|
All skinfolk ain’t kinfolk, but as Black people in America, we still feel a connection with one another. A reciprocated smile as we pass one another on the street; a spontaneous, but still synchronized, “Swag Surfin’” dip at the club; a “Cupid Shuffle” kick at the cookout. Small moments like these reinforce the bond I feel with other Black people. But these days, as I quarantine at home, the Black faces sparking that sense of familiarity are not nodding in solidarity or swaying in unison. They stare back, frozen in photographs accompanying obituaries that announce yet another Black life lost to the coronavirus. I do not know these people. I am not even one of the 31 percent of Black people in America who personally knows someone who has died of COVID-19. But in these faces I see my loved ones. I see myself. I thought of these obituaries last week, when the United States passed yet another grim pandemic milestone. More than 50,000 Black Americans are now dead from COVID-19, according to data from the COVID Racial Data Tracker, a collaboration between The COVID Tracking Project at The Atlantic and the Boston University Center for Antiracist Research. (And even that number is likely an undercount: We don’t know the race or ethnicity for roughly 20,000 of the 319,000 Americans whose lives have been claimed by COVID-19.) Everyone in the U.S. is at the mercy of the coronavirus; it doesn’t discriminate by race or class or gender or age. And yet, from the very beginning of the pandemic, the virus has exposed and targeted all of the disparities that come along with being Black in America. We are dying at 1.7 times the rate of white people from this virus, which means that the toll of these disparities has never been easier to quantify: 19,000 Black people would still be alive if not for systemic racism. [Ibram X Kendi: Stop blaming Black people for dying of the coronavirus] For centuries, Black people have spoken about the struggles we face, pointing to root causes like poverty, housing segregation, unemployment, and environmental degradation. And for centuries, those concerns have largely gone ignored. The same thing has happened with the pandemic. Long before any data confirmed our worst fears, Black people knew that the coronavirus would disproportionately devastate our already vulnerable communities. Driven by that foresight, I launched a newsletter, Coronavirus News for Black Folks, in early April. As the death toll crept up and up, the brutality of American racism became even clearer. Black people with clear symptoms of COVID-19 were turned away from receiving tests, sometimes on multiple occasions, only to die at home. Black families were entirely destroyed as members died within weeks and days of one another. By the end of July, twice as many Black children as white children had died of COVID-19: In Michigan, the first child to die from the virus was a 5-year-old Black girl who spent two weeks on a ventilator. While a large swath of Americans, myself included, are able to safely stay at home, Black people are disproportionately essential workers, who have no choice but to brave the pandemic and head to work. Many have lost their lives working jobs they felt were unsafe and underpaid. “Our white executive director has not been in the office for the past six weeks, has not asked how any of us are holding up, and has not emailed us to say thank you,” a 20-something security guard told me in April. “I feel betrayed. I used to love my position and the people I work with. Now I’m resentful of the protection some people are afforded while others, like myself, are sent out to the front lines.” (The security guard was granted anonymity for fear of professional reprisal.) As if the havoc wreaked by the virus wasn’t already bad enough, the racial disparities will persist as the U.S. works its way out of the pandemic. Just as one in three Black people knows someone directly who has died from COVID-19, one in three Black people has said they will not get the vaccine, according to a recent Kaiser Family Foundation study. Clinical trials have shown that the vaccine is safe and effective, but a long-standing mistrust in America’s predominantly white medical institutions is only deepening, and so the number of Black lives lost to this virus will continue to rise, even though we now have a way to end it. Thankfully, moments of Black kinship still emerge even during all the suffering. The same week that marked more than 50,000 Black deaths saw a horizon of hope. Sandra Lindsay, a Jamaican-born nurse in Queens, New York, became the first person to be vaccinated in the United States, after receiving the shot from Michelle Chester, also a Black woman. Even a pandemic can’t break the resilient bond of Black America. from https://ift.tt/37IAhGC Check out http://natthash.tumblr.com
0 Comments
Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. California is on the verge of breaking a pandemic record from the darkest days of the spring: With 17,750 COVID-19 patients hospitalized yesterday, the state is closing in on New York’s single-day high of 18,825, set on April 13. It’s a shocking turn of events for California, a huge state that, not long ago, had better control of—or luck with—the virus than much of the country. In October, as the pandemic’s winter surge was beginning to take shape across the U.S., California’s public-health researchers and officials expressed measured optimism that the nation’s most populous state could avoid a disastrous rise in cases. During a press conference on October 19, Governor Gavin Newsom pointed to declining hospitalization rates as a sign of the state’s success, but also warned that the decline was slowing. “We’re beginning to flatten out, plateau, as relates to hospitalizations,” he said. For a moment, such a plateau seemed like the most likely outcome. A week after Newsom’s press conference, the state had 2,991 people hospitalized with COVID-19, its lowest number since April 10. But the trend quickly reversed, and by November 23, the state’s hospitalizations had doubled to more than 6,000. [Read: The pandemic’s final surge will be brutal] What’s happened since is a worst-case scenario. While California’s per capita hospitalization rate is nowhere near New York at its worst—with 39.5 million people, the Golden State is about twice as populous as New York—the sheer number of patients in the hospital is still a sign of how badly California is doing right now. Worse yet is how quickly the state reached nearly 18,000 hospitalizations during its current surge. When New York reached its record, it represented a 12 percent increase over the week prior. In California, by contrast, hospitalizations are up 27 percent over last week. With cases in California continuing to rise, more hospitalizations will follow. Things are much worse in some parts of the state than others. Southern and central California are driving the current surge: 34 percent of the state’s hospitalized patients are in Los Angeles County, the nation’s most populous by far. Yesterday, 620 people per million were hospitalized with confirmed COVID-19 there, the fifth-highest rate among California counties. Plus, Los Angeles County contains only a portion of the sprawling metro area. San Bernardino County, Los Angeles County’s neighbor to the east, has an even higher rate of hospitalizations, with 766 per million. Orange County, just south of Los Angeles County, with 561 per million, and Riverside County, east of Orange County, with 540 per million, are also among the 10 California counties with the highest COVID-19 hospitalization rates. Together, these four counties account for more than 11,000 of the state’s 17,750 hospitalized patients. Just one other California county with more than 500,000 residents has a higher rate than Los Angeles County—Stanislaus, a food-production center in the Central Valley east of San Francisco with a large population of essential workers, many of whom live in cramped conditions and are unable to stop working during an economic downturn. The Bay Area is doing better than Southern California, but this surge is still the region’s worst to date. Santa Clara, the Bay Area’s largest county, has the highest rate, with a concerning 323 people hospitalized per million—like Los Angeles County, that’s about three times higher than Santa Clara’s previous high this summer. San Francisco County, home to fewer than 900,000 people, has just 175 hospitalized right now, with a rate one-third that of Los Angeles County. A more expansive definition of the Bay Area might include San Joaquin County, which borders Stanislaus and has a hospitalization rate of 445 per million; the Central Valley region, including Fresno and the San Joaquin Valley, has been approaching its limited intensive-care-unit capacity in recent weeks. Northern California, as defined by the state for its regional stay-at-home orders, is still better off: 28.7 percent of its ICU beds are available, so it’s not under the state stay-at-home orders that are triggered when ICU capacity falls below 15 percent in a particular area. For comparison, the Bay Area is at 13.7 percent. Greater Sacramento is at 16.2 percent. Meanwhile, the San Joaquin Valley and Southern California are essentially full. California has very little room for error; on December 3, The New York Times reported that only two states had fewer ICU beds in total per capita. By comparison, Poland has nearly the same population and three times as many hospital beds. [Read: The U.S. has passed the hospital breaking point] Why California—a state that had been an example of a reasonably effective response—and why now? Some officials have pointed to lockdown fatigue. Thanksgiving alone is not the culprit, as cases were clearly rising in early November. The state’s reversal of fortunes is so sharp and sudden that the reasons remain unclear, but its time as a big and relatively bright spot in a dark winter has definitively come to an end. from https://ift.tt/2KjMGYG Check out http://natthash.tumblr.com The newly discovered coronavirus had killed only a few dozen people when Feixiong Cheng started looking for a treatment. He knew time was of the essence: Cheng, a data analyst at Cleveland Clinic, had seen similar coronaviruses tear through China and Saudi Arabia before, sickening thousands and shaking the global economy. So, in January, his lab used artificial intelligence to search for hidden clues in the structure of the virus to predict how it invaded human cells, and what might stop it. One observation stood out: The virus could potentially be blocked by melatonin. Melatonin, best known as the sleep hormone, wasn’t an obvious factor in halting a pandemic. Its most familiar role is in the regulation of our circadian rhythms. Each night, as darkness falls, it shoots out of our brain’s pineal glands and into our blood, inducing sleep. Cheng took the finding as a curiosity. “It was very preliminary,” he told me recently—a small study in the early days before COVID-19 even had a name, when anything that might help was deemed worth sharing. After he published his research, though, Cheng heard from scientists around the world who thought there might be something to it. They noted that, in addition to melatonin’s well-known effects on sleep, it plays a part in calibrating the immune system. Essentially, it acts as a moderator to help keep our self-protective responses from going haywire—which happens to be the basic problem that can quickly turn a mild case of COVID-19 into a life-threatening scenario. Cheng decided to dig deeper. For months, he and colleagues pieced together the data from thousands of patients who were seen at his medical center. In results published last month, melatonin continued to stand out. People taking it had significantly