down syndrome is 67 percent. But that number conceals stark differences within the country. One study found higher rates of termination in the West and Northeast and among mothers who are highly educated. “On the Upper East Side of Manhattan, it’s going to be completely different than in Alabama,” said Laura Hercher, the genetic counselor. These differences worry Hercher. If only the wealthy can afford to routinely screen out certain genetic conditions, then those conditions can become proxies of class. They can become, in other words, other people’s problems. Hercher worries about an empathy gap in a world where the well-off feel insulated from sickness and disability. For those with the money, the possibilities of genetic selection are expanding. The leading edge is preimplantation genetic testing (PGT) of embryos created through in vitro fertilization, which altogether can cost tens of thousands of dollars. Labs now offer testing for a menu of genetic conditions—most of them rare and severe conditions such as Tay-Sachs disease, cystic fibrosis, and phenylketonuria—allowing parents to select healthy embryos for implantation in the womb. Scientists have also started trying to understand more common conditions that are influenced by hundreds or even thousands of genes: diabetes, heart disease, high cholesterol, cancer, and—much more controversially—mental illness and autism. In late 2018, Genomic Prediction, a company in New Jersey, began offering to screen embryos for risk of hundreds of conditions, including schizophrenia and intellectual disability, though it has since quietly backtracked on the latter. The one test customers keep asking for, the company’s chief scientific officer told me, is for autism. The science isn’t there yet, but the demand is. The politics of prenatal testing for Down syndrome and abortion are currently yoked together by necessity: The only intervention offered for a prenatal test that finds Down syndrome is an abortion. But modern reproduction is opening up more ways for parents to choose what kind of child to have. PGT is one example. Sperm banks, too, now offer detailed donor profiles delineating eye color, hair color, education; they also screen donors for genetic disorders. Several parents have sued sperm banks after discovering that their donor may have undesirable genes, in cases where their children developed conditions such as autism or a degenerative nerve disease. In September, the Georgia Supreme Court ruled that one such case, in which a sperm donor had hidden his history of mental illness, could move forward. The “deceptive trade practices” of a sperm bank that misrepresented its donor-screening process, the court ruled, could “essentially amount to ordinary consumer fraud.” 
Garland-Thomson calls this commercialization of reproduction “velvet eugenics”--velvet for the soft, subtle way it encourages the eradication of disability. Like the Velvet Revolution from which she takes the term, it’s accomplished without overt violence. But it also takes on another connotation as human reproduction becomes more and more subject to consumer choice: velvet, as in quality, high-caliber, premium-tier. Wouldn’t you want only the best for your baby—one you’re already spending tens of thousands of dollars on IVF to conceive? “It turns people into products,” Garland-Thomson says. ••• None of this suggests that testing should be entirely abandoned. Most parents choosing genetic testing are seeking to spare their children real physical suffering. Tay-Sachs disease, for example, is caused by mutations in the HEXA gene, which causes the destruction of neurons in the brain and spinal cord. At about three to six months old, babies begin losing motor skills, then their vision and hearing. They develop seizures and paralysis. Most do not live past childhood. There is no cure. In the world of genetic testing, Tay-Sachs is a success story. It has been nearly eliminated through a combination of prenatal testing of fetuses; preimplantation testing of embryos; and, in the Ashkenazi Jewish population, where the mutation is especially prevalent, carrier screening to discourage marriages between people who might together pass on the mutation. The flip side of this success is that having a baby with the disease is no longer simple misfortune because nothing could have been done. It can be seen instead as a failure of personal responsibility. Fertility doctors have spoken to me passionately about expanding access to IVF for parents who are fertile but who might use embryo screening to prevent passing on serious diseases. In a world where IVF becomes less expensive and less hard on a woman’s body, this might very well become the responsible thing to do. And if you’re already going through all this to screen for one disease, why not avail yourself of the whole menu of tests? The hypothetical that Karl Emil’s sister imagined, in which a child’s every risk is laid out, feels closer than ever. How do you choose between one embryo with a slightly elevated risk of schizophrenia and another with a moderate risk of breast cancer? Not surprisingly, those advocating for preimplantation genetic testing prefer to keep the conversation focused on monogenic diseases, where single gene mutations have severe health effects. Talk of minimizing the risk of conditions like diabetes and mental illness—which are also heavily influenced by environment—quickly turns to designer babies. “Why do we want to go there?” says David Sable, a former IVF doctor who is now a venture capitalist specializing in life sciences. “Start with the most scientifically straightforward, the monogenic diseases—cystic fibrosis, sickle cell anemia, hemophilia—where you could define very specifically what the benefit is.” What about Down syndrome, then, I asked, which can be much less severe than those diseases but is routinely screened for anyway? His answer surprised me, considering that he has spent much of his career working with labs that count chromosomes: “The concept of counting chromosomes as a definitive indicator of the truth—I think we’re going to look back on that and say, ‘Oh my God, we were so misguided.’ ” Consider the sex chromosomes, he said. “We’ve locked ourselves into this male-female binary that we enforced with XX and XY.” But it’s not nearly so neat. Babies born XX can have male reproductive organs; those born XY can have female reproductive organs. And others can be born with an unusual number of sex chromosomes like X, XXY, XYY, XXYY, XXXX, the effects of which range widely in severity. Some might never know there’s anything unusual in their chromosomes at all. When Rayna Rapp was researching prenatal testing back in the ’80s and ’90s, she came across multiple sets of parents who chose to abort a fetus with a sex-chromosome anomaly out of fear that it could lead to homosexuality—never mind that there is no known link. They also worried that a boy who didn’t conform to XY wouldn’t be masculine enough. Reading about their anxieties 30 years later, I could sense how much the ground had moved under our feet. Of course, some parents might still have the same fears, but today the boundaries of “normal” for gender and sexuality encompass much more than the narrow band of three decades ago. A child who is neither XX nor XY can fit into today’s world much more easily than in a rigidly gender-binary one. Both sex-chromosome anomalies and Down syndrome were early targets of prenatal testing—not because they are the most dangerous conditions but because they were the easiest to test for. It’s just counting chromosomes. As science moves past this relatively rudimentary technique, Sable mused, “the term Down syndrome is probably going to go away at some point, because we may find that having that third 21 chromosome maybe does not carry a predictable level of suffering or altered function.” Indeed, most pregnancies with a third copy of chromosome 21 end as miscarriages. Only about 20 percent survive to birth, and the people who are born have a wide range of intellectual disabilities and physical ailments. How can an extra chromosome 21 be incompatible with life in some cases and in other cases result in a boy, like one I met, who can read and write and perform wicked juggling tricks with his diabolo? Clearly, something more than just an extra chromosome is going on. As genetic testing has become more widespread, it has revealed just how many other genetic anomalies many of us live with—not only extra or missing chromosomes, but whole chunks of chromosome getting deleted, chunks duplicated, chunks stuck onto a different chromosome altogether, mutations that should be deadly but that show up in the healthy adult in front of you. Every person carries a set of mutations unique to them. This is why new and rare genetic diseases are so hard to diagnose—if you compare a person’s DNA with a reference genome, you come up with hundreds of thousands of differences, most of them utterly irrelevant to the disease. What, then, is normal? Genetic testing, as a medical service, is used to enforce the boundaries of “normal” by screening out the anomalous, but seeing all the anomalies that are compatible with life might actually expand our understanding of normal. “It’s expanded mine,” Sable told me. 
Sable offered this up as a general observation. He didn’t think he was qualified to speculate on what this meant for the future of Down syndrome screening, but I found this conversation about genetics unexpectedly resonant with something parents had told me. David Perry, a writer in Minnesota whose 13-year-old son has Down syndrome, said he disliked how people with Down syndrome are portrayed as angelic and cute; he found it flattening and dehumanizing. He pointed instead to the way the neurodiversity movement has worked to bring autism and ADHD into the realm of normal neurological variation. “We need more kinds of normal,” another father, Johannes Dybkjær Andersson, a musician and creative director in Copenhagen, said. “That’s a good thing, when people show up in our lives”—as his daughter, Sally, did six years ago—“and they are just normal in a totally different way.” Her brain processes the world differently than his does. She is unfiltered and open. Many parents have told me how this quality can be awkward or disruptive at times, but it can also break the stifling bounds of social propriety. Stephanie Meredith, the director of the National Center for Prenatal and Postnatal Resources at the University of Kentucky, told me of the time her 20-year-old son saw his sister collide with another player on the basketball court. She hit the ground so hard that an audible crack went through the gym. Before Meredith could react, her son had already leapt from the bleachers and picked his sister up. “He wasn’t worried about the rules; he wasn’t worried about decorum. It was just responding and taking care of her,” Meredith told me. She had recently been asked a simple but probing question: What was she most proud of about her son that was not an achievement or a milestone? The incident on the basketball court was one that came to mind. “It doesn’t have to do with accomplishment,” she said. “It has to do with caring about another human being.” That question had stayed with Meredith—and it stayed with me—because of how subtly yet powerfully it reframes what parents should value in their children: not grades or basketball trophies or college-acceptance letters or any of the things parents usually brag about. By doing so, it opens the door to a world less obsessed with achievement. Meredith pointed out that Down syndrome is defined and diagnosed by a medical system made up