lower odds of developing COVID-19, much less dying of it. Other researchers noticed similar patterns. In October, a study at Columbia University found that intubated patients had better rates of survival if they received melatonin. When President Donald Trump was flown to Walter Reed National Military Medical Center for COVID-19 treatment, his doctors prescribed—in addition to a plethora of other experimental therapies—melatonin. Eight clinical trials are currently ongoing, around the world, to see if these melatonin correlations bear out. Few other treatments are receiving so much research attention. If melatonin actually proves to help people, it would be the cheapest and most readily accessible medicine to counter COVID-19. Unlike experimental drugs such as remdesivir and antibody cocktails, melatonin is widely available in the United States as an over-the-counter dietary supplement. People could start taking it immediately. Yet Cheng emphasizes that he’s not recommending that. Like any substance capable of slowing the central nervous system, melatonin is not a trifling addition to the body’s chemistry. Its apparent benefit to COVID-19 patients could simply be a spurious correlation—or, perhaps, a signal alerting us to something else that is actually improving people’s outcomes. Cheng thinks that might be the case. He and others suggest that the real issue at play may not be melatonin at all, but the function it most famously controls: sleep. In fact, several mysteries of how COVID-19 works converge on the question of how the disease affects our sleep, and how our sleep affects the disease. The virus is capable of altering the delicate processes within our nervous system, in many cases in unpredictable ways, sometimes creating long-term symptoms. Better appreciating the ties between immunity and the nervous system could be central to understanding COVID-19—and to preventing it. Throughout the pandemic, the department of neurology at Johns Hopkins University has been flooded with consultation requests for people suffering from insomnia. Rachel Salas, one of the team’s neurologists, says she initially thought this surge in sleep disorders was merely the result of all the anxieties that come with a devastating global crisis: worries about health, the economic impact, and isolation. Indeed, patterns of sleep disruption have played out around the world. Roughly three quarters of people in the United Kingdom have had a change in their sleep during the pandemic, according to the British Sleep Society, and less than half are getting refreshing sleep. “In the summer, we were calling it ‘COVID-somnia,’” Salas says. In recent months, however, Salas has watched a more curious pattern emerge. Many people’s sleep continues to be disrupted by predictable pandemic anxieties. But more perplexing symptoms have been arising specifically among people who have recovered from COVID-19. “We’re seeing referrals from doctors because the disease itself affects the nervous system,” she says. After recovering, people report changes in attention, debilitating headaches, brain fog, muscular weakness, and, perhaps most commonly, insomnia. Many don’t seem anxious or preoccupied with pandemic-related concerns—at least not to a degree that could itself explain their newfound inability to sleep. Rather it is sometimes part of what the medical community has begun to refer to as “long COVID,” where symptoms persist indefinitely after the virus has left a person. When it comes to sleep disturbances, Salas worries, “I expect this is just the beginning of long-term effects we’re going to see for years to come.” Her colleague Arun Venkatesan has been trying to get to the bottom of how a virus could cause insomnia. He focuses specifically on autoimmune and inflammatory diseases that affect the nervous system. Initially, Venkatesan says, the common assumption among doctors was that many post-COVID-19 symptoms were due to an autoimmune reaction—a misguided, targeted attack on cells of one’s own body. This can happen in the nervous system after infections by various viruses, in predictable patterns, such as that of Guillain-Barré syndrome. In the days after an infection, as new antibodies mistakenly attack nerves, weakness and numbness spread from the tips of the extremities inward. Disconcerting as it can be, this type of pattern is at least identifiable and predictable; doctors can tell patients what they’re dealing with and what to expect. By contrast, the post-COVID-19 patterns are sporadic, not clearly autoimmune in nature, says Venkatesan. The symptoms can appear even after a mild case of COVID-19, and timescales vary. “We’ve seen a number of patients who were not even hospitalized, and felt much better for weeks, before worsening,” Venkatesan says. And the findings aren’t limited to the brain. At Northwestern University, the radiologist Swati Deshmukh has been fielding a steady stream of cases in which people experience nerve damage throughout the body. She has been looking for evidence that the virus itself might be killing nerve cells. Hepatitis C and herpes viruses are known to do so, and autopsies have found SARS-CoV-2 inside of nerves in the brain. Still, she believes, symptoms are most likely due to inflammation. Indeed, the leading theory to explain how a virus can cause such a wide variety of neurologic symptoms over a variety of timescales comes down to haphazard inflammation—less a targeted attack than an indiscriminate brawl. This effect is seen in a condition known as myalgic encephalomyelitis, sometimes called chronic fatigue syndrome. The diagnosis encompasses myriad potential symptoms, and likely involves multiple types of cellular injury or miscommunication. In some cases, damage comes from prolonged, low-level oxygen deprivation (as after severe pneumonia). In others, the damage to nerve-cell communication could come by way of inflammatory processes that directly tweak the functioning of our neural grids. The unpredictability of this disease process—how, and how widely, it will play out in the longer term, and what to do about it—poses unique challenges in this already-uncertain pandemic. Myalgic encephalomyelitis is poorly understood, stigmatized, and widely misrepresented. Medical treatments and diagnostic approaches are unreliable. General inflammatory states rarely respond to a single prescription or procedure, but demand more holistic, ongoing interventions to bring the immune system back to equilibrium and keep it there. The medical system is not geared toward such approaches. But this understanding of what is happening may also offer some hope. Although the technical details are clearly thorny, there is some reassurance in what the doctors are not seeing. When nerves are invaded and killed, the damage can be permanent. When nerves are miscommunicating—in ways that come and go—that process can be treated, modulated, prevented, and quite possibly cured. Although sleep cycles can be disturbed and damaged by the post-infectious inflammatory process, radiologists and neurologists aren’t seeing evidence that this is irreversible. And among the arsenal of ways to attempt to reverse it are basic measures such as sleep itself. Adequate sleep also plays a part in minimizing the likelihood of ever entering into this whole, nasty, uncertain process. A central function of sleep is maintaining proper channels of cellular communication in the brain. Sleep is sometimes likened to a sort of anti-inflammatory cleansing process; it removes waste products that accumulate during a day of firing. Without sleep, those by-products accumulate and impair communication (just as seems to be happening in some people with post-COVID-19 encephalomyelitis). “In the early stages of COVID-19, you feel extremely tired,” says Michelle Miller, a sleep-medicine professor at the University of Warwick in the U.K. Essentially, your body is telling you it needs sleep. But as the infection goes on, Miller explains, people find that they often can’t sleep, and the problems with communication compound one another. The goal, then, is breaking out of this cycle, or preventing it altogether. Here the benefits of sleep extend throughout the body. “Sleep is important for effective immune function, and it also helps to regulate metabolism, including glucose and mechanisms controlling appetite and weight gain,” Miller says. All of these bear directly on COVID-19, as risk factors for severe cases include diabetes, obesity, and sleep apnea. Even in the short term, getting enough deep, slow-wave sleep will optimize your metabolism and make you maximally prepared should you fall ill. These effects may even bear on vaccination. Flu shots appear to be more effective among people who have slept well in preceeding days getting one. All of this leads back to the basic question: Is one of the most glaring omissions in public-health guidelines right now simply to tell people to get more sleep? The only health advice more banal than being told to wash your hands is being told to sleep more. But it’s a cliché for a reason. Sleep fortifies and prepares us for any given crisis, but especially when the days are short and cold, and people have little else they might do to empower and protect themselves. Monotonous days can slip people into depression, alcohol abuse, and all manner of suboptimal health. It may well turn out that standard pandemic advice should be to wear a mask, keep distances, and get sleep. That’s easier said than done. Asim Shah, a psychiatry and behavioral-sciences professor at Baylor College of Medicine, believes sleep is at the core of many of the mental-health issues that have spiked over the course of the year. “There’s a complete lack of structure. That has caused a huge disturbance in the sleep cycles,” he says. “Usually everyone has a schedule. They get sunlight and they generate melatonin and it puts them to sleep. Right now we’re seeing people losing interest in things, isolating, not exercising, and then not getting sleep.” Depression and anxiety make insomnia worse, and the cycle degenerates. This may be where melatonin—or other approaches to enhancing the potent effects of sleep—could be consequential. Russel Reiter, a cell-biology professor at the University of Texas at San Antonio, is convinced that widespread treatment of COVID-19 with melatonin should already be standard practice. In May, Reiter and colleagues published a plea for melatonin to be immediately given to everyone with COVID-19. If the world of melatonin research had a molten core, it would be Reiter. He has been studying the hormone’s potential health benefits since the 1960s, and tells me he takes 70 milligrams daily. (Most bottles at the pharmacy recommend from 1 to 10 milligrams.) After we spoke, he sent me some of the many journal articles he has published on melatonin and COVID-19, at least four of which appeared in Melatonin Research. He blithely referred to them as “propaganda” and noted that he has been studying melatonin since before I was born (without asking when that was). “I know melatonin sideways and backwards,” Reiter said, “and I’m very confident recommending it.” The majority of sleep scientists, though, seem to agree that the most crucial interventions that facilitate sleep will not be medicinal, or even supplemental. The general recommendation is that getting your body’s melatonin cycles to work regularly is preferable to simply taking a supplement and continuing to binge Netflix and stare at your phone in bed. Now that so many people’s days lack structure, Shah believes a key to healthy pandemic sleep is to deliberately build routines. On weekends, wake up and go to bed at the same time as you do other days. Take scheduled walks. Get sunlight early in the day. Reduce blue light for an hour before bed. Stay connected with other people in meaningful ways, despite being physically distant. Even small daily rituals can help, says Tricia Hersey, the founder of a nap-advocacy organization called The Nap Ministry. Light a candle. Have a cup of tea in a specific place at a certain time. “Repetitive rituals are part of what makes us human and ground ourselves,” she told me. They’re also perhaps the most attainable intervention there is. Wherever you are, Hersey says, “you can daydream. You can slow down. You can find small ways to stop and remember who you are.” To her, feeling in control over sleep is important precisely because order is lacking in so many other parts of life for so many people. Year over year, there are significant sleep disparities across the U.S. population. The amount and quality of sleep we get depends on our environment as much as, if not more than, our personal behavior. Socioeconomic status and quality sleep chart on parallel lines. The most effective way to improve sleep is to ensure that people have a calm and quiet place to rest each night, free of concerns about basic needs such as food security. The pandemic has brought the opposite assurances, exacerbating the uncertainties at the root of already-stark disparities. As the quest for sleep falls only more to individuals, many are left to think outside the box. That has included, for some, dabbling in hypnosis. Not the kind of hypnosis where you’re onstage and told to act like a chicken, but a process slightly more refined. Christopher Fitton is one of a number of hypnotherapists who have spent the pandemic creating YouTube videos and podcasts meant to help put people to sleep. Fitton’s sessions involve 30 minutes of him saying empowering things to listeners in his pleasant, semi-whispered voice. He tells me he is now getting more than 1 million listens a month. Hypnotherapy is meant to slow down the rapid firing of our nerves. Similar to guided meditation or deep breathing, the intent is to stop people from overthinking and allow sleep to happen naturally. As you listen to Fitton saying banal things about the muscles in your back or asking you to envision a specific tree in a specific place, “the aim is to get into a relaxed, trancelike state, where your subconscious is open to more suggestion,” he says. Then, when he tells you to sleep, your brain is less likely to argue with him about how you’re too busy, or how you need to worry more about why someone read your text message but didn’t reply. Hypnotherapists such as Fitton provide tools to ground yourself, ultimately in pursuit of being able to do it unassisted, sans the internet. (It’s better not to bring your phone into your bedroom anyway.) Focusing involves practice; the trancelike state rarely happens easily, and no single way works for everyone. Some experimentation is usually needed. Apparently it still is for me. While listening to one of Fitton’s recordings, I couldn’t fully escape the image of him in his home office speaking softly into his microphone, reading an ad for Spotify, just as alone as everyone else. But regardless of whom you trust to help relieve you of consciousness, now seems like an ideal time to get serious about the practice. Draw boundaries for yourself, and sleep like your life depends on it. Hopefully it won’t. from https://ift.tt/3ph7Cht Check out http://natthash.tumblr.com For a fraction of people, getting these first COVID-19 vaccines could be unpleasant—more than the usual unpleasantness of getting a shot. They might make you feel sick for a day or two, even though they contain no whole viruses to actually infect you. Both the Pfizer/BioNTech and Moderna vaccines are quite “reactogenic”—meaning they stimulate a strong immune response that can cause temporary but uncomfortable sore arms, fevers, chills, and headaches. In other words, getting them might suck a little, but it’s nowhere near as bad as COVID-19 itself. Reactogenicity happens to some degree with all vaccines and is not in itself a safety concern. Vaccines, after all, work by tricking the body into thinking it has been infected, and these “symptoms” are an indication it has successfully done so. The fever, fatigue, and other signs we associate with colds or flu or even COVID-19 are typically caused by our immune responses, not the virus itself. “A reactogenic vaccine is not the same thing as an unsafe vaccine,” says Saad Omer, a vaccinologist and the director of the Yale Institute for Global Health. Compared with existing vaccines, the two COVID-19 ones from Pfizer/BioNTech and Moderna are a little more reactogenic than flu vaccines but are roughly on par with the shingles vaccine, which can interfere with daily life for a couple days in some people. (Moderna’s also seems to be a little more reactogenic than Pfizer’s, possibly because it’s a larger dose.) These vaccines have enough of a kick that the CDC suggested hospitals stagger vaccinations among staff, so an entire unit isn’t out on a given day. Nursing homes as well are concerned about vaccinating all staff and residents at once, which could reduce staff availability at the same time residents need more care. As the United States embarks on its largest, most complex vaccination campaign in history, experts say vaccine providers need to set expectations for people getting the shots. If someone who gets a vaccine is unpleasantly surprised, they might not come back for a second dose or their experience might sway their friends and family against it. Managing expectations is about making sure that Americans are willing to get the vaccine. “There has to be pretty good transparency about what you’re going to experience,” says Deborah Fuller, a microbiologist and vaccine researcher at the University of Washington. The sore arms, fevers, and headaches are a result of innate immunity, the first of the immune system’s two main branches. Innate immunity is a blunt tool; it wants to fight anything foreign. When you get a COVID-19 vaccine, the cells in your arm take up mRNA that encodes a version of the coronavirus’s spike protein. The virus uses spike protein as a key to get into our cells, but unattached from the rest of the virus, the spike protein can’t infect anything. Still, the innate immune system recognizes the vaccine materials and the resulting spike protein as foreign. This signal sets off a reaction that can feel a lot like getting sick. More immune cells get recruited to your arm, which may become inflamed and sore, activating even more immune cells that might cause whole-body symptoms such as fever and fatigue. Some of those immune cells will belong to the second branch of the immune system, adaptive immunity. These are the targeted assassins of the immune system. They include B cells, which make antibodies that can bind to the spike protein and T cells that can recognize infected cells. Adaptive immunity is what will specifically protect you from COVID-19. And to get there, you first need the innate immune system to recognize the foreign protein and turn on the adaptive immune system. A reactogenic vaccine isn’t necessarily a more effective vaccine, but it is a sign that the first step is working. Reactogenicity is also distinct from anaphylaxis, a severe allergic reaction that has occurred in a handful of people getting the Pfizer vaccine in the U.S. and the U.K. Anaphylaxis is an immune reaction as well, but it begins within minutes after exposure, with dramatic drops in blood pressure and difficulty breathing. It’s still unclear what in the shots triggered an allergic reaction, though the vaccines contain sugar as a cryoprotectant and salts to get the right acidity, in addition to the active ingredients. The CDC recommends 30 minutes of observation after COVID-19 vaccination for anyone with a history of anaphylaxis and 15 minutes for everyone else. Anaphylaxis is very treatable with epinephrine (a.k.a. an EpiPen) and antihistamines, and the vaccine recipients who experienced it have all recovered. The CDC and FDA have a vaccine adverse-events monitoring network that will scrutinize anaphylaxis as well other possible serious and longer-term side effects. These side effects are all different from normal and common reactogenicity, which should last only a couple days. The reactogenicity of the mRNA vaccines from Pfizer/BioNTech and Moderna is likely largely due to the bubble of fat used to package the mRNA. These bubbles, called lipid nanoparticles, seem to stimulate the immune system in animals even when empty. In the past, vaccine makers sometimes have added a second ingredient to a vaccine, called an adjuvant, to enhance the immune response. The lipid nanoparticle, originally designed to protect the mRNA and smuggle it inside cells, just happened to act as an adjuvant as well. “It’s like a three-in-one package,” Fuller says. Lipid nanoparticles are an active area of innovation for designing future mRNA vaccines, of which Pfizer/BioNTech’s and Moderna’s are the first two. The COVID-19 pandemic finally validated the years of expectations about the technology. When I spoke with Drew Weissman, a mRNA vaccine pioneer at the University of Pennsylvania, not long after the first clinical trial results that proved how well these vaccines worked, he was optimistic about the future of mRNA vaccines. The technology could be applied to improve existing vaccines, such as for the flu, and make new ones against other diseases or even cancer. His one note of caution was on reactogenicity. “We’re working on ways of reducing that,” he told me. “I’m not sure people will tolerate it for influenza vaccines or other vaccines.” For context, less than half of adults in the U.S. got the flu vaccine last year. But COVID-19 on the whole is much worse than the flu. It’s already killed more than 300,000 Americans this year, compared with the 60,000 who die from the flu in a very bad year. And even for people who recover, illness from the coronavirus can last much longer and feel much worse. A sore arm or fever for a day, in contrast, might not be so bad. from https://ift.tt/3mAtUsW Check out http://natthash.tumblr.com This week, American health-care workers started receiving their first doses of a new COVID-19 vaccine. Early data have shown that the Pfizer/BioNTech vaccine is safe and highly effective, reaching 95 percent efficacy about a week after the second of two doses. The second COVID-19 vaccine under evaluation for use in the United States is expected to receive an FDA emergency use authorization as soon as tomorrow. COVID-19 vaccine doses won’t arrive in many U.S. nursing homes until next week or the week after that, but a few residents in West Virginia and Florida got their first shot this week. While staff and residents in nursing homes and other long-term-care facilities wait for doses to arrive, 863 more U.S. facilities reported outbreaks than in the previous week, and known cases of COVID-19 in long-term-care facilities are high and rising. Vaccinations in these facilities have the potential to save tens of thousands of lives over the next few months: In the past seven days, states reported more than 5,000 deaths linked to long-term-care facilities. In the United States as a whole, cases rose only slightly this week (Thursday, December 10, through Wednesday, December 16) compared with the previous week’s numbers, which included Thanksgiving reporting backlogs. Hospitalizations continue to climb, and deaths are rising across the country, reflecting the high cases and hospitalizations we’ve seen since early November. For the second week in a row, more COVID-19 deaths were reported in the United States than at any other time in the pandemic. Yesterday alone, states and territories reported 3,400 COVID-19 deaths, 24 percent more than were reported on the worst day of the spring surge.