of people who have to be highly successful to get there, who likely base part of their identity on their intelligence. This is the system giving parents the tools to decide what kind of children to have. Might it be biased on the question of whose lives have value? ••• When Mary Wasserman gave birth to her son, Michael, in 1961, kids with Down syndrome in America were still routinely sent to state institutions. She remembers the doctor announcing, “It’s a mongoloid idiot”—the term used before chromosome counting became common—and telling her “it” should go to the state institution right away. Wasserman had volunteered for a week at such an institution in high school, and she would never forget the sights, the sounds, the smells. The children were soiled, uncared for, unnurtured. In defiance of her doctor, she took Michael home. The early years were not easy for Wasserman, who was a divorced mother for much of Michael’s childhood. She worked to support them both. There weren’t really any formal day cares then, and the women who ran informal ones out of their homes didn’t want Michael. “The other mothers were not comfortable,” one of them told her after his first week. Others rejected him outright. She hired private babysitters, but Michael didn’t have playmates. It wasn’t until he was 8, when a school for kids with disabilities opened nearby, that Michael went to school for the first time. Michael is 59 now. The life of a child born with Down syndrome today is very different. State institutions closed down after exposés of the unsanitary and cruel conditions that Wasserman had glimpsed as a high-school student. After children with disabilities go home from the hospital today, they have access to a bevy of speech, physical, and occupational therapies from the government—usually at no cost to families. Public schools are required to provide equal access to education for kids with disabilities. In 1990, the Americans With Disabilities Act prohibited discrimination in employment, public transportation, day cares, and other businesses. Inclusion has made people with disabilities a visible and normal part of society; instead of being hidden away in institutions, they live among everyone else. Thanks to the activism of parents like Wasserman, all of these changes have taken place in her son’s lifetime. Does she wish Michael had had the opportunities that kids have now? “Well,” she says, “I think maybe in some ways it was easier for us.” Of course the therapies would have helped Michael. But there’s more pressure on kids and parents today. She wasn’t shuttling Michael to appointments or fighting with the school to get him included in general classes or helping him apply to the college programs that have now proliferated for students with intellectual disabilities. “It was less stressful for us than it is today,” she says. Raising a child with a disability has become a lot more intensive—not unlike raising any child. I can’t count how many times, in the course of reporting this story, people remarked to me, “You know, people with Down syndrome work and go to college now!” This is an important corrective to the low expectations that persist and a poignant reminder of how a transforming society has transformed the lives of people with Down syndrome. But it also does not capture the full range of experiences, especially for people whose disabilities are more serious and those whose families do not have money and connections. Jobs and college are achievements worth celebrating—like any kid’s milestones—but I’ve wondered why we so often need to point to achievements for evidence that the lives of people with Down syndrome are meaningful. When I had asked Grete Fält-Hansen what it was like to open up her life to parents trying to decide what to do after a prenatal diagnosis of Down syndrome, I suppose I was asking her what it was like to open up her life to the judgment of those parents—and also of me, a journalist, who was here asking the same questions. As she told me, she had worried at first that people might not like her son. But she understands now how different each family’s circumstances can be and how difficult the choice can be. “I feel sad about thinking about pregnant women and the fathers, that they are met with this choice. It’s almost impossible,” she said. “Therefore, I don’t judge them.” Karl Emil had grown bored while we talked in English. He tugged on Grete’s hair and smiled sheepishly to remind us that he was still there, that the stakes of our conversation were very real and very human. This article appears in the December 2020 print edition. It was first published online on November 18, 2020. from https://ift.tt/2IMOpVt Check out http://natthash.tumblr.com Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. The reports have come in from all across the country: Hospitals are filling up, especially in the Midwest, and they are running out of the staff they need to take care of patients. Last week, the United States broke its record from April for the number of hospitalized COVID-19 patients, blowing past 60,000 all the way to 73,000, according to data compiled by the COVID Tracking Project at The Atlantic. Now new data released by the Department of Health and Human Services quantify the crisis in America’s hospitals in closer detail. At The Atlantic’s request, HHS provided data on the number of hospitals experiencing staffing shortages. From November 4 to November 11, 958 hospitals—19 percent of American hospitals—faced a staffing shortage. This week, 1,109 hospitals reported that they expect to face a staffing shortage. That’s 22 percent of all American hospitals. In eight states, the situation is even more dire. More than 35 percent of hospitals in Arkansas, Missouri, North Dakota, New Mexico, Oklahoma, South Carolina, Virginia, and Wisconsin are anticipating a staffing shortage this week. COVID-19 puts pressure on hospitals in two ways. One, staff members get sick or are exposed to the coronavirus and have to stay home, reducing the labor supply. Two, more patients arrive at the hospital, increasing demand. A surge of cases makes both factors worse. [Read: ‘No one is listening to us’] As a rule of thumb, the COVID Tracking Project has found that an increase in cases shows up as an increase in hospitalizations about 12 days later. Over the past 12 days, the seven-day average for new cases has jumped from fewer than 90,000 a day to 150,000 a day. While we’ve been able to track the number of people hospitalized with COVID-19 since March, we have not known how many new people were being admitted to hospitals each day, perhaps the best indicator of surging infections. But yesterday, HHS released this data going back to mid-July. At the peak of the summer surge, the seven-day average of daily admissions topped 5,000. Yesterday, the same measure topped 10,000. We should expect many more hospitalizations, and even worse staffing shortages, to come. 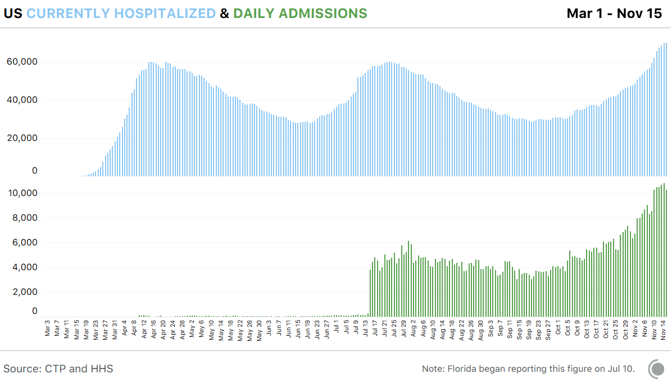
Even if a state has open hospital beds, it may not have the workers to put patients in them. “We are short of staff all times, either because they have COVID or they have some other illness, and we need to rule out COVID before we bring them back to work,” University of Wisconsin Health CEO Alan Kaplan told CNBC last week. The desperate times have led to some desperate measures. Last week, North Dakota Governor Doug Burgum ordered that health-care workers who have COVID-19 but are asymptomatic can be sent back to work. Many nurses have objected to the practice. Even without government mandates, the shortage of workers has meant that only 36 percent of hospital nurses are “always … able to stay home when they have influenza or COVID-like symptoms,” according to a survey by National Nurses United conducted from mid-October to November 9. [Read: The worst day of the pandemic since May] And that was before the current surge reached its recent heights. While we don’t have data for the spring, this week’s staffing shortages have already exceeded those of the summer, according to HHS. Nearly every state in every region is showing major increases in hospital admissions. But the Midwest is up roughly seven times from its September low. That’s a lot of pressure to exert on a region’s health-care systems, especially the staff. Beds can be built, floors can be repurposed, but you can’t simply train a new legion of nurses and doctors. During past surges, which were more localized, workers could be brought in from other places, but given that the current onslaught is national, that’s going to be much more difficult. 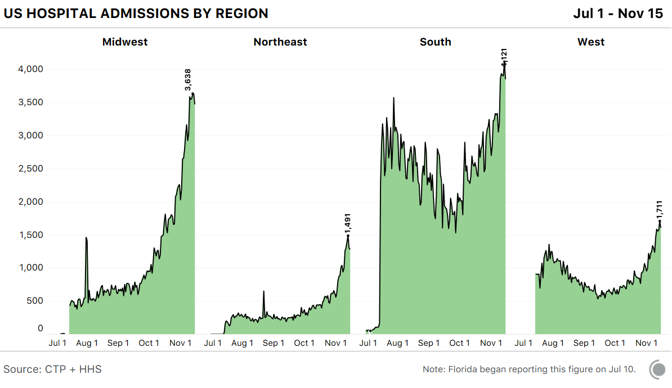
The core issue is the same one that doctors laid out in the spring: If infections are not brought under control, too many people will end up in beleaguered hospitals, and the standard of care will fall. We largely prevented that over the summer. And measured from the spring into the summer, death rates fell. While it is not clear that this drop continued into the fall, what does seem likely is that if a region’s health-care system begins to collapse under a staffing shortage, the case-fatality rate will rise again. That is to say, unless hospitalization trends change, more people will die, and die within sight of a vaccine. “If we can get patients into staffed beds, I feel like they’re doing better,” Eli Perencevich, an infectious-disease doctor at the University of Iowa, told my colleague Ed Yong. “But that requires a functional health-care system, and we’re at the point where we aren’t going to have that.” from https://ift.tt/38SO3Y2 Check out http://natthash.tumblr.com Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. There’s never a good time to get sick with COVID-19, but in the next few weeks it will be especially dangerous. America’s coronavirus epidemic is really, really bad right now. One-hundred-seventy-thousand-new-cases-a-day bad. Hospital-systems-on-the-brink-of-collapse bad. I asked Atlantic writers who have spent months reporting on the pandemic for their simplest advice on making it to the new year. Some Americans live with roommates, some can’t work without child care, and some have to work in crowded conditions—everyone’s situation is different—but these basic tips can, we hope, be helpful in a variety of situations. My colleagues’ guidance boils down to this winter’s golden rule for interacting with anyone outside your immediate household: Don’t spend time indoors with other people. The perils of the indoors have been demonstrated scientifically; for example, one study earlier this year found that a sick person was 18.7 times more likely to spread the coronavirus in a “closed environment” (such as a gym, a floating restaurant boat, or a poorly ventilated tent) than in an “open-air environment.” Some indoor spaces are likely riskier than others. Earlier this year, my colleague Derek Thompson advised readers to avoid especially spitty environments like bars, indoor restaurants, and gyms, where people are more likely to be eating, talking, shouting, singing, or breathing heavily than they are at, say, the grocery store. Restaurant dining in particular has been linked to a heightened risk of coronavirus transmission. [Read: It’s time to hunker down] But talking, eating, and other merrymaking doesn’t magically become safe when it happens inside your home. The coronavirus spreads through the air, so—no matter where you are, even if you’re at your grandma’s house, or your best friend’s—breathing the same air as other people for extended periods of time is risky. Your best bet is to avoid indoor gatherings altogether. They can be made marginally safer through testing, masking, and