Our count of U.S. COVID-19 deaths currently stands at 298,823, and will almost certainly reach 300,000 this week. It’s worth noting that from March through early November, when official COVID-19 deaths remained well under 250,000, at least 350,000 more people died than usual in the United States. A quarter of those “excess deaths” were officially attributed to causes other than COVID-19, but may actually have been due to the virus. The New York Times offers a close look at where deaths are above normal in the United States. These COVID-19 deaths haven’t affected all Americans equally. As of this week, U.S. states report that more than 50,000 Black people have died of COVID-19. As stark as this number is, it’s also an undercount, in part because for more than 20,000 U.S. COVID-19 deaths reported to date, no racial or ethnic demographic data were reported. Since the beginning of the pandemic, the data have shown that Black people have been much more likely to die than white people in the same jurisdiction. In Washington, D.C., where the known disparity is the most extreme, Black residents have been more than six times as likely to die from COVID-19 as white residents. Nationwide, if these disparities did not exist—if Black people were only as likely to die of COVID-19 as white people are—more than 22,000 Black Americans would still be alive.
At the national level, the good news this week is that cases haven’t risen that much above last week’s big increases—but at the regional level, the story is more complex. Before Thanksgiving, we predicted that case, test, and death reporting would be compromised by the holiday, first dropping during and immediately after the holiday weekend, and then rising sharply as backlogs resolved. We think tests and cases have now largely recovered from this period of erratic reporting. Death reporting is a complex—and much lengthier—process that often results in backlogs that are opaque to members of the public, and it’s less clear that the death-reporting backlogs related to the holiday have been completely resolved. With Christmas a little over a week away and New Year’s Day a week after that, we are now heading into a doubly disruptive period in COVID-19 data. The actual patterns present in cases and deaths will eventually become clear when complete reporting by symptom onset and date of death becomes available from federal data sources, but through mid-January at least, we should view the daily and weekly movements in the data with extra caution. We also strongly recommend not relying on test-positivity calculations during this period, when reported cases and reported tests are likely to be even less synchronized than they usually are. Hospitalizations remain the sturdiest metric through periods of reporting disruption. States reported that a little over 113,000 people were in the hospital with COVID-19 yesterday. For comparison, hospitalizations in the spring and summer surges peaked at just under 60,000 people. Regionally, hospitalizations are continuing to decline in the Midwest, but they’re rising everywhere else in the country. If current hospitalization trends continue, the Northeast’s rising numbers will soon cross the Midwest’s declining ones.
This regional pattern is mirrored in new reported cases per capita. In the Midwest, cases have declined more sharply than hospitalizations, and this is an expected pattern, as hospitalizations trail behind cases. Case rises may be reaching a plateau in the Northeast and are unambiguously rising in the South and West.
In much of the country, cases appear to be flat or falling compared with last week’s case numbers—which, again, we believe to have been unusually high due to holiday backlogs being resolved. Even on the heels of last week’s very high numbers, 19 states are seeing more cases reported this week than last, and 13 states are reporting case numbers at least 5 percent higher than last week’s.
The biggest case increases by percentage this week were in Tennessee, California, and Hawaii, but the scale of outbreaks throughout California far exceeds those of every other state. There are nearly 16,000 people in the hospital with COVID-19 in California, which reported more than 250,000 cases just this week.
California’s regional outbreaks vary dramatically in severity. According to the Los Angeles Times, Southern California has reached 711 new cases per 100,000 people in the past seven days—more than double the Bay Area’s number—and Los Angeles County alone has reported more than 91,000 new cases in the past week. Los Angeles County has a population of more than 10 million people, slightly more than the entire state of Michigan, and according to health officials, one in 80 people in the county has COVID-19 this week. The county’s director of health services said this week that its hospitals are “under siege,” and on average, two county residents are dying of COVID-19 every hour. The virus is now spreading most quickly in suburban counties in Southern California, where the L.A. Times reports that since the week of Thanksgiving, COVID-19 hospitalizations have doubled in Los Angeles, San Diego, Orange, Riverside, San Bernardino, and Ventura Counties. Orange County is building field hospitals to accommodate the spike in COVID-19 patients, and the number of cases in the county’s jails have jumped from 74 to more than 400 in a single week. California Governor Gavin Newsom said on Tuesday that the state has ordered an additional 5,000 body bags and has 60 refrigerated storage units on standby to accommodate an expected rise in deaths following on the state’s soaring case counts and hospitalizations. Arizona, a state hit early and hard in the summer’s Sun Belt case surge, now has the second-highest number of people hospitalized per capita. One hospital system in Arizona reports that it expects to reach 125 percent capacity tomorrow. Along with Arizona, 11 other states have now reached 300 COVID-19 hospitalizations per million people in at least two different stages of the pandemic. Louisiana has now reached this alarming level of hospitalizations in each of the country’s three surges to date.
At the very top of the list, however, is Nevada, which has nearly 600 COVID-19 hospitalizations per million people. If we look closely at Las Vegas hospitals in the hospitalization data set published by the U.S. Department of Health and Human Services, we can see that many of them have very high ICU occupancy rates, which implies a high level of strain on the health-care system. Nevada’s overall hospital-occupancy rates have been rising alongside California’s, but they began higher and they have stayed higher.
In the Northeast, Connecticut, New Jersey, and Rhode Island are all reporting COVID-19 hospitalization rates of more than 300 per million people, and Rhode Island is now reporting hospitalizations well above its spring peak. In New York, Governor Andrew Cuomo has ordered hospitals to shift to “crisis management mode” ahead of an expected surge in hospitalizations. Massachusetts Governor Charlie Baker said that COVID-19 hospitalizations in the state have increased by 93 percent over the past three weeks alongside a 73 percent rise in the number of patients in intensive-care units, and urged residents to avoid holiday gatherings. Florida is reporting more than 5,100 people hospitalized with COVID-19 in the state this week, slightly more than half the number of people hospitalized during the state’s summer surge. Last week, we wrote about a new data set from the Department of Health and Human Services that reports facility-level information on COVID-19 hospitalizations and hospital capacity across the United States. We are continuing to explore these data alongside the numbers we compile from states, and this week, the federal data show that in many states, a large number of facilities have almost no ICU beds available. In Oklahoma, 65 percent of hospitals have 10 percent or fewer open ICU beds. Many of these facilities are small, and as their limited capacity fills, the burden on larger regional hospitals will increase as they are forced to take on patient overflow. Nicki Camberg, Alice Goldfarb, Erin Kissane, Alexis Madrigal, Jessica Malaty Rivera, Sara Simon, and Peter Walker contributed to this report. from https://ift.tt/3gW2H2G Check out http://natthash.tumblr.com Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. Back in the spring, before the first surge of the coronavirus had fully diminished, public-health experts were already warning of a second surge. Shutdowns were ending and public spaces reopening, but as the months turned cold, they said, cases could spike again—more dramatically, even, than in the first wave. The reprieve after the first wave, though, was short: By June, case numbers were climbing again. As northerners were headed outside, southerners were headed inside, where the virus spreads most easily, and the country’s summer surge began. By this way of looking at the pandemic—the increases, dips, and plateaus in case numbers on a national scale—the United States is in its third surge. Cases, hospitalizations, and deaths all peaked and then subsided first in April and again in August. When the current surge will peak is not yet clear. Another way of looking at it takes into account the pandemic’s patchwork spread. At the state level, only one state, Louisiana, has suffered three major surges. In some of the places hit worst in the earlier surges, November and December mark the virus’s first resurgence. In New Jersey and Connecticut, hospitalizations are climbing again to levels not seen since spring, and in Arizona and Texas, they are as high as they ever were. This chart shows the states where hospitalizations hit at least 300 people per million in at least two nonconsecutive weeks, according to data from the COVID Tracking Project at The Atlantic. This level of hospitalization is a good measure of the pandemic’s local severity, both because it captures serious cases that aren’t limited to deaths and because hospitalization data are reliable over short time frames (unlike data for cases and deaths, which can be delayed by weekends and holidays). This cutoff, 300 per million, is somewhat arbitrary, but it captures the states that have generally suffered the most during the pandemic. 