limiting the number of attendees, but none of these methods is foolproof. As my colleague Sarah Zhang has written, a negative COVID-19 test is not a “get out of jail free” card; it’s unclear how well the tests work on people who aren’t feeling sick. Masks don’t do much good if people spend several hours together in an unventilated room. And several public-health experts recently told The Washington Post that even small, casual get-togethers are significantly contributing to the spread of the virus. [Read: The pandemic is in uncharted territory] All of these precautions are flawed; like slices of Swiss cheese, they have holes that let the virus through. But if you layer your Swiss cheese, gathering only in small numbers while wearing masks after being tested, the chance of transmission does meaningfully drop. The most effective ways to mitigate risk indoors (and again, if you can avoid it, it’s best not to be indoors) might include some approaches that have gotten less attention in the past few months. For example, if you’re inside with other people, limit the time you spend there. A 15-minute visit with a handful of friends is less dangerous than a four-hour dinner party with them. My colleague Olga Khazan also emphasized that you should consider local transmission rates before deciding whether to see anyone else indoors. As she reported last month, it’s safer (but still not entirely safe) to gather inside if your area is seeing 10 or fewer new cases a day per 100,000 people. Right now that excludes most major metropolitan areas in the United States, as well as plenty of rural counties. But keep in mind that local regulations don’t necessarily map onto local risk. As Amanda Mull has written, just because a business is legally open doesn’t mean you can patronize it safely. Amanda and Annie Lowrey have both written about how state and local governments are allowing businesses to stay open beyond the boundaries of safety because they fear the economic outcomes of closing them. [Read: The simple rule that could keep COVID-19 deaths down] If you must gather inside, it’s best to make the indoors as outdoorsy as possible. As Zeynep Tufekci wrote in The Atlantic this summer, managing airflow is crucial for curtailing airborne transmission, and it hasn’t received nearly enough attention. Powerful air filtration is the best standard, but even failing that, you can use fans, windows, and your HVAC system to trade as much air as possible between your home and the outside world; here’s a helpful guide for the amateur airflow artiste. If it’s any comfort, you can ignore certain dubious safety measures. That includes the conspicuous but largely useless sanitization regimes that Derek has dubbed hygiene theater, as well as fever checks, which my colleague James Hamblin has warned might do more harm than good. Focusing on what individuals can do to slightly reduce the risk that was created by monstrous systemic failure might seem futile, or entirely beside the point. But in the absence of massive federal mobilization, which seems unlikely to arrive under the Trump administration, it might be the best we can do. [Read: The worst day of the pandemic since May] That’s why I want to leave you with an invitation (not to my house!) that, I hope, does not seem too naive: Adjust the way you’re thinking about the pandemic. Remember that your decisions affect everyone you share air with, no matter how circumstantially, as you go about your life. Even if you accept the risk of a dinner party, you likely haven’t consulted with the person who’ll be bagging your groceries a week later. And finally, try to think on a longer timescale. Learn to read the trends in case and hospitalization numbers so you can peek at the future. Make a plan for isolating from the outside world and the rest of your household in case you do get sick. Things are going to get worse before they get better, but for perhaps the first time since the pandemic started, it is clear that they are going to get better. Two vaccine candidates seem more promising than public-health experts had hoped. The president-elect has pledged to ground his approach to the pandemic in science. The canceled holidays and the third straight night of freezer pizza aren’t going to last forever. Remembering that could make these next few months of restraint a little easier to bear. from https://ift.tt/3pB216G Check out http://natthash.tumblr.com The United States is now in what disaster-preparedness experts once modeled as a worst-case scenario. We are flooded with a highly transmissible virus that causes unpredictable symptoms: sometimes mild, sometimes fatal. The curve is not flat, or even a curve. It’s almost a line that points straight upward. More than 1,000 Americans are dying every day, on average. Soon that number will likely hit 2,000. In this precarious moment, many Americans are planning to celebrate the Thanksgiving holiday by traveling and having dinner with 10 or more people. Pandemic models generally account for such behavior in the early stages of an outbreak, before people understand the nature of a virus, but not during the heart of the crisis. If this were an outbreak movie, and the characters were congregating in multigenerational units indoors to have boisterous conversations over lengthy meals, you’d probably be yelling at your screen. Few things sound nicer than sitting around eating with friends and family, after so much isolation and worry over this decades-long year. But from an infectious-disease standpoint, the guidelines in this moment are unfortunately straightforward: Limit activities to those essential to life. Don’t gather socially. Don’t travel. Many doctors and public-health experts have spoken out to this effect in recent weeks. Don’t celebrate Thanksgiving in anything resembling the modern American way—with multigenerational gatherings that involve travel and prolonged conversations over an indoor meal. In short, do not do anything resembling a Norman Rockwell painting. If you or your loved ones haven’t heard this directive, there’s a reason. In another administration, the Centers for Disease Control and Prevention would issue guidelines to Americans, in a coordinated effort with the president and coronavirus task force to be concrete in advising and coordinating with governors, mayors, and citizens. Instead, there is a messaging void. The president has abdicated his duties since the lead-up to the election. He has broken with his task force and refused to concede or allow transfer of power to incoming experts, leaving them without vital information. The CDC has a middling page of new “considerations” for holiday celebrations that the agency’s officials have neither publicly announced nor explained in news conferences. [Read: How Trump sold failure to 70 million people] Many local health departments, mayors, and governors have stepped up. In Baltimore and Chicago public-health directives have clearly advised people not to gather for the holiday. But our landscape is also dotted with local leaders who are unable or afraid to go nearly so far. Telling people not to gather for a holiday is, of course, an unpopular message. So I’m doing it. The truth is that we’ll likely need to be more careful with each passing day this winter, not less. The virus knows no difference between holidays and workdays. Our default should be to treat Thanksgiving as a day when the health guidelines are no different from any other day. As the prevalence of the virus increases, things that were previously low risk become more dangerous. Hence the return of directives: Don’t gather indoors. Don’t travel. It’s never been advisable during the pandemic to socialize with people outside your bubble who can’t manage to wear masks and keep their distance, but it’s especially injudicious now. No family member should put pressure on others to gather. It’s likely that many people will join reluctantly because they don’t want to be the ones who are no fun, or to keep others in the family from acting indignant or insulted. Let those people be indignant. That’s on them. Remember that this isn’t a personal or even a family-wide calculation. The risk of such gatherings is not limited to those who gather. Each transmission of the virus is like lighting a tree on fire in a forest. A small wedding in Maine in August, for example, is known to have led to the deaths of seven people who were not in attendance. We are all in this together. That means everyone has to do their part. Just because a local official has not banned or warned against gathering with elders indoors does not make it safe. Some states, counties, and cities will warrant stricter restrictions than others. In disaster zones, like El Paso, Texas, where hospital ICUs are full and inmates are being drafted to staff makeshift morgues, it may be necessary to advise people not to leave home at all. (Officials in El Paso restricted business activity in late October, but a Texas court of appeals overturned the city’s stay-at-home order on Friday.) Hopefully few places get to that point. In warm areas with less spread, people could have outdoor gatherings of small groups, if everyone is vigilant about not getting too close. But that should be the extent of what celebrations happen anywhere. [Read: It’s time to hunker down.] Ideally by now many people have social bubbles so they’re not entirely alone. Expanding this bubble for a single day is logistically difficult. Theoretically everyone in a family could isolate for two weeks prior and get tested multiple times over that period, and the risk of a gathering would be low. There may be certain circumstances where families try this, for example because a loved one is terminally ill, and this occasion carries particular significance. But the gathering can never be zero risk. Quarantining for two weeks after would be key, as well. In all, this would mean a month of meticulous isolation in order to have a probably-safe indoor meal. That’s a lot to ask. Many people are unlikely to be willing and able to go to those lengths. This doesn’t mean the day needs to be joyless. It’s just that we need to be creative this year about how to find that joy. Celebrating Thanksgiving by entering someone’s home and spreading a lethal infectious disease is a little too darkly ironic anyway. Take the opportunity to think about what you love most about the day. Focus on how to re-create that, and even build on it. Maybe learn to cook one of the dishes that someone else usually brings to dinner. Think of the people you actually look forward to seeing, and call them. Think of the people you don’t look forward to seeing, and don’t call them. Appreciate that you can’t get cornered by some annoying second cousin; you save money on travel; you don’t have to pretend to care about football. Maybe most important, this year is an opportunity to bond over the moral certainty of the moment. At its core, Thanksgiving is a nebulous day of atoning for the sins of colonialism by eating food and saying thank you. Now families and friends and communities can work together to achieve something meaningful and good: ending the pandemic. All you’re asked to do is eat food at home. Whatever you do, take heart that this radically different pandemic lifestyle doesn’t have to last too much longer. By next Thanksgiving, if the news of an effective vaccine proves as fortuitous as it sounds, we can go back to whatever traditions draw people to this day. This is a onetime deal. Next year will be an opportunity to be thankful for the elements of the holiday that we tend to take for granted. It will be like a Super Thanksgiving. Or maybe this new