Using this measure, the beginning of the pandemic, when the dimly understood novel coronavirus spread rapidly through the East Coast, shows up clearly. Illinois, Michigan, and Louisiana all had major outbreaks as well, generally centered on the metropolitan areas of Chicago, Detroit, and New Orleans. At the end of March, The New York Times reported that Louisiana had perhaps the fastest growth in cases in the world--2,305 cumulative cases through March 26—perhaps because of Mardi Gras. In Michigan, officials and experts pointed to deep poverty and lack of resources in the Detroit metro area to explain the disproportionate impact there: thousands of homes without water, high levels of multigenerational housing, few jobs in which residents can work remotely. Chicago faced similar problems. The initial surge swept first through the city’s Black communities; of the first 1,000 COVID-19 deaths in Cook County, half of the victims were Black, twice their proportion of the population. Again, local experts attributed the numbers to a combination of inequalities, including poverty, underlying health conditions, and struggling hospitals; the county’s massive jail was also the country’s worst COVID-19 hot spot in early April. [Read: The pandemic’s final surge will be brutal] As the problem in those states began to subside, hospitalizations were on the rise in the Sun Belt, from the South through the Southwest. Why was the problem worse in the Sun Belt during the summer? A few theories have been suggested. First, the rise coincided with business reopenings across the region. Places hit harder early on were slower to reopen; across the Sun Belt, by contrast, states went through what Alexis Madrigal and Robinson Meyer call “all or nothing” reopenings. Second, the Northeast and the Midwest are often unpleasant outside in the early spring and lovely during the summer, while the reverse is often true in the Sun Belt. In that last week of June, “America lost control of the pandemic,” as Meyer wrote at the time, and 16 states hit their highest case counts, most of them Sun Belt states. Now the situation is much worse than that awful week. Of the 12 states that have exceeded 300 hospitalizations per million twice during the pandemic, all 12 were above that threshold during the week of December 6. Louisiana is above that threshold for the third time this year—it suffered through the first round of uncontrolled community spread, then through the Sun Belt surge, and again through the winter surge. Half of those 12 states have higher hospitalization rates now than during their first surges. In the first few months of the pandemic, the virus came in waves, rising in one place, falling in another. Now it’s rising almost everywhere. With federal assistance drying up, improvement in the unemployment rate slowing, and consumer spending down, states and municipalities have been slow to go through another round of shutdowns. Nowhere in the country has the virus ever been truly driven back; when the conditions were right, it surged again. from https://ift.tt/34nljUf Check out http://natthash.tumblr.com The pandemic has brought unprecedented suffering and yet, Congress hasn’t passed new relief since March. As politicians attempt to negotiate a package before the holidays, Americans are going hungry. What about our politics let the situation get so bad? On this episode of the podcast Social Distance, staff writer James Hamblin and executive producer Katherine Wells talk with Luis Guardia, the president of the Food Research & Action Center, and the Atlantic staff writer David A. Graham. Listen to their conversation here: Subscribe to Social Distance on Apple Podcasts, Spotify, or another podcast platform to receive new episodes as soon as they’re published. What follows is a selection of their conversation with Guardia, edited for clarity: Katherine Wells: What was the situation with hunger in this country before the pandemic? Luis Guardia: We’ve certainly had a hunger problem before, though a lot of it remained unseen. There are a lot of misconceptions about who is hungry. And when COVID-19 hit, I think everybody was shocked to see how quickly things changed. Those hunger numbers just went through the roof really quickly. We’ve gone beyond this notion of being food-insecure—in the sense of not knowing where the next meals were going to come from or [whether] they’re going to be enough. People actually started disrupting their meal patterns. People actually went hungry. Or if they didn’t go hungry, they had to make the tough decisions about maybe not paying the rent, or maybe not paying their medical bill, or maybe not paying the utility bill. The problem had come home to roost in a very sharp and incredibly fast way that we were just not anticipating. Wells: What kind of resources are available for people? Where do people go, and are those systems functioning? Guardia: Unfortunately, we just haven’t had the leadership necessary to deal with food insecurity in a comprehensive way in this country. We all remember, early on in the pandemic, seeing the incredible images of miles of cars queued up outside of food banks. The food banks were quickly overwhelmed and remain overwhelmed. There is still significant demand, but what’s heartbreaking for us at FRAC was knowing that there are solutions at hand like SNAP, the Supplemental Nutrition Assistance Program. We know from working with our friends at Feeding America, that for every one meal the Feeding America network provides, SNAP provides nine. Wells: Is the problem that there aren’t the resources or that they’re just not getting to people? Guardia: They need to get to people, but they also need to be increased. We know SNAP does not provide enough for people to buy a robust, nutritious diet. We know that a lot of people on SNAP have to make hard choices about stretching out those food dollars. That’s why boosting the SNAP benefit is so critically important. The government did this very quickly in response to the Great Recession in 2008–2009. The SNAP maximum benefit amount was increased by 13 to 14 percent. What we’ve been calling for is an increase of about 15 percent. James Hamblin: You became head of the Food Research & Action Center just before the pandemic started and have seen food insecurity increase and SNAP not meaningfully increase. What’s it been like? Guardia: It has been exasperating. We know SNAP is effective. It rides the regular wheels of commerce. It provides a tremendous amount of work, convenience, and greater dignity for people to access food. And as economists are scratching their heads about how [we can] get the economy going again with fiscal stimulus tools, SNAP is one of the most effective stimulus tools there is. We know that for every $1 of benefit in SNAP, the economy grows $1.50 to $1.80. That’s a pretty good return on investment. Hamblin: And why should we even have to make that argument? “It’s a good investment to have people have food”? I understand that’s the language of Washington, but it’s kind of weird that we have to do that, right? Guardia: It’s a little bit disheartening, but we always use every tool in the toolbox. We’re hearing some positive language come from the Biden-Harris team. We’re hopeful that they can step up and show some leadership on this. from https://ift.tt/3mzHA7L Check out http://natthash.tumblr.com Jimbo Livaditis has sold Christmas trees through wartime and peace, recessions and booms, disasters both local and national, and the rapid advancement of fake-tree technology. He has been in the business his whole life, spending his childhood Decembers running around the parking lot of his family’s Atlanta ice-cream shop, where his dad—the eponymous Big John of Big John’s Christmas Trees—had started selling trees in 1949 to offset slow winter sales of frozen treats. He went to work on the tree lots with his siblings as a teenager in the 1970s, and in 1987, he and his brother took over the company. In all those years, he has never seen people jonesing for Christmas trees the way they have this year. “I hate to overuse the word unprecedented,” Livaditis told me. “But it is exceptional.” By last Wednesday, Big John’s had already closed five of its nine lots because the company was simply running out of trees. “We usually sell right up until December 22 or 23,” Livaditis said. “Shutting down any of our lots this early is something that will go down as an historic event in our 71 years of operation.” After selling what he described as a “surreal” number of trees on Black Friday, Livaditis put out feelers to friends in the industry everywhere from Northern California to South Florida, looking for more stock to truck in, to no avail. He kept hearing the same thing: Sellers in every corner of the country were going through Christmas trees almost as fast as they could get them off the truck. There appears to be a run on Christmas trees. Over the past two weeks, the media have started to pick up on the apparent frenzy, but putting numbers to these observations is a little tricky because the industry is almost charmingly low on data. There are no flashy start-ups peddling Fraser firs via app—a Christmas miracle! Google Trends, which tracks what people search for over time, shows a higher and more sustained interest in real Christmas trees this year than any before it, but the large majority of the 25 million fresh trees bought annually are sold through small, local businesses such as Big John’s, making any understanding of how a season is going nationwide a mostly anecdotal one. Anecdotally, though, business is booming, even in an economically scarred country. During the pandemic, Americans have emptied the shelves of all kinds of products. Flour, jigsaw puzzles, dumbbells, inflatable pools, ring lights, peel-and-stick tile, antacids—all have seen their inventories depleted as people think of new things that might help them feel better and pass the time. Now, as coronavirus cases tick up, federal aid bottoms out, and the country sorts out the aftermath of a contentious election, far more people than usual seem to have looked around their home and decided that, well, maybe a little bit of holiday cheer would feel nice, and it would also be something new to do. If they can’t have all the grander things they might need right now, then what they want is to decorate the hell out of a Christmas tree. A rush on Christmas trees wasn’t a foregone conclusion. As with many of the pandemic’s hot commodities, it wasn’t clear what people might find compelling about this holiday season, and what they might dismiss as too much work, until they were already peppering tree merchants with preorders. “We were just preparing for the worst, thinking we might not sell any trees, or we might get shut down” in tightening pandemic restrictions, Julian Tempesta, who runs Vermont Christmas Trees, told me. The company operates two tree lots in wealthy Brooklyn neighborhoods, where many residents have second homes. Without an opportunity to throw the lavish Christmas parties that typically motivate such buyers to get their trees early, Tempesta worried that this year might be a bust. “We were shooting for like 75 percent of our typical sales,” Tempesta said. If some of those residents did abscond to country homes, those who stayed in town have more than made up the difference; both his lots have sold out multiple times. All season, that slowdown never came. In Atlanta, Livaditis’s customers started preordering trees in September, weeks earlier than they usually do, but that didn’t dent walk-up sales to his lots at all. Even his corporate clients, many of whose employees are working from home, still ordered trees for their offices, including a 30-footer for the lobby of Georgia-Pacific’s headquarters. “We’re at a pretty good pace of driving to the city, dropping off trees, coming home, cutting more, and driving to the city to drop off trees,” Galen Parke of Adam Parke Trees, Tempesta’s supplier in Vermont, told me. When I called him, he warned me that the signal might drop—he was in the truck, driving through rural New England once again, hoping the strong demand didn’t suddenly dry up. If anything, sellers usually have the opposite problem: Because Christmas trees take a decade or so to reach maturity, low planting rates during the Great Recession have constrained current supply. In a normal year, it’s still enough to meet demand, but little about this year is normal. [Read: The Christmas-tree shortage could last for years] One reason that trees are selling so fast this year is simple math. When a holiday usually centered around gathering becomes fragmented, it loses its economies of scale. People still want to celebrate the same way; they just have to do it in smaller, more numerous groups, each of which requires its own supplies. The looming run on Christmas trees was foretold by the apparent boom in Thanksgiving turkey sales. Urged to reduce the size of their gatherings and avoid travel, many Americans did just that, but many still had traditional Thanksgiving dinners—they just had more of them. A family that gathers 16 people for the holidays in a normal year might split that out into four celebrations of four people during the pandemic, which means up to four smaller turkeys instead of one big bird. Or, now, four trees instead of one big one that everyone travels to sit around together. This month, I found myself planning exactly that sort of dispersed Christmas. I always fly home to Atlanta for the holidays, so I had never bought a tree, real or otherwise, until two Sundays ago, when I dragged my folding grocery cart several blocks to the store near my Brooklyn apartment, selected a nearly five-foot-tall fir, and wheeled it home, full of the type of pure-hearted Christmas joy I had not experienced since childhood. On the way out, huge sidewalk shelving racks meant to hold miniature and tabletop trees stood bare, their voids telling of all the little Christmas trees that had been spirited away to tiny apartments occupied by young transplants who usually head out of the city for the holiday. In the week and a half since I got my tree, I have traipsed miles around the city on foot, looking for things with which to adorn it—multicolored lights, a topper star covered in chunky gold glitter, an ornament that bears a striking resemblance to my Chihuahua in a red Christmas tutu, a tree skirt accented with jingle bells to prevent said Chihuahua from drinking the tree water. And, like, sure: Why not Christmas trees? After nine months of pandemic purgatory, some of the Christmas enthusiasm is likely attributable to practical desires: People need something new and fun to do, and picking up and decorating a Christmas tree will give a family at least a day of wholesome entertainment with a joyful payoff. People want to “have something new and pleasant to think about, especially this year, after being at home with your family for so long, and everyone’s staring at each other,” Leigh Anne Livaditis, Jimbo’s wife and business partner, told me. “People want to decorate the house and change things up and have a new project. I think that’s why they came so early this year.” [Read: Americans have baked away all the flour] But Christmas trees aren’t necessarily selling just because many Americans are cooped up at home all day. Their existence is emotional: satisfying tradition, marking time, standing as a symbol of familial love and goodwill. If you’re in the business long enough, Livaditis told me, you see that sales are affected more by emotional circumstances than by practical ones. Before this year, the biggest spike in sales he could remember was in 2001, when the country was also coming to terms with a singular national tragedy. Then, as now, people seemed to see Christmas as a time for both hope and remembrance. “It’s celebratory, but in a different way,” Livaditis told me. “It’s like celebrating somebody’s life when they pass.” Christmas is a rare time in which much of the country goes idle for a day or two, allowing most people to focus on what they hold dear. In a year of unrelenting stress and pain, a lot of people have grabbed the opportunity to pause—and the tree that symbolizes it—with both hands. Livaditis told me that he felt lucky to be able to contribute to people’s Christmases every year, but especially this year. The early mad dash for trees has given a little bit of psychological relief to a lot of families and provided the physical centerpiece for millions of little pandemic Christmases. “I enjoy Christmas-tree season more than anything,” Livaditis said, “even though we’re the host of the party that we never really get to enjoy, per se, because we’re hosting.” This year, though, things look a little different. The day after he and I spoke, the company closed three of its remaining four lots because of dwindling inventory. On Monday, it announced that its final location, in the parking lot of the ice-cream shop, would close for the season this afternoon. For Livaditis’s family, the Christmas-tree rush has also provided a very rare blessing: an opportunity to have a real, restful holiday together, for the first time in a generation. from https://ift.tt/34jz3zo Check out http://natthash.tumblr.com Editor’s Note: The Atlantic is making vital coverage of the coronavirus available to all readers. Find the collection here. With the FDA’s emergency authorization of the first COVID-19 vaccine imminent, the biggest and most complex vaccination campaign in the nation’s history is gearing into action. Planes are ferrying vaccines around the country, hospitals are readying ultracold freezers, and the very first people outside of clinical trials will soon get shots in their arms. The end of the pandemic is in sight. But vaccines are not an off switch. It will take several months to vaccinate enough Americans to resume normal life, and this interim could prove long, confusing, and chaotic. The next six months will almost certainly bring delays in vaccine timelines, fights over vaccine priority, and questions about how immune the newly vaccinated are and how they should behave. We’ve spent 2020 adjusting to a pandemic normal, and now a strange, new period is upon us. Call it vaccine purgatory. The biggest unknown is how long we will be left in purgatory. Operation Warp Speed officials have laid out an aggressive timeline to get nearly all Americans vaccinated by June, but this presumes several pieces going perfectly. The vaccines from Pfizer, which was just recommended for FDA authorization, and Moderna, which is expected to follow next week, cannot hit manufacturing delay, and additional vaccine candidates, from AstraZeneca and Johnson & Johnson, must earn speedy authorization from the FDA early next year. Pfizer earlier revised down the number of doses it will deliver in 2020 and separately has said it cannot supply any additional doses to the U.S., beyond the 100 million already ordered, before June. The timeline for authorizing AstraZeneca’s vaccine is up in the air after a messy clinical trial. And Johnson & Johnson’s has not yet been proved to work. [Read: The vaccine is here. Now for the hard part.] Your experience of this purgatory may depend on where you live. While a CDC committee sets recommendations of how to prioritize initially scarce doses, each state ultimately decides how to allocate the vaccines it receives. A person who qualifies as an essential worker in Illinois might not in Indiana. One city could end up opening vaccinations to the general public before its neighbor. This system is meant to be local and flexible, but that will necessarily mean a patchwork of policies that could come off as unfair or inconsistent. “It is such a complicated and large logistical challenge that a lot of things will go wrong. A lot of things will not go to plan,” says Eric Toner, a senior scholar at the Johns Hopkins Center for Health Security. “The important thing is not to get hung up on that.” Hard trade-offs are ahead, as many groups have some claim to priority but they by definition cannot all be prioritized. Toner says not to lose sight of the ultimate goal: “Let’s just keep vaccinating people.” The decisions still being made about how to prioritize vaccines will dramatically color individual people's experiences over the next months. But ultimately getting out of purgatory will require reaching herd immunity, which is something we can only achieve collectively. Vaccines can protect individuals, but vaccination as a public-health strategy protects a community. Every person who gets vaccinated is a small step toward herd immunity, toward bringing down the amount of circulating virus. Eventually, we can go all back to schools and dinner parties and concerts. I. Health-care workers and nursing-home residents and staffVaccines will do very little to change life for the average American in 2020. The very first Americans to receive COVID-19 vaccines will be health-care workers and residents of long-term care facilities. These priorities, set by the CDC’s Advisory Committee on Immunization Practices last week, are meant to preserve the health-care system and to save lives. People in long-term care facilities account for many of the hospitalizations and roughly 40 percent of U.S. COVID-19 deaths, according to data from the COVID Tracking Project at The Atlantic, even though only a small fraction of the country’s population—less than 1 percent—lives in these facilities. Because the first shipments of vaccines will not cover all 24 million people in these two groups, the CDC has recommended sub-prioritizations too. Hospital workers who are in contact with patients are first on the list—including janitorial and support staff. The CDC also asks hospitals to consider that people who have recovered from COVID-19 likely have some immunity, so they do not need to be vaccinated first, though they won’t be prevented from getting vaccinated when doses are available later. For long-term care facilities, the CDC recommends putting skilled-nursing facilities, which have the sickest patients, before assisted-living facilities. [Read: The vaccine is not coming soon enough for nursing homes] After vaccination begins, hospitals and nursing homes will not change overnight. Both the Pfizer and Moderna vaccines require two doses, three and four weeks apart, respectively, and even then the vaccines take time to build immunity—the companies measured 95 percent protection from COVID-19 symptoms only after one or two weeks. That will be well into 2021 for even the first people vaccinated this year. (The first dose may offer some protection after 10 days, but that likely wouldn't be as strong or long-lasting as the full regimen.) Scientists also do not yet have the data to confirm that the vaccines actually prevent people from spreading the coronavirus asymptomatically in addition to preventing COVID-19 symptoms. This is likely, but data on this won’t be available until early next year. For now, a vaccine can clearly offer some protection to the recipient—but that person can’t be fully confident that they won’t spread the disease to others. A nurse might feel safer at work but still worry about bringing the virus home to their family. Moreover, “even with a vaccine that is 95 percent effective, you don’t know if you are in the 5 percent,” Marci Drees, the infection-prevention officer at ChristianaCare and a representative on the CDC advisory committee, points out. Health-care workers who come in contact with COVID-19 patients will continue to need full personal protection equipment. Drees says she doesn’t anticipate any changes in PPE or quarantine-after-exposure policies in the near term. Slowly, though, small corners of the world could start to change. In nursing homes where every staff member and resident gets vaccinated—essentially reaching building-wide herd immunity—some restrictions could be loosened. Residents could increase their very limited socializing with one another. Jason Belden, the director of emergency preparedness for the California Association of Health Facilities, says the buildings might eventually open to some visitors, but symptom checks and masking will continue. With everyone inside vaccinated, the risk from unknowingly letting in a visitor who is infected is diminished, but not zero. States, hospitals, and nursing homes are still dealing with a lot of unknowns right now though. For one, Operation Warp Speed keeps changing the number of doses that will be initially available to each state. Kris Ehresmann, the director of the Minneasota health department’s infectious-disease division, told me that the numbers have changed so many times just in the past week, “I had this slide that I showed to the governor on Thursday. Then when I gave an update Monday, I used the same slide and had to cross things out. And I gave an update [Wednesday], and I crossed even more things out.” States also have no sense of how regularly shipments will come, so they are unable to plan beyond the first few weeks. Hospitals, for example, might be able to vaccinate only a quarter of their staff in the first wave. Without knowing more, they will then be unable to reassure their staff about when the rest will get the shots—will it be in one or four or eight weeks? This uncertainty is one of the biggest challenges for hospitals right now, says Azra Behlim, a senior director at the health-care-services firm Vizient. “There’s a little bit more panic when I don’t know when I’ll be getting anything else.” [Read: U.S. hospitals have passed the breaking point] The inclusion of nursing-home residents in the first priority group by the CDC advisory committee also came as a bit of a surprise to states, which did not expect it when they drew up vaccine plans earlier this year. The federal government has contracted with CVS and Walgreens to help vaccinate nursing-home residents, but this division of responsibility between the federal and state levels has also introduced confusion. Ehresmann says she’s been told to reserve some number of her state’s 183,000 initial doses for nursing homes, even though the nursing-home vaccination program also won’t be ready to start for a few more weeks. In California, Belden says, facilities in the association are still waiting to find out which ones will get how many doses when. “All of our members are reaching out every day. Am I going to be first? Am I going to be second? What's it going to look like? None of those questions have been answered,” he told me. “But I do suspect we'll get answers very soon.” Pfizer and Moderna expect to have 35 to 40 million doses of their vaccines ready by the end of the year, which is almost enough to cover hospitals and nursing homes at two doses per person. By early 2021, states will be getting ready for the next priority group. II. Essential workers and adults at risk for COVID-19In some ways, the very first group is actually the easiest to vaccinate. Health-care workers and residents of long-term-care facilities are relatively well-defined groups, and they are already concentrated in hospitals and nursing homes. “The real test will be what comes after that,” says Saad Omer, a vaccinologist and the director of the Yale Institute for Global Health. It only gets harder from here. The first hard choice is a stark one: Who should come next, essential workers, or adults over 65 or with comorbidities? The question boils down to which strategy to prioritize, Omer says: reducing transmission out in the community, by vaccinating essential workers interfacing with the public, or reducing deaths, by vaccinating the people most at risk of dying of COVID-19. The CDC advisory committee has indicated that it will recommend essential workers next, though the National Academies and the WHO have recommended the opposite. None of this guidance is binding. The decision is ultimately up to the states, though they have historically followed the CDC. Essential workers are also a nebulous category, and again, states get to set their own definitions. “There are an awful lot of interest groups that are lobbying states and lobbying feds to get their members or their constituents vaccinated sooner,” Toner told me. Should bank tellers count as essential workers? Teachers? Exterminators? And how should states prioritize different groups of essential workers? One study found that 70 percent of American workers can be defined as essential workers and 42 percent as frontline workers that directly interact with the public. The decision to prioritize essential workers also has to do with reaching working-class Black and Latino communities that have been disproportionately hit by the coronavirus. But these are the same communities that may be hardest to reach—because of distrust in the government and language barriers. As part of their vaccine planning, state health departments are planning to connect with churches, nonprofit groups, and other leaders in those communities. Without this effort, vaccines will go only to people who come asking for it. “The people who are capable of advocating for themselves in these situations are sometimes people who are less in need of the services than those who are not advocating for themselves,” says Kelly Moore, an associate director of the Immunization Action Coalition. These communities might take longer to reach, which means the overall vaccination might proceed a bit slower. There can be tension, Toner adds, between vaccinating as many people as quickly as possible and actually reaching priority groups. States and the CDC are still working out who will qualify as adults at high risk for COVID-19. Again, there’s a trade-off: Requiring proof will make getting the vaccines out harder, but forgoing it might mean someone who doesn’t strictly qualify gets a vaccine. “I don’t think we should get mired in documentation,” Toner said. “I don’t feel like they should have to show their medical record to prove that they’re diabetic. Or if they say they’re 65, but they’re only really 64, I wouldn't have them bring a birth certificate. I think to some extent, we would have to trust people.” III. The general publicFive months into the future, the plans get even fuzzier. When vaccines become available to the general public depends on a few unknowns. First, how many other vaccine candidates, like AstraZeneca’s and Johnson & Johnson’s, will actually also get authorized? These companies have already ramped up manufacturing, so doses can be ready to go as soon as the FDA gives the greenlight. Second, will they run into manufacturing delays? The mRNA vaccines from Pfizer and Moderna rely on a new technology that has never been used in an approved vaccine, let alone produced at the scale needed now. During manufacturing of the more routine H1N1 swine-flu vaccine during the 2009 pandemic, the U.S. ran out of “fill and finish” facilities that package bulk vaccines into vials. The government set up a program to prevent this bottleneck in the future, but other unforeseen snags may come up. The last stage of purgatory will be getting vaccines to the general public. Some parts of the country may allow everyone to get the vaccine sooner than others. In 2009, says Moore, who was running Tennessee’s immunizations program at the time, demand for the swine-flu vaccine in priority groups varied across the state. Some vaccine providers had doses for priority groups sitting unused, while members of the general public were asking about shots. Moore let those providers begin giving the vaccine to anyone who asked. This dynamic is very likely to play out between cities and between states with the COVID-19 vaccine, where doses are currently being allocated by census population but demand may vary. This decision is tough because it’s likely to be criticized either way. “Visualize the frustration … if Georgia and Tennessee and Alabama all have different groups being allowed to be vaccinated at different times. But if you don’t, if you try to make everyone in the whole country do these groups in lockstep, then you can imagine that that also is terribly unfair,” Moore says, if “there are lots of willing people who could be protected, and vaccine is being withheld.” Vaccine hesitancy is, of course, also a more general concern across the country. But Americans’ willingness to take a COVID-19 vaccine has risen as data on the vaccines’ efficacy has come out, and experts expect it to keep rising if early vaccination goes well. Many people have said they are more comfortable waiting a few months to get the vaccine, which is in effect what will happen. Eventually, our social lives can start getting back to normal. It won’t happen in a moment, but stepwise, in small ways and then larger ones. Omer says small gatherings like dinner parties and game nights might be safe if everyone in the group is vaccinated. School reopenings and mass gatherings will likely happen only when widespread vaccination—along with masks and social distancing through the winter and spring—pushes COVID-19 rates to low levels. Public-health experts stress that vaccines work in tandem with other measures: The start of a vaccination campaign cannot be an excuse to abandon the measures that are working right now. Moore likens vaccines to another slice on a pile of Swiss cheese, where each slice is an intervention that is by itself imperfect (masks, social distancing, even vaccines) but they drastically reduce risk when stacked together. Rochelle Walensky, President-elect Biden’s pick for CDC director, made this analogy on Twitter: “If I have a cup of water, I can put out a stove fire. But I can’t put out a forest fire, even if that water is 100% potent. That’s why everyone must wear a mask. As a nation, we’ll recover faster if you give the vaccine less work to do when it's ready.” There will likely be many frustrating and imperfect things about the vaccine rollout in the next few months. But the goal is to get the country—and, really, the world—back to normal, and that happens not when you as an individual are vaccinated but when enough people all over are vaccinated. It might take longer than we like, but we get there together. from https://ift.tt/2JYuFi6 Check out http://natthash.tumblr.com By nearly all measures, it has been a horrible week, a horrible month (10 days in), and a horrible year. The United States this week set records in all three metrics that gauge the pandemic’s severity, with a total of 1.4 million new cases and 15,966 deaths. Yesterday, states and territories reported 3,088 deaths from COVID-19--a record no one wanted to see—and the average number of deaths per day over the past 7 days exceeded 2,000, surpassing the highest average we saw in the spring’s deadly first surge. More than 106,000 people are currently hospitalized with COVID-19. 
If the patterns we’ve traced since the spring hold true, the worst is yet to come. Given the rapid increase in the number of new cases, we expect the metrics for hospitalizations and deaths to continue rising in the coming weeks—especially if in-person gatherings over Thanksgiving weekend led to increased spread of the coronavirus, as public-health experts warned would happen. A crucial bit of muddiness remains in the data themselves: Some of the reported deaths we are seeing now are likely related to the post-Thanksgiving backlog we’ve written so much about in the past couple of weeks. What’s not exactly clear is how many of these deaths are following the case increases that occurred before and during the holiday week. Either way, we expect that deaths will climb steeply given current case and hospitalization numbers. Test reporting, too, is probably still slightly low because of the holiday effect. Case numbers appear to be largely back online following the holiday reporting disruption, however, which makes sense—historically, case numbers have been quicker to recover from holidays and weekends than tests and deaths. Case numbers were high across the U.S. this week, with each of the country’s seven most populous states reporting more than 50,000 new cases among their residents. Fourteen states in regions across the U.S. reported a record number of cases this week; that’s on top of the 16 states that hit new-case records last week. 