way of doing it will work so well, you’ll never want to go back. from https://ift.tt/2Kfd4m1 Check out http://natthash.tumblr.com The end may be near for the pestilence that has haunted the world this year. Good news is arriving on almost every front: treatments, vaccines, and our understanding of this coronavirus. Pfizer and BioNTech have announced a stunning success rate in their early Phase III vaccine trials—if it holds up, it will be a gamechanger. Treatments have gotten better, too. A monoclonal antibody drug—similar to what President Donald Trump and former Governor Chris Christie received—just earned emergency-use authorization from the FDA. Dexamethasone—a cheap, generic corticosteroid—cut the death rate by a third for severe COVID-19 cases in a clinical trial. Doctors and nurses have much more expertise in managing cases even in using nonmedical interventions like proning, which can improve patients’ breathing capacity simply by positioning them facedown. Health-care workers are also practicing fortified infection-control protocols, including universal masking in medical settings Our testing capacity has greatly expanded, and people are getting their results much more quickly. We may soon get cheaper, saliva-based rapid tests that people can administer on their own, itself a potential game-changer. [Read: The vaccine news that really matters] The Centers for Disease Control and Prevention has finally acknowledged that aerosol transmission happens and that ventilation is important. The initial bungled messaging and science around masks was unfortunate, but things have turned around; the CDC has even publicized how masks can help protect the wearer from infection, as well as lower the chances of onward transmission. The importance of clusters and super-spreading is more widely appreciated, maybe partly because of the highly publicized White House cluster, which is still simmering. We have reasons to celebrate, but—and you knew there was a but—a devastating surge is now under way. And worse, we are entering this dreadful period without the kind of leadership or preparation we need, and with baseline numbers that will make it difficult to avoid a dramatic rise in hospitalizations, deaths, and potential long-term effects on survivors. Almost every day, America is breaking new records in confirmed cases: They are up 40 percent from just one week ago. These cases are not confined to a region or a state; the whole nation is in the midst of a terrible surge. So too is much of Europe, where country after country is experiencing record numbers of cases. This is not a “casedemic”—the false notion that we just have better testing and detection, without any real change in the underlying risk for illness and death. It’s true that we missed a lot of cases in the spring because we didn’t have enough tests, and that we are catching more of them now. But it’s not just confirmed cases that are on the rise. The United States is also experiencing a steep increase in hospitalizations, as well as about 1,500 reported deaths a day; those are the highest numbers since mid-May, and they are still rising sharply. Trevor Bedford, a scientist at Fred Hutchinson Cancer Research Center, in Seattle, calculates that more than 2,000 deaths a day may already be baked in for early December, meaning that even if we stopped every new infection from now on, we’d still see that many people die per day in just a few weeks among those already infected. [Read: ‘No one is listening to us’] The Pfizer-BioNTech vaccine—or Moderna’s vaccine—may be available in the United States to health-care workers and other high-priority people as early as the end of this year. But it won’t be distributed widely until well into 2021, even in the best-case scenario—and the Pfizer vaccine needs two doses, about 21 days apart. Those promising monoclonal antibodies, too, are in very short supply. The president was one of fewer than 10 people to receive the treatment outside of a clinical trial. Even if the drug works as well as we hope, the 300,000 doses that Eli Lilly has agreed to deliver will not be enough when they finally arrive, probably toward the end of this year when we have a hundred fifty thousand positive cases per day, and still rising. Dexamethasone availability is excellent, but deaths are climbing despite its widespread use, because it helps address only one of this disease’s complications. We have little reason to count on the authorities for leadership that has the precision and scale we need. The outgoing president has refused to concede the election and has launched a flurry of frivolous lawsuits to muddy the transition, thereby making the odds of an effective federal response over the next few months less likely. All of this means we desperately need to flatten the curve again before hospitals nationwide are overrun. Utah, Illinois, Minnesota, Colorado, and other states are already reporting that hospitals and intensive-care units are at or near capacity. The bottleneck for medical care isn’t just lack of space, or even equipment, which we may be able to increase, but staff—trained nurses and doctors who can attend to patients, and who cannot be manufactured out of thin air. During the spring crisis in the New York tri-state area, health-care workers from around the country rushed to the region, buttressing the exhausted medical workforce. With a nationwide surge, doctors and nurses are needed in their hometown hospitals. If fewer people can be admitted to hospitals because of lack of space, patients won’t benefit from our improved clinical management of COVID-19. We may give back some of our gains in the mortality rate. We may also see deaths rise from other causes: Fewer nonurgent but important surgeries, more overworked medical staff, and overburdened emergency rooms could all contribute to