The slowing case growth in midwestern states that we noted last week have continued: After the Thanksgiving data dip and subsequent rise, new cases appear to be declining in the region. Meanwhile, in the Northeast, South, and West, cases are rising sharply. After 14 weeks of North or South Dakota posting the highest per capita case numbers in the country, Rhode Island has taken their place, with 1,253 cases per million on the seven-day average. (The below chart, along with most of the others we use in our weekly posts, is available as a mobile-friendly interactive tool in the Charts section of our site.) 
With the catastrophic rise in cases, communities of color across the country have been especially hard hit by the terrible effects of the pandemic. In Rhode Island, more than one in eight Latino people has tested positive for COVID-19, compared with one in 31 white people. In both North and South Dakota, one in eight Black people has tested positive. Some of the highest per capita statistics are being reported for American Indians and Alaska Natives. South Dakota is reporting that one in seven Native Americans has tested positive for COVID-19. Notably, as case disparities between some other racial and ethnic groups have decreased in South Dakota, that has not been the case for Native Americans, for whom the weekly new cases reported per capita have been higher than for any other group, or the state overall, for the past three months. In surveying racial and ethnic disparities in other parts of the country, we also note that in Louisiana, one in six Asian people has tested positive for COVID-19. Hospitalizations rose in 26 states this week, mostly concentrated in the Northeast, South, and parts of the West. We believe these rising numbers indicate that outbreaks will continue to worsen in many of the country’s most populous states. Although the Midwest still has the highest per capita number of people hospitalized, the actual numbers there are falling; nine states in the region reported drops in the number of people hospitalized compared with last week. 
New Hampshire, Delaware, and Maine reported the largest percentage increases in COVID-19 hospitalizations in the past week, with California and New York right behind them. In California, the already high number of hospitalized COVID-19 patients rose 23 percent from last week; the state is reporting that, statewide, ICUs are 90 percent full. ICUs in Silicon Valley and parts of the Central Valley are full, and San Francisco, which long maintained relatively low case levels given the city’s density and population, now says it may run out of hospital beds in the coming weeks. In Los Angeles County, ICU and overall hospital capacity are running low, and a record 1,719 health-care workers in the county reported last week that they have COVID-19, more than double the number who reported they were sick the week before. The pandemic continues to play out in particularly distressing ways in long-term-care facilities. As our LTC team reported yesterday, a surge in cases in the Northeast and West continues; last week, both regions reported their highest numbers of new cases in the past six months. The Midwest and South saw a small downturn in new cases, which is promising, yet the week still saw the nation’s highest number of newly reported cases—51,574—in long-term-care facilities since the COVID Tracking Project began collecting these data in May. And, as we always note, these figures are an undercount, since not every state reports long-term-care data. Nearly 40 percent of the new cases in the Northeast came from Pennsylvania; the state reported more new cases of COVID-19 in LTC facilities than any other state except California, which has more than three times as many residents. Our researchers have been unable to obtain current data about the number of people living in Pennsylvania’s long-term-care facilities. But if numbers have remained relatively constant over the past five years, we can estimate, based on a 2015 number of residents in LTC facilities and available COVID-19 data from the state, that nearly 30 percent of people living in Pennsylvania LTC facilities have had COVID-19. And nearly one in five Pennsylvania long-term-care residents who has contracted the virus has died. Alice Goldfarb, Erin Kissane, Jessica Malaty Rivera, Charlotte Minsky, Joanna Pearlstein, and Peter Walker contributed to this report. from https://ift.tt/3acYMgP Check out http://natthash.tumblr.com |
Authorhttp://natthash.tumblr.com Archives
April 2023
Categories |
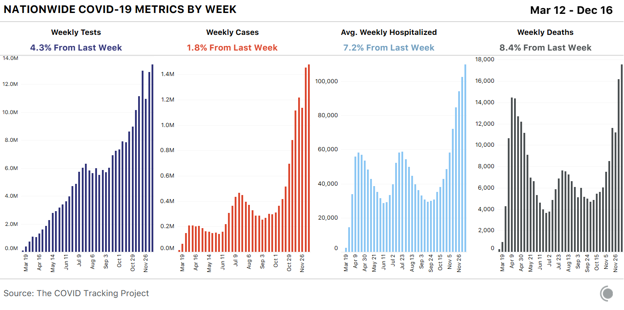
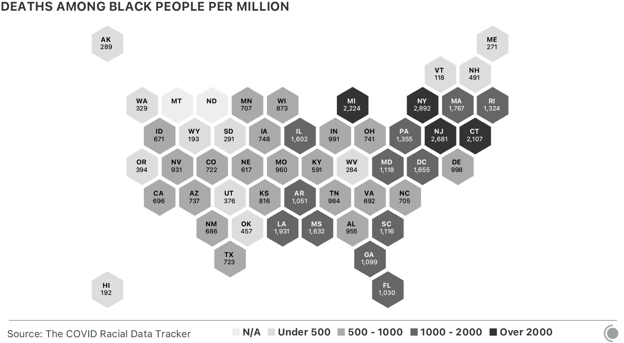
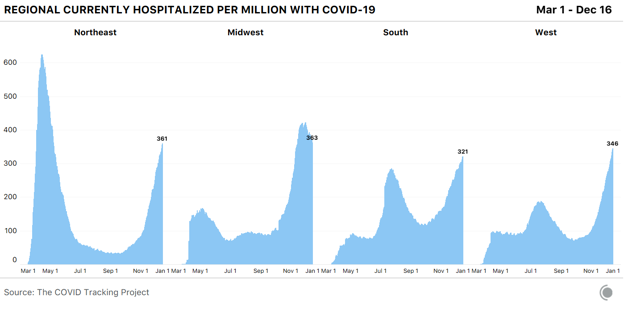
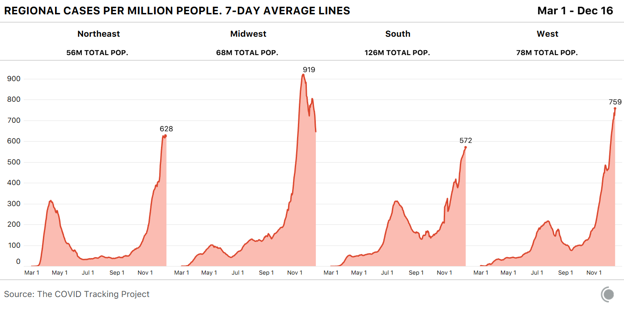
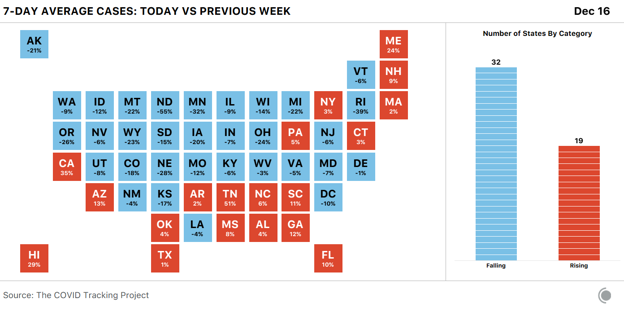
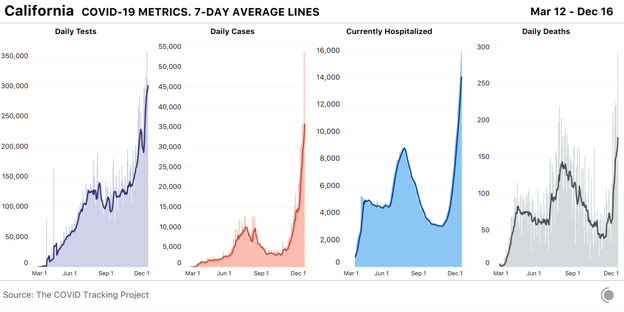
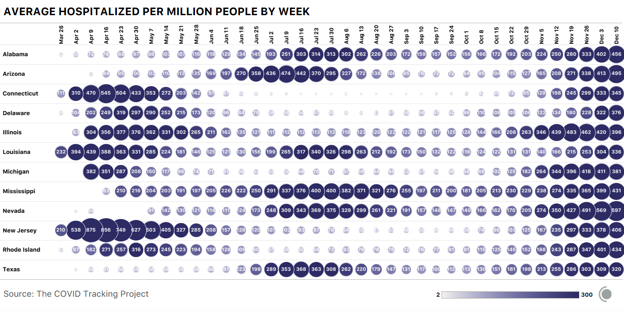
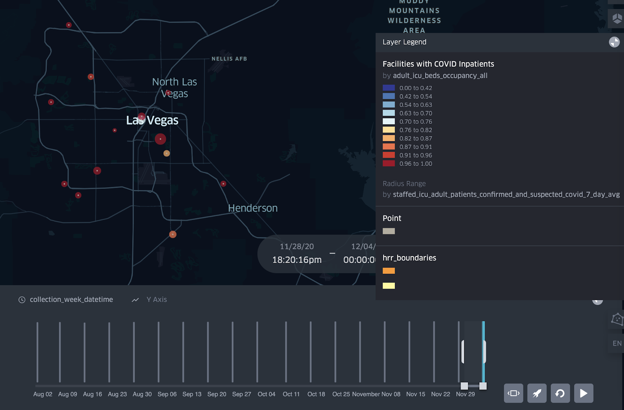
 RSS Feed
RSS Feed