worsening health outcomes for many other viruses that peak in winter months, like influenza, as well other ordinary medical conditions. This seasonality is not a huge surprise, which makes our lack of preparation even more tragic. The 1918 flu pandemic saw an earlier, milder wave in the spring; a lull in the summer; and a deadlier surge starting in the fall. Other coronaviruses endemic to us are also sharply seasonal, tending to peak in winter. This may be because the humidity and temperature conditions of fall and winter favor the virus more. It may also be because we spend more time indoors during the winter. Most likely, it’s a combination, along with other factors (Less vitamin D? less light?). Whatever the causes, public-health experts knew a fall and winter wave was a high likelihood, and urged us to get ready. But we did not. The best way to prepare would have been to enter this phase with as few cases as possible. In exponential processes like epidemics, the baseline matters a great deal. Once the numbers are this large, it’s very easy for them to get much larger, very quickly—and they will. When we start with half a million confirmed cases a week, as we had in mid-October, it’s like a runaway train. Only a few weeks later, we are already at about 1 million cases a week, with no sign of slowing down. Americans are reporting higher numbers of contacts compared with the spring, probably because of quarantine fatigue and confusing guidance. It’s hard to keep up a restricted life. But what we’re facing now isn’t forever. It’s time to buckle up and lock ourselves down again, and to do so with fresh vigilance. Remember: We are barely nine or 10 months into this pandemic, and we have not experienced a full-blown fall or winter season. Everything that we may have done somewhat cautiously—and gotten away with—in summer may carry a higher risk now, because the conditions are different and the case baseline is much higher. When community transmission is this high, every kind of exposure is more dangerous. A gym class is more likely to have someone who is infectious. Workplaces will have more cases, meaning more employees will unknowingly bring the virus home. More people at the grocery store will be positive. A casual gathering of friends may be harder to hold outdoors. Even transmission from surfaces may pose a higher risk now, because lower humidity levels may improve the survivability of the virus. Plus, the holidays are upon us, which means a spike in gatherings of people who do not otherwise see one another. Such get-togethers, especially if they are multigenerational, can spark more outbreaks. I take no joy in saying this, but all of this means that any gathering outside one’s existing quarantine pod should be avoided for now—especially if it is indoors. Think of it as a postponement and plan to hold it later. Better a late Christmas than an early medical catastrophe. Pods should not expand unless absolutely necessary. Order takeout instead of dining indoors. Make game night virtual. Shop in bulk, so you can do fewer trips to the store. It’s not the right time for wedding receptions or birthday parties. Young people present one of the biggest challenges. Many colleges are ending school and sending students home, for what could be a country-wide super-spreader event. That age group—young adults—is especially dangerous; while they can get infected, they are less likely to get very sick, so they don’t stay put the way sick people would. That means they pose a great risk to their more vulnerable parents and other older relatives as they go about their lives. Ideally, colleges should offer the students already on campus the option to stay in the dorms over winter break, and those who live in off-campus housing should consider staying put. If they do go home, the students should quarantine for the recommended two weeks to the greatest degree possible. It might also be time for ordinary people to consider using higher-quality masks (N95s and KN95s)—something that public-health experts have long recommended. This is especially true for low-wage workers, a disproportionate number of whom are people of color and have to work indoors; older people, and anyone who works with them; and people with preexisting conditions that put them at higher risk. Ideally, we’d have a significant aid package, allowing businesses to remain closed and workers to stay home as much as possible, while also increasing workplace standards through better ventilation and masks. Tragically, that doesn’t seem to be in the cards. On the plus side, though, it’s now possible for ordinary people to purchase higher-quality masks, which suggests that the dire shortage of Spring is over. It’s still wise to avoid hoarding; most people don’t need that many, and this surge will put a fresh strain on the supplies. As long as they are put on and taken off carefully (use hand sanitizer before and after), such masks are reusable after being left in a paper bag or breathable container for at least five days, which means as few as five are enough to rotate through a typical work week for people who work with others—especially indoors. All of this is unpleasant, but the alternative is much worse. There is a Turkish saying for times like these, when we can see a light at the end of the tunnel: “Time passes quickly if we can count the days until the end.” We are no longer in the open-ended, dreadful period of spring 2020, when we did not know if we’d even have a vaccine, whether any therapeutics would work, and whether we’d ever emerge from the shadow of this pandemic. We can see the cavalry coming, but until it’s here, we need to lock ourselves down once again. from https://ift.tt/38GRLUD Check out http://natthash.tumblr.com |
Authorhttp://natthash.tumblr.com Archives
April 2023
Categories |
 RSS Feed
RSS